Burnout in Nursing Managers: A Systematic Review and Meta-Analysis of Related Factors, Levels and Prevalence

 , ,
, ,  , ,
, ,  and
and 
Abstract
:1. Background
2. Methods
2.1. Data Sources, String and Inclusion Criteria
2.2. Coding of Results
2.3. Data Analysis
3. Results
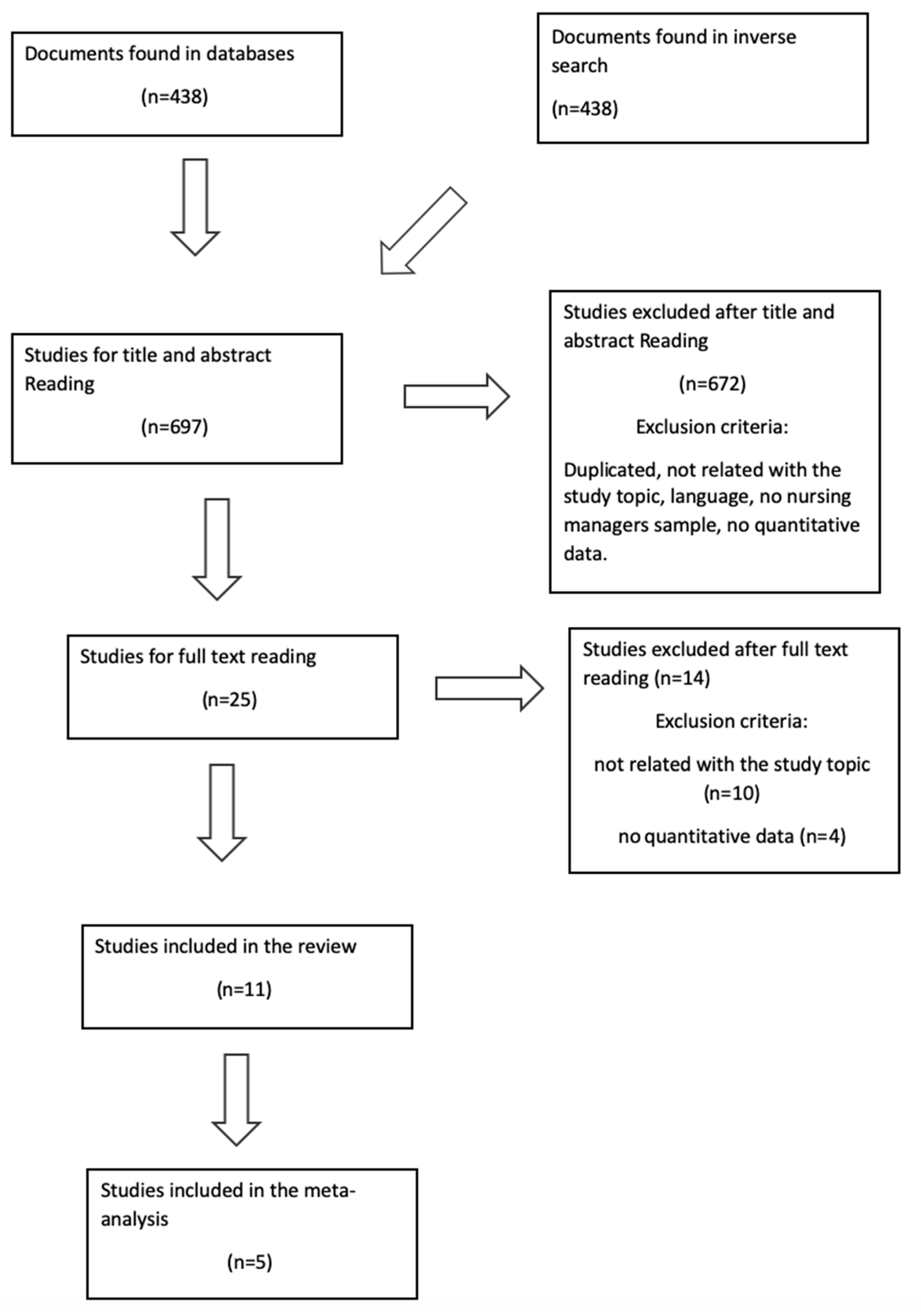
3.1. Search Description and Studies Included
3.2. Levels and Prevalence of Burnout among Nursing Managers
3.3. Risk Factors and Mediating Factors for Burnout in Nursing Managers
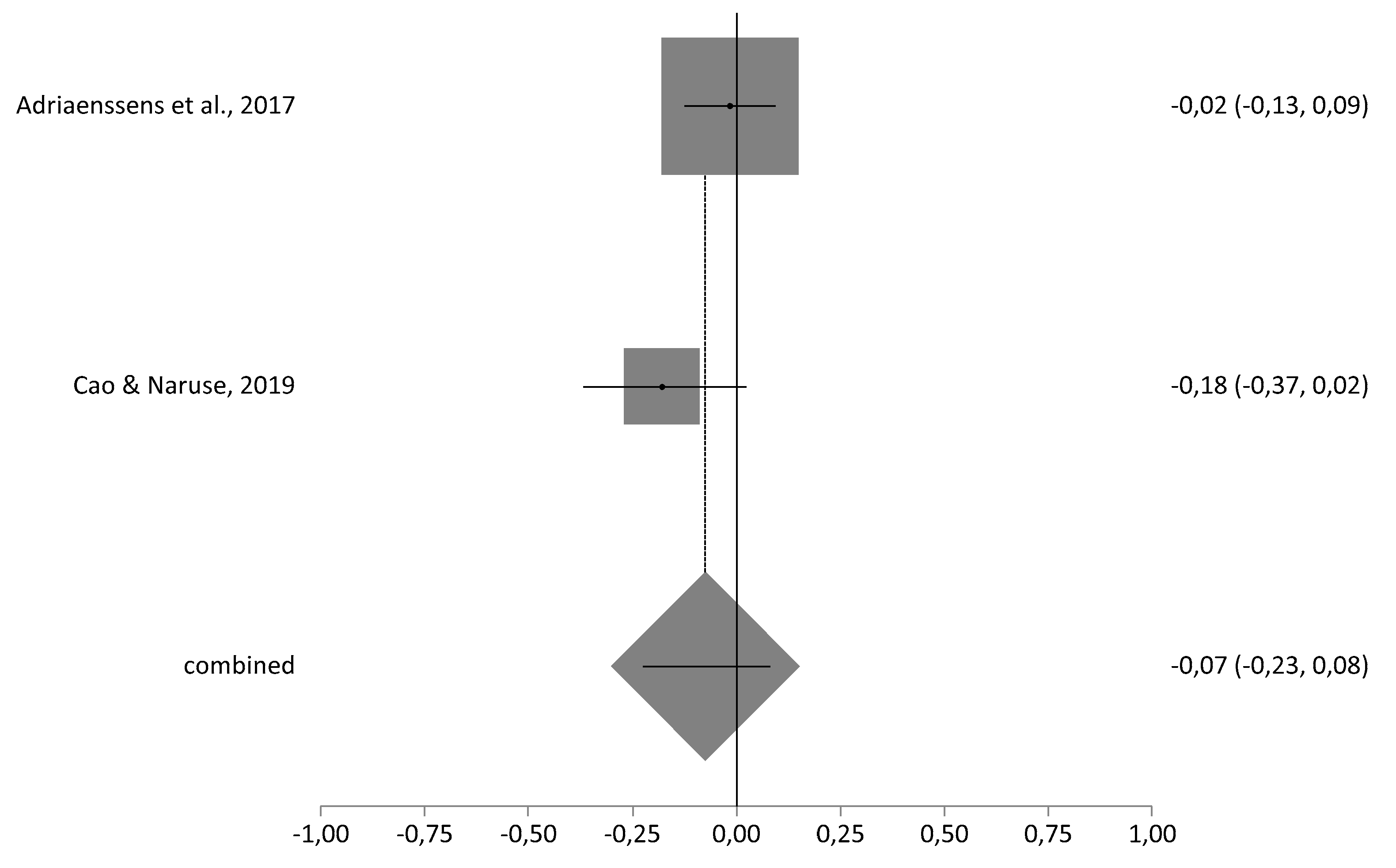
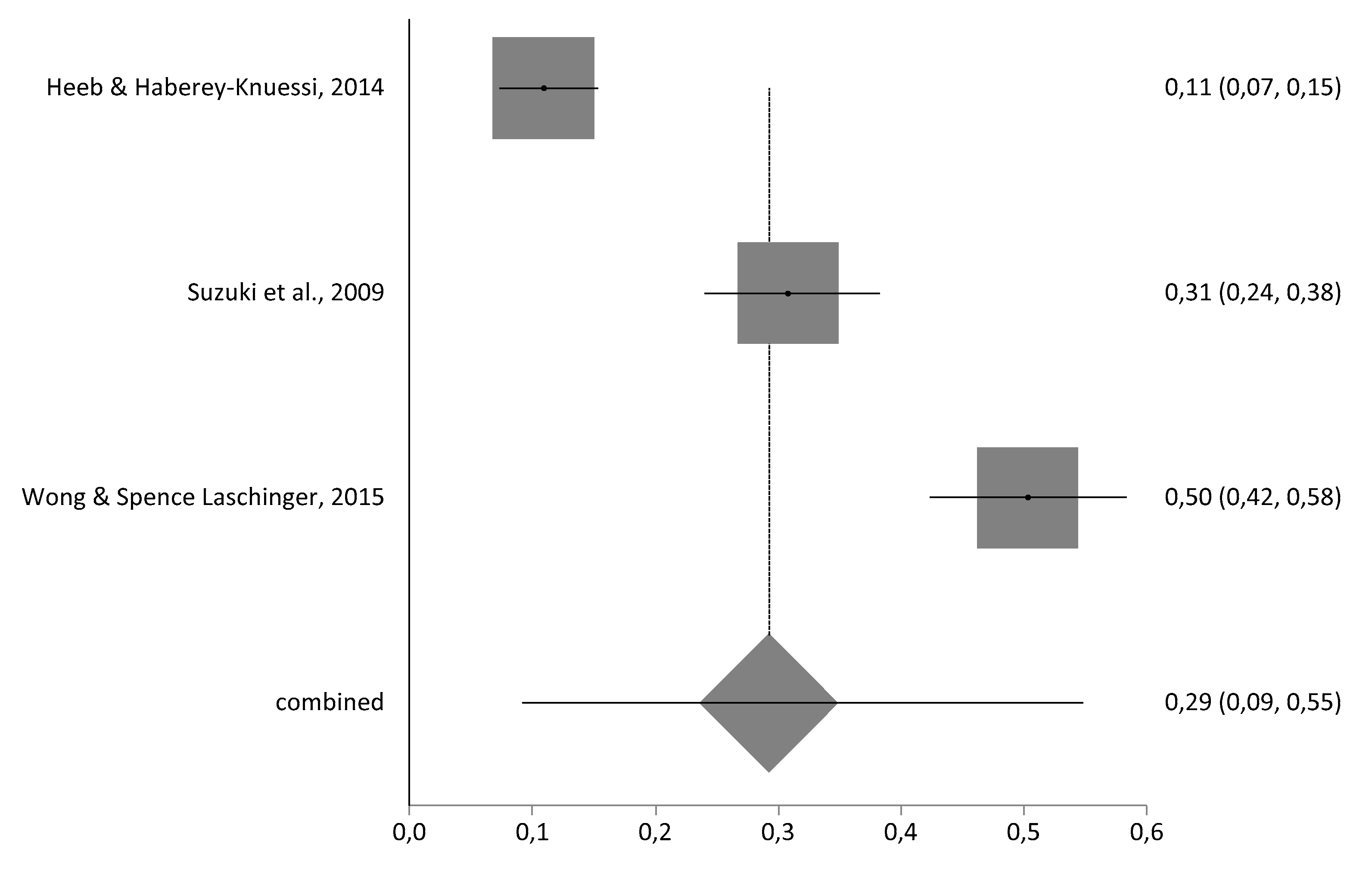
3.4. Meta-Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Issues
References
- Stamm, B.H. Measuring compassion satisfaction as well as fatigue: Developmental history of the Compassion Satisfaction and Fatigue Test. In Treating Compassion Fatigue; Figley, C.R., Ed.; Brunner-Routledge: New York, NY, USA, 2002. [Google Scholar]
- Schaufeli, W.B.; Leiter, M.; Maslach, C. Burnout: 35 years of research and practice. Career Dev. Int. 2019, 14, 204–220. [Google Scholar] [CrossRef] [Green Version]
- Freudenberger, H.J. Staff burn-out. J. Soc. Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Monsalve-Reyes, C.S.; San Luis-Costas, C.; Fernández- Castillo, R.; Aguayo-Estremera, R.; Cañadas-de la Fuente, G.A. Factores de riesgo y niveles de burnout en enfermeras de atención primaria: Una revisión sistemática. Atención Primaria 2017, 49, 77–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cañadas-De la Fuente, G.A.; Vargas, C.; San Luis, C.; García, I.; Cañadas, G.R.; De la Fuente, E.I. Risk factors and prevalence of burnout syndrome in the nursing profession. Int. J. Nurs. Stud. 2015, 52, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Molina-Praena, J.; Ramírez-Baena, L.; Gómez-Urquiza, J.; Cañadas, G.; De la Fuente, E.; Cañadas-De la Fuente, G. Levels of burnout and risk factors in medical area nurses: A meta-analytic study. Int. J. Environ. Res. Public Health 2018, 15, 2800. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Parada, M.E.; Moreno, B.R.; Mejías, M.Z.; Rivas, F.A.; Rivas, F.F.; Cerrada, S.J.; Rivas, P. Job satisfaction and burnout syndrome in the nursing staff of the Instituto Autónomo Hospital Universitario Los Andes, Mérida, Venezuela. Rev. Fac. Nac. Salud Pública 2005, 23, 33–45. [Google Scholar]
- Adriaenssens, J.; Hamelink, A.; Van Bogaert, P. Predictors of occupational stress and well-being in first-line nurse managers: A cross-sectional survey study. Int. J. Nurs. Stud. 2017, 73, 85–92. [Google Scholar] [CrossRef]
- Franco, G.P.; de Barros, A.L.B.L.; Nogueira-Martins, L.A.; Zeitoun, S.S. Burnout in nursing residents. Rev. Esc. Enferm USP 2011, 45, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Bjerregård-Madsen, J.; Kaila, A.; Vehviläinen-Julkunen, K.; Miettinen, M. Time allocation and temporal focus in nursing management: An integrative Review. J. Nurs. Manag. 2016, 24, 983–993. [Google Scholar] [CrossRef]
- Gallagher, R.M.; Gormley, D.K. Perceptions of stress, burnout, and support systems in pediatric bone marrow transplantation nursing. Clin. J. Oncol. Nurs. 2009, 13, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Qucik, T.L. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life. Natl. Product. Rev. 1990, 9, 475–479. [Google Scholar]
- Ciapponi, A. Critical appraisal guide of observational studies in epidemiology. Evid Actual Pract. Ambul. 2010, 13, 135–140. [Google Scholar]
- Cao, X.; Naruse, T. Effect of time pressure on the burnout of home-visiting nurses: The moderating role of relational coordination with nursing managers. Jpn. J. Nurs. Sci. 2018, 16, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.A.; Laschinger, H.K.S. The influence of frontline manager job strain on burnout, commitment and turnover intention: A cross-sectional study. Int. J. Nurs. Stud. 2015, 52, 1824–1833. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.; Saito, M.; Tagaya, A.; Mihara, R.; Maruyama, A.; Azuma, T.; Sato, C. Relationship between assertiveness and burnout among nurse managers. Jpn. J. Nurs. Sci. 2009, 6, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Heeb, J.-L.; Haberey-Knuessi, V. Health professionals facing burnout: What do we know about nursing managers? Nurs. Res. Pract. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Laschinger, H.K.S.; Finegan, J. Situational and dispositional predictors of nurse manager burnout: A time-lagged analysis. J. Nurs. Manag. 2008, 16, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Kanste, O. The association between leadership behaviour and burnout among nursing personnel in health care. Nord. J. Nurs. Res. 2015, 28, 4–8. [Google Scholar] [CrossRef]
- Lee, V.; Henderson, M.C. Occupational stress and organizational commitment in nurse administrators. JONA J. Nurs. Adm. 1996, 26, 21–28. [Google Scholar] [CrossRef]
- Hewko, S.J.; Brown, P.; Fraser, K.D.; Wong, C.A.; Cummings, G. Factors influencing nurse managers’ intent to stay or leave: A quantitative analysis. J. Nurs. Manag. 2015, 23, 1058–1066. [Google Scholar] [CrossRef]
- Karsavuran, S.; Kaya, S. The relationship between burnout and mobbing among hospital managers. Nurs. Ethics 2017, 24, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Ceravolo, D.; Raines, D.A. The impact of a mindfulness intervention for nurse managers. J. Holist. Nurs. 2019, 37, 47–55. [Google Scholar] [CrossRef] [PubMed]
- The Oxford 2011 Levels of Evidence. Available online: https://www.cebm.net/2011/06/explanation-2011-ocebm-levels-evidence/ (accessed on 3 June 2020).
- Ramírez-Baena, L.; Ortega-Campos, E.; Gómez-Urquiza, J.L.; Cañadas-De la Fuente, G.R.; De la Fuente-Solana, E.I.; Cañadas-De la Fuente, G.A. A multicentre study of burnout prevalence and related psychological variables in medical area hospital nurses. J. Clin. Med. 2019, 8, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grazziano, E.; Ferraz Bianchi, E.R. Impacto del estrés ocupacional y burnout en enfermeros. Enfermería Glob. 2010. [Google Scholar] [CrossRef] [Green Version]
- Tully, S.; Tao, H. CE: Original research: Work-related stress and positive thinking among acute care nurses: A cross-sectional survey. Am. J. Nurs. 2019, 119, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Alarcón, C.; Cervantes, M.E.; Dominguez, A.; Hernández, J.; Velázquez, M. Evaluación de la conducta asertiva y no asertiva en enfermeras jefe de planta. Rev. Enf. IMSS 2003, 11, 133–142. [Google Scholar]
- Guo, Y.; Luo, Y.; Lam, L.; Cross, W.; Plummer, V.; Zhang, J. Burnout and its association with resilience in nurses: A cross-sectional study. J. Clin. Nurs. 2018, 27, 441–449. [Google Scholar] [CrossRef]
- Khan, B.P.; Quinn-Griffin, M.T.; Fitzpatrick, J.J. Staff nurses’ perceptions of their nurse managers’ transformational leadership behaviours and their own structural empowerment. J. Nurs. Admin. 2018, 48, 609–614. [Google Scholar] [CrossRef]
- Boamah, S.A.; Read, E.A.; Spence-Laschinger, H.K. Factors influencing new graduate nurse burnout development, job satisfaction and patient care quality: A time-lagged study. J. Adv. Nurs. 2017, 73, 1182–1195. [Google Scholar] [CrossRef]
- Naruse, T.; Taguchi, A.; Kuwahara, Y.; Nagata, S.; Watai, I.; Murashima, S. Relationship between perceived time pressure during visits and burnout among home visiting nurses in Japan. Jpn. J. Nurs. Sci. 2012, 9, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Cañadas-De La Fuente, G.A.; Albendín-García, L.; De la Fuente, E.I.; San Luis, C.; Gómez-Urquiza, J.L.; Cañadas, G.R. Síndrome de burnout en profesionales de enfermería que realizan jornada física complementaria en servicios de cuidados críticos y urgencias. Rev. Esp. Salud Pública 2016, 90, 1–9. [Google Scholar]
- Portero de la Cruz, S.P.; Cebrerino-Cruz, J.C.; Herruzo-Cabrera, J.H.; Vaquero-Abellán, M.V. Fatores relacionados à probabilidade de sofrer problemas de saúde mental em profissionais de emergência. Rev. Lat. Am. Enferm. 2019, 27, 3144. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Davey, A.; Davey, S.; Shukla, A.; Shrivastava, K.; Bansal, R. Occupational stress among staff nurses: Controlling the risk to health. Indian J. Occup. Environ. Med. 2014, 18, 52–56. [Google Scholar]
- De Carvalho, D.P.; Rocha, L.P.; Barlem, E.L.D.; Barlem, E.L.D.; Cecagno, D.; Dalmolin, G.D.L. Productivity versus workloads in the nursing working environment. Rev. Esc. Enferm. USP 2018, 51, 51. [Google Scholar] [CrossRef]
- Wei, H.; Roberts, P.; Strickler, J.; Corbett, R.W. Nurse leaders’ strategies to foster nurse resilience. J. Nurs. Manag. 2019, 27, 681–687. [Google Scholar] [CrossRef]
- Huyghebaert, T.; Gillet, N.; Audusseau, O.; Fouquereau, E. Perceived career opportunities, commitment to the supervisor, social isolation: Their effects on nurses’ well-being and turnover. J. Nurs. Manag. 2019, 27, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Maza, Y.; Shechter, E.; Eizenberg, N.P.; Segev, E.G.; Flugelman, M.Y. Physician empowerment programme; a unique workshop for physician-managers of community clinics. BMC Med. Educ. 2016, 16, 269. [Google Scholar] [CrossRef] [Green Version]
- Gómez del Pulgar, E.; Meléndez-Moreno, A. Mindfulness, prevención y control del síndrome de desgaste profesional en la enfermería española. Rev. Enfermería Trabajo 2017, 3, 70–75. [Google Scholar]
- Knupp, A.M.; Patterson, E.S.; Ford, J.L.; Zurmehly, J.; Patrick, T. Associations among nurse fatigue, individual nurse factors, and aspects of the nursing practice environment. J. Nurs. Admin. 2018, 48, 642–648. [Google Scholar] [CrossRef]
- Lindholm, M. Working conditions, psychosocial resources and work stress in nurses and physicians in chief managers’ positions. J. Nurs. Manag. 2006, 14, 300–309. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors (Publication Year), Country. | Burnout Instrument | n | Characteristics | Mean Values (Standard Deviation) | Study Design/OCEBM* |
|---|---|---|---|---|---|
| Suzuki et al. (2009) [17], Japan. | MBIJ-RAS | 172 | Age: 43.8 ± 7.1 Married: 30.2% Children: 29.9% | Burnout total = 11.0 EE = 1.4 D = 3.6 | Cross-sectional/ LE: 2C GR: B |
| Wong et al. (2015) [16], Canada. | MBI | 159 | Age: 48.1 ± 7.0 Female: 143 (92.3%) Male: 12 (7.7%) | EE = 2.91 (1.44) D = 1.58 (1.44) | Cross-sectional/ LE: 2C GR: B |
| Heeb et al. (2014) [18], Switzerland. | MBI-HSS | 257 | Age: 46.7 Female: 58.0% Married: 58% Children: 56.4% | EE = 16.9 (7.1) D = 5.4 (4.2) PA = 35.6 (6.9) | Cross-sectional/ LE: 2C GR: B |
| Spence Laschinger et al. (2008) [19], Canada. | MBI | 134 | Age: 48.04 ± 10.21 Female: 129 (95.3%) Male: 5% (4.7) | EE = 3.14 (1.15) | Cross-sectional/ LE: 2C GR: B |
| Adriaenssens et al. (2017) [9], Belgium. | MBI-HSS | 319 | Age: 45.7 (24–63) Female: 59.1% Children: 86.2% Full time: 85.8% | EE = 1.42 (0.71) | Cross-sectional/ LE: 2C GR: B |
| Kanste (2008) [20], Finland. | MBI-HSS | 627 | Female: 94% Male: 6% Age: 43.7 ± 9.0 | EE = 2.95 D = 1.82 PA = 6.18 | Cross-sectional/ LE: 2C GR: B |
| Cao et al. (2018) [15], Japan. | J-BI | 93 | Female: 97.8% Male: 2.2% Age: 43.26 ± 7.98 Full time: 67.7% | EE = 2.46 (0.91) D = 1.70 (0.70) | Cross-sectional/ LE: 2C GR: B |
| Lee et al. (1996) [21], USA. | MBI | 78 | Female: 93% Married: 79% | ND | Cross-sectional/ LE: 2C GR: B |
| Hewko et al. (2015) [22], Canada. | MBI | 95 | Female: 87 (92%) Male: 8 (8%) Age: 75% (40–59) | EE = 3.57 (1.38) D = 3.58 (1.50) PA = 5.08 (1.09) | Cross-sectional/ LE: 2C GR: B |
| Karsavuran et al. (2017) [23], Turkey. | MBI | 244 | Female: 78 (32%) Male: 166 (68%) Married: 75.4% Age: 38% (50s) | High scores for EE and D and low scores for PA were associated with high levels of burnout. | Cross-sectional/ LE: 2C GR: B |
| Ceravolo et al. (2019) [24], USA. | ProQOL CBI | 12 | The mindfulness intervention had a positive impact on the Professional Quality of Life and Copenhagen Burnout Inventory scores. | Longitudinal Prospective/ LE:2C GR: B |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Membrive-Jiménez, M.J.; Pradas-Hernández, L.; Suleiman-Martos, N.; Vargas-Román, K.; Cañadas-De la Fuente, G.A.; Gomez-Urquiza, J.L.; De la Fuente-Solana, E.I. Burnout in Nursing Managers: A Systematic Review and Meta-Analysis of Related Factors, Levels and Prevalence. Int. J. Environ. Res. Public Health 2020, 17, 3983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113983
Membrive-Jiménez MJ, Pradas-Hernández L, Suleiman-Martos N, Vargas-Román K, Cañadas-De la Fuente GA, Gomez-Urquiza JL, De la Fuente-Solana EI. Burnout in Nursing Managers: A Systematic Review and Meta-Analysis of Related Factors, Levels and Prevalence. International Journal of Environmental Research and Public Health. 2020; 17(11):3983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113983
Chicago/Turabian StyleMembrive-Jiménez, María José, Laura Pradas-Hernández, Nora Suleiman-Martos, Keyla Vargas-Román, Guillermo A. Cañadas-De la Fuente, José Luis Gomez-Urquiza, and Emilia I. De la Fuente-Solana. 2020. "Burnout in Nursing Managers: A Systematic Review and Meta-Analysis of Related Factors, Levels and Prevalence" International Journal of Environmental Research and Public Health 17, no. 11: 3983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113983