Red and Processed Meat Consumption and Risk of Depression: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Background
1.2. Aim of the Study
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Evaluation
2.5. Meta-Analysis
2.6. Subgroup and Sensitivity Analysis
3. Results
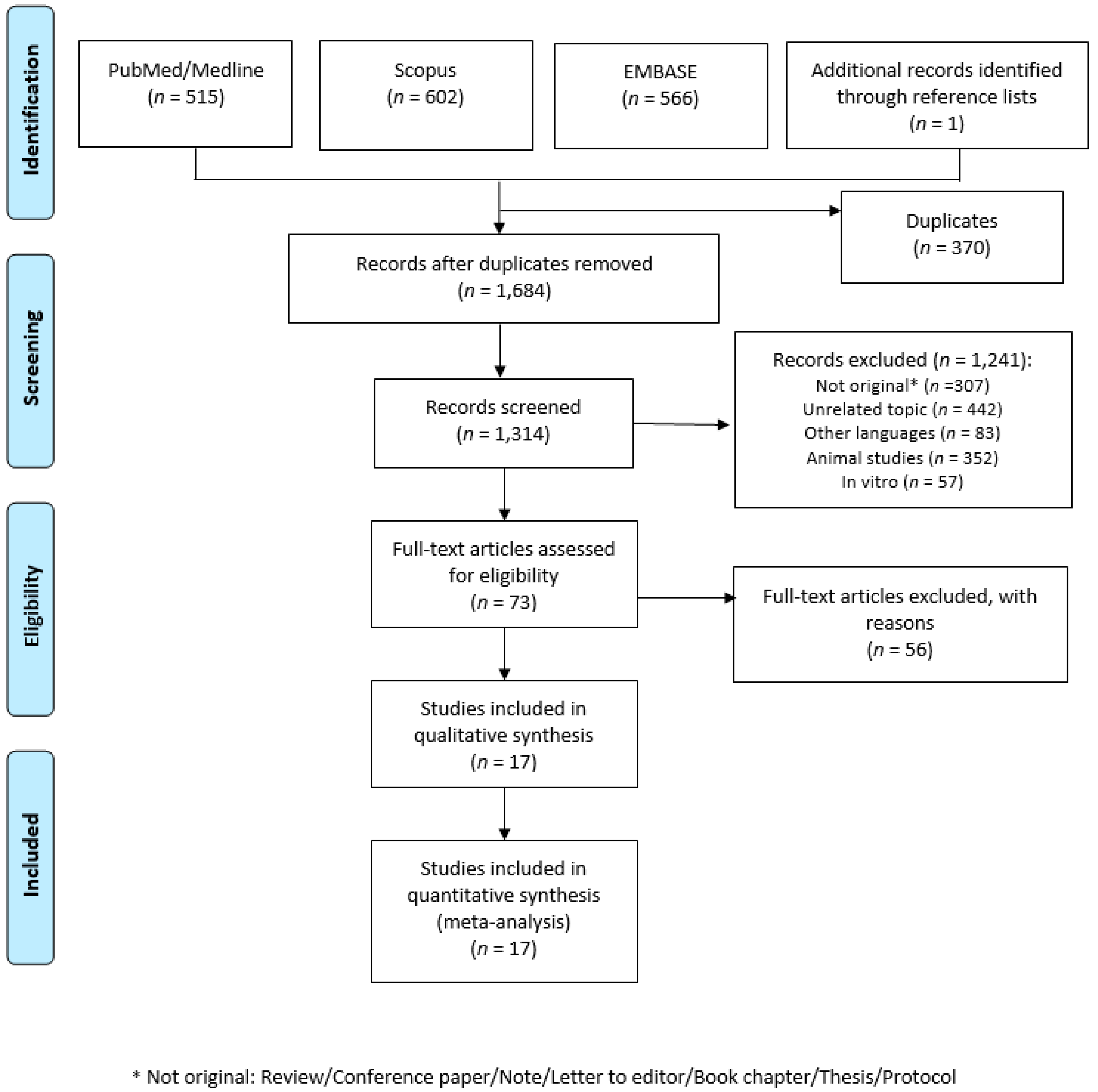
3.1. Literature Search
3.2. Characteristics of the Included Studies
3.3. Characteristics of the Studied Populations
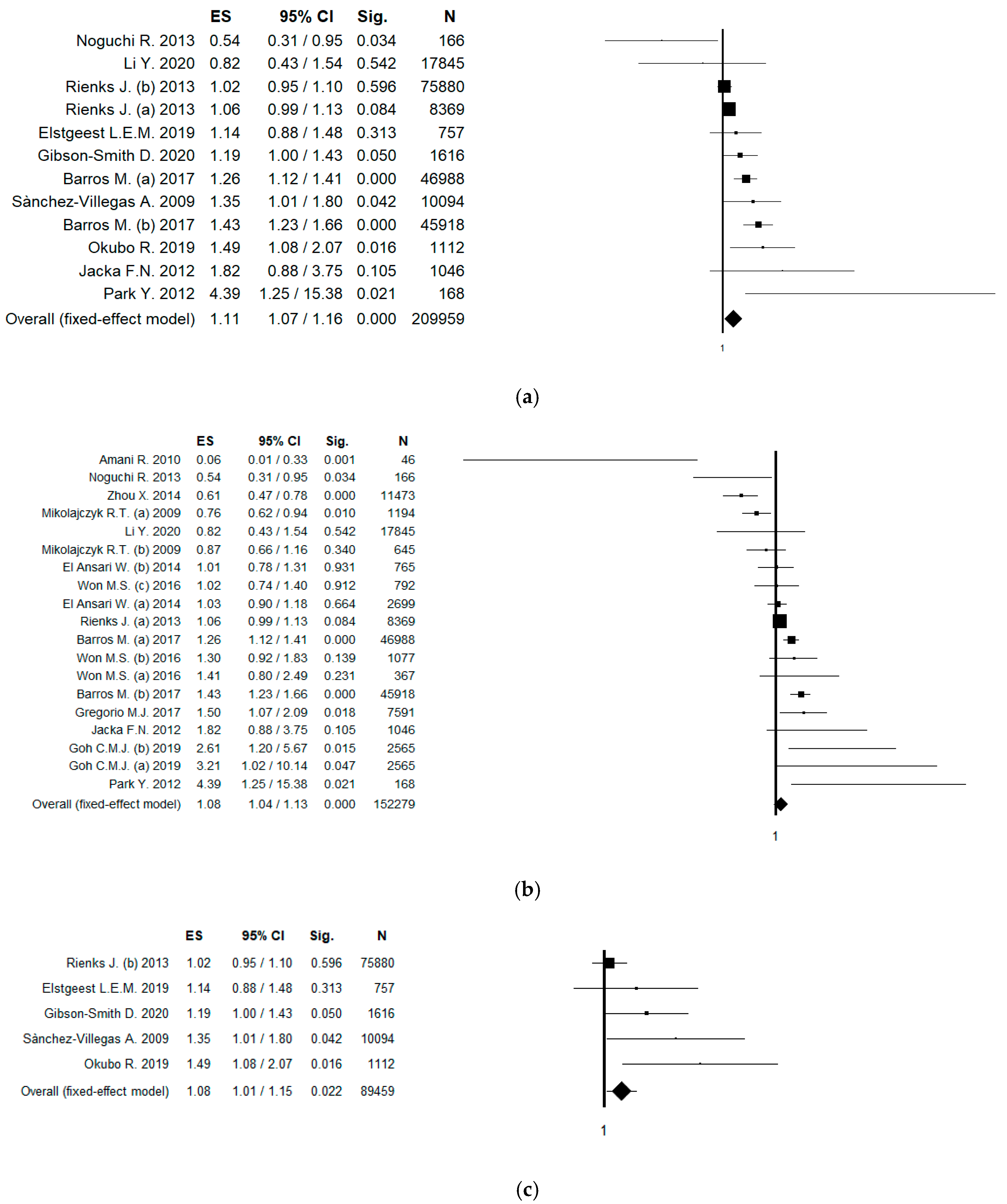
3.4. Results of Meta-Analysis
3.5. Sensitivity Analysis
3.6. Subgroup Analysis by Gender
4. Discussion
Limitantions and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Depression. Available online: https://www.who.int/news-room/fact-sheets/detail/depression#:~:text=Depression%20is%20a%20leading%20cause%20of%20disability%20worldwide,and%20pharmacological%20treatments%20for%20moderate%20and%20severe%20depression (accessed on 7 August 2020).
- Fornaro, M.; Solmi, M.; Stubbs, B.; Veronese, N.; Monaco, F.; Novello, S.; Fusco, A.; Anastasia, A.; De Berardis, D.; Carvalho, A.F.; et al. Prevalence and correlates of major depressive disorder, bipolar disorder and schizophrenia among nursing home residents without dementia: Systematic review and meta-analysis. Br. J. Psychiatry 2020, 216, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amerio, A.; Odone, A.; Marchesi, C.; Ghaemi, S.N. Is depression one thing or many? Br. J. Psychiatry 2014, 204, 488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.S.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Borges, G.; Bromet, E.J.; Bruffaerts, R.; de Girolamo, G.; de Graaf, R.; Gureje, O.; et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet 2007, 370, 841–850. [Google Scholar] [CrossRef] [Green Version]
- Orsolini, L.; Latini, R.; Pompili, M.; Serafini, G.; Volpe, U.; Vellante, F.; Fornaro, M.; Valchera, A.; Tomasetti, C.; Fraticelli, S.; et al. Understanding the Complex of Suicide in Depression: From Research to Clinics. Psychiatry Investig. 2020, 17, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacka, F.N. Nutritional Psychiatry: Where to Next? EBioMedicine 2017, 17, 24–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandhu, K.V.; Sherwin, E.; Schellekens, H.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Feeding the microbiota-gut-brain axis: Diet, microbiome, and neuropsychiatry. Transl. Res. 2017, 179, 223–244. [Google Scholar] [CrossRef]
- Saghafian, F.; Malmir, H.; Saneei, P.; Milajerdi, A.; Larijani, B.; Esmaillzadeh, A. Fruit and vegetable consumption and risk of depression: Accumulative evidence from an updated systematic review and meta-analysis of epidemiological studies. Br. J. Nutr. 2018, 119, 1087–1101. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Liu, X.; Zhang, D. Fish consumption and risk of depression: A meta-analysis. J. Epidemiol. Community Health 2016, 70, 299–304. [Google Scholar] [CrossRef]
- Li, Y.; Lv, M.R.; Wei, Y.J.; Sun, L.; Zhang, J.X.; Zhang, H.G.; Li, B. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef]
- Norde, M.M.; Collese, T.S.; Giovannucci, E.; Rogero, M.M. A posteriori dietary patterns and their association with systemic low-grade inflammation in adults: A systematic review and meta-analysis. Nutr. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.S.; Lau, R.; Aune, D.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Red and processed meat and colorectal cancer incidence: Meta-analysis of prospective studies. PLoS ONE 2011, 6, e20456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasso, A.; Latella, G. Role of Heme Iron in the Association between Red Meat Consumption and Colorectal Cancer. Nutr. Cancer 2018, 70, 1173–1183. [Google Scholar] [CrossRef]
- Seiwert, N.; Heylmann, D.; Hasselwander, S.; Fahrer, J. Mechanism of colorectal carcinogenesis triggered by heme iron from red meat. Biochim. Biophys. Acta Rev. Cancer 2020, 1873, 188334. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer Working Group on the Evaluation of Carcinogenic Risks to Humans. In Monographs on the Evaluation of Carcinogenic Risks to Humans; Red Meat and Processed Meat; IARC: Lyon, France, 2018; pp. 107–422.
- Santarelli, R.L.; Pierre, F.; Corpet, D.E. Processed meat and colorectal cancer: A review of epidemiologic and experimental evidence. Nutr. Cancer 2008, 60, 131–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiavarini, M.; Bertarelli, G.; Minelli, L.; Fabiani, R. Dietary Intake of Meat Cooking-Related Mutagens (HCAs) and Risk of Colorectal Adenoma and Cancer: A Systematic Review and Meta-Analysis. Nutrients 2017, 9, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective; Third Expert Report, Continuous Update Project Expert Report; World Cancer Research Fund/American Institute for Cancer Research: Washington, DC, USA, 2018. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Ng, C.G.; Boks, M.P.; Zainal, N.Z.; de Wit, N.J. The prevalence and pharmacotherapy of depression in cancer patients. J. Affect. Disord. 2011, 131, 1–7. [Google Scholar] [CrossRef]
- Okamura, M.; Yamawaki, S.; Akechi, T.; Taniguchi, K.; Uchitomi, Y. Psychiatric disorders following first breast cancer recurrence: Prevalence, associated factors and relationship to quality of life. Jpn. J. Clin. Oncol. 2005, 35, 302–309. [Google Scholar] [CrossRef]
- Firth, J.; Veronese, N.; Cotter, J.; Shivappa, N.; Hebert, J.R.; Ee, C.; Smith, L.; Stubbs, B.; Jackson, S.E.; Sarris, J. What Is the Role of Dietary Inflammation in Severe Mental Illness? A Review of Observational and Experimental Findings. Front. Psychiatry 2019, 10, 350. [Google Scholar] [CrossRef] [PubMed]
- Polokowski, A.R.; Shakil, H.; Carmichael, C.L.; Reigada, L.C. Omega-3 fatty acids and anxiety: A systematic review of the possible mechanisms at play. Nutr. Neurosci. 2020, 23, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk, R.T.; El Ansari, W.; Maxwell, A.E. Food consumption frequency and perceived stress and depressive symptoms among students in three European countries. Nutr. J. 2009, 8, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, X.; Bi, B.; Zheng, L.; Li, Z.; Yang, H.; Song, H.; Sun, Y. The prevalence and risk factors for depression symptoms in a rural Chinese sample population. PLoS ONE 2014, 9, e99692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, D.; Lisy, K.; Lockwood, C.; Colbeck, M. The impact of essential fatty acid, B vitamins, vitamin C, magnesium and zinc supplementation on stress levels in women: A systematic review. JBI Database Syst. Rev. Implement Rep. 2017, 15, 402–453. [Google Scholar] [CrossRef]
- Petridou, E.T.; Kousoulis, A.A.; Michelakos, T.; Papathoma, P.; Dessypris, N.; Papadopoulos, F.C.; Stefanadis, C. Folate and B12 serum levels in association with depression in the aged: A systematic review and meta-analysis. Aging Ment. Health 2016, 20, 965–973. [Google Scholar] [CrossRef]
- Petrilli, M.A.; Kranz, T.M.; Kleinhaus, K.; Joe, P.; Getz, M.; Johnson, P.; Chao, M.V.; Malaspina, D. The Emerging Role for Zinc in Depression and Psychosis. Front. Pharmacol. 2017, 8, 414. [Google Scholar] [CrossRef] [Green Version]
- Selhub, J. Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J. Nutr. Health Aging 2002, 6, 39–42. [Google Scholar]
- Esnafoglu, E.; Ozturan, D.D. The relationship of severity of depression with homocysteine, folate, vitamin B12, and vitamin D levels in children and adolescents. Child Adolesc. Ment. Health 2020. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.; Brunnhuber, K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M.; Forbes, C.; Glanville, J.; Hicks, N.J.; Moody, J.; et al. How to formulate research recommendations. BMJ 2006, 333, 804–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0.; The Cochrane Collaboration: London, UK, 2013. [Google Scholar]
- Gianfredi, V.; Bragazzi, N.L.; Nucci, D.; Villarini, M.; Moretti, M. Cardiovascular diseases and hard drinking waters: Implications from a systematic review with meta-analysis of case-control studies. J. Water Health 2017, 15, 31–40. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Abalsamo, A.; Acito, M.; Villarini, M.; Moretti, M.; Realdon, S. Green Tea Consumption and Risk of Breast Cancer and Recurrence-A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2018, 10, 1886. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Salvatori, T.; Nucci, D.; Villarini, M.; Moretti, M. Genotoxic risk in nurses handling antiblastic drugs: Systematic review of literature and meta-analysis. Recenti Prog. Med. 2017, 108, 511–520. [Google Scholar] [CrossRef]
- Amerio, A.; Stubbs, B.; Odone, A.; Tonna, M.; Marchesi, C.; Nassir Ghaemi, S. Bipolar I and II Disorders; A Systematic Review and Meta-Analysis on Differences in Comorbid Obsessive-Compulsive Disorder. Iran. J. Psychiatry Behav. Sci. 2016, 10, e3604. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Paterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 14 November 2018).
- Hedges, L.V.; Veve, J.L. Fixed- and Random-effects models in meta-analysis. Psychol. Methods 1998, 3, 486–504. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianfredi, V.; Nucci, D.; Fatigoni, C.; Salvatori, T.; Villarini, M.; Moretti, M. Extent of Primary DNA Damage Measured by the Comet Assay in Health Professionals Exposed to Antineoplastic Drugs: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 523. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Lin, L. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Salvatori, T.; Dallagiacoma, G.; Fatigoni, C.; Moretti, M.; Realdon, S. Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1579. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Salvatori, T.; Villarini, M.; Moretti, M.; Nucci, D.; Realdon, S. Is dietary fibre truly protective against colon cancer? A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2018, 69, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Amani, R.; Saeidi, S.; Nazari, Z.; Nematpour, S. Correlation between dietary zinc intakes and its serum levels with depression scales in young female students. Biol. Trace Elem. Res. 2010, 137, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Barros, M.B.A.; Lima, M.G.; Azevedo, R.C.S.; Medina, L.B.P.; Lopes, C.S.; Menezes, P.R.; Malta, D.C. Depression and health behaviors in Brazilian adults—PNS 2013. Rev. Saud. Publica 2017, 51, 8s. [Google Scholar] [CrossRef] [Green Version]
- El Ansari, W.; Adetunji, H.; Oskrochi, R. Food and mental health: Relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent. Eur. J. Public Health 2014, 22, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Elstgeest, L.E.M.; Visser, M.; Penninx, B.; Colpo, M.; Bandinelli, S.; Brouwer, I.A. Bidirectional associations between food groups and depressive symptoms: Longitudinal findings from the Invecchiare in Chianti (InCHIANTI) study. Br. J. Nutr. 2019, 121, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Gibson-Smith, D.; Bot, M.; Brouwer, I.A.; Visser, M.; Giltay, E.J.; Penninx, B. Association of food groups with depression and anxiety disorders. Eur. J. Nutr. 2020, 59, 767–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, C.M.J.; Abdin, E.; Jeyagurunathan, A.; Shafie, S.; Sambasivam, R.; Zhang, Y.J.; Vaingankar, J.A.; Chong, S.A.; Subramaniam, M. Exploring Singapore’s consumption of local fish, vegetables and fruits, meat and problematic alcohol use as risk factors of depression and subsyndromal depression in older adults. BMC Geriatr. 2019, 19, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregorio, M.J.; Rodrigues, A.M.; Eusebio, M.; Sousa, R.D.; Dias, S.; Andre, B.; Gronning, K.; Coelho, P.S.; Mendes, J.M.; Graca, P.; et al. Dietary Patterns Characterized by High Meat Consumption Are Associated with Other Unhealthy Life Styles and Depression Symptoms. Front. Nutr. 2017, 4, 25. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Pasco, J.A.; Williams, L.J.; Mann, N.; Hodge, A.; Brazionis, L.; Berk, M. Red meat consumption and mood and anxiety disorders. Psychother. Psychosom. 2012, 81, 196–198. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, C.; Li, S.; Zhang, D. Association between dietary protein intake and the risk of depressive symptoms in adults. Br. J. Nutr. 2020, 1–12. [Google Scholar] [CrossRef]
- Noguchi, R.; Hiraoka, M.; Watanabe, Y.; Kagaw, Y. Relationship between dietary patterns and depressive symptoms: Difference by gender, and unipolar and bipolar depression. J. Nutr. Sci. Vitaminol. 2013, 59, 115–122. [Google Scholar] [CrossRef] [Green Version]
- Okubo, R.; Matsuoka, Y.J.; Sawada, N.; Mimura, M.; Kurotani, K.; Nozaki, S.; Shikimoto, R.; Tsugane, S. Diet quality and depression risk in a Japanese population: The Japan Public Health Center (JPHC)-based Prospective Study. Sci. Rep. 2019, 9, 7150. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Kim, M.; Baek, D.; Kim, S.H. Erythrocyte n-3 polyunsaturated fatty acid and seafood intake decrease the risk of depression: Case-control study in Korea. Ann. Nutr. Metab. 2012, 61, 25–31. [Google Scholar] [CrossRef]
- Rienks, J.; Dobson, A.J.; Mishra, G.D. Mediterranean dietary pattern and prevalence and incidence of depressive symptoms in mid-aged women: Results from a large community-based prospective study. Eur. J. Clin. Nutr. 2013, 67, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Villegas, A.; Delgado-Rodriguez, M.; Alonso, A.; Schlatter, J.; Lahortiga, F.; Serra Majem, L.; Martinez-Gonzalez, M.A. Association of the Mediterranean dietary pattern with the incidence of depression: The Seguimiento Universidad de Navarra/University of Navarra follow-up (SUN) cohort. Arch. Gen. Psychiatry 2009, 66, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Won, M.S.; Kim, S.; Yang, Y.J. Comparison of Health Status and Nutrient Intake between Depressed Women and Non-depressed Women: Based on the 2013 Korea National Health and Nutrition Examination Survey. Clin. Nutr. Res. 2016, 5, 112–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Yang, Y.; Xie, M.S.; Ding, X.; Li, H.; Liu, Z.C.; Peng, S.F. Is meat consumption associated with depression? A meta-analysis of observational studies. BMC Psychiatry 2017, 17, 409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larrieu, T.; Laye, S. Food for Mood: Relevance of Nutritional Omega-3 Fatty Acids for Depression and Anxiety. Front. Physiol. 2018, 9, 1047. [Google Scholar] [CrossRef] [PubMed]
- Cannon, A.R.; Hammer, A.M.; Choudhry, M.A. Chapter 29—Alcohol, Inflammation, and Depression: The Gut-Brain Axis. In Inflammation and Immunity in Depression; Baune, B.T., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 509–524. [Google Scholar] [CrossRef]
- Tavares, A.I. Physical activity and healthy diet: Determinants and implicit relationship. Public Health 2014, 128, 568–575. [Google Scholar] [CrossRef]
- Ferravante, C.; Gianfredi, V.; Bietta, C. Nutrition in Umbria: Adherence to five-a-day. Recenti Prog. Med. 2020, 111, 539–545. [Google Scholar] [CrossRef]
- Dobal, M.T.; Wesley, Y.; Wilson, F.L. Decision-making process about food choices and physical activity among black women living in New York City: A qualitative study. Divers. Equal. Health Care 2017, 14, 302–312. [Google Scholar]
- Dreimuller, N.; Lieb, K.; Tadic, A.; Engelmann, J.; Wollschlager, D.; Wagner, S. Body mass index (BMI) in major depressive disorder and its effects on depressive symptomatology and antidepressant response. J. Affect. Disord. 2019, 256, 524–531. [Google Scholar] [CrossRef]
- Gianfredi, V.; Blandi, L.; Cacitti, S.; Minelli, M.; Signorelli, C.; Amerio, A.; Odone, A. Depression and Objectively Measured Physical Activity: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3738. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sanchez-Meca, J.; Marin-Martinez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [Green Version]
- Gianfredi, V.; Grisci, C.; Nucci, D.; Parisi, V.; Moretti, M. Communication in health. Recenti Prog. Med. 2018, 109, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Monarca, S.; Moretti, M.; Villarini, M. Health education, what is the role for pharmacist? Results from a cross sectional study in Umbria, Italy. Recenti Prog. Med. 2017, 108, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Balzarini, F.; Gola, M.; Mangano, S.; Carpagnano, L.F.; Colucci, M.E.; Gentile, L.; Piscitelli, A.; Quattrone, F.; Scuri, S.; et al. Leadership in Public Health: Opportunities for Young Generations Within Scientific Associations and the Experience of the “Academy of Young Leaders”. Front. Public Health 2019, 7, 378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankovic, N.; Geelen, A.; Streppel, M.T.; de Groot, L.C.; Orfanos, P.; van den Hooven, E.H.; Pikhart, H.; Boffetta, P.; Trichopoulou, A.; Bobak, M.; et al. Adherence to a healthy diet according to the World Health Organization guidelines and all-cause mortality in elderly adults from Europe and the United States. Am. J. Epidemiol. 2014, 180, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Nucci, D.; Minelli, L.; Gianfredi, V. MI NUTRO (MIgrants NUTRition knOwledge for integration): A nutrition education intervention among immigrants, Perugia (Italy)-pilot study. Recenti Prog. Med. 2020, 111, 546–552. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Search Strategy | Details |
|---|---|
| Inclusion criteria | P: adults (men and women) |
| E: high intake of red and processed meat | |
| O: Depressive disorder | |
| S: cohort studies, case-control, cross-sectional | |
| Exclusion criteria | P: people < 18 years old, pregnant women, patients with chronic diseases |
| E: combined consumption of multiple food components (e.g., dietary pattern) | |
| O: other psychological disorders | |
| S: not original papers (opinion paper, review article, commentary, letter, protocols, article without quantitative data, thesis, conference papers, note, book chapter), trials | |
| Language filter | English |
| Time filter | No filter (from inception) |
| Database | PubMed/Medline; EMBASE, Scopus |
| Author, Year [Reference] | Country | Study Design | Study Period | Sample Size, Gender, Age | N. Depressed Subjects, Gender, Age | Attrition+ | Diagnosis of Depression | Validated Tool, for Depression | Tool used to Assess Meat Intake | Validated Tool, for Meat Intake | Portion of Meat | OR, HR, β, r (CI95%) | Adjustment | QS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amani R., 2010 [53] | Iran | case-control | 2006 | 46 F, range 20–25 y | 23 mean age: 20.7 ± 1.6 y | 262 | 21-BDI | yes | 12-item semiquantitative FFQ | n.a. | 3–4 times/week | 2 cases/14 controls p < 0.001 | crude model | 7 |
| Barros M., 2017 [54] | Brazil | cross-sectional | 2013–2014 | 49,025 (25,542 F; 23,483 M) mean: 37 y | 3107 minor depression; 2037 major depression | 11,177 (M; F) | PHQ-9 | yes | 12-item FFQ | yes | weekly consumption | Minor depression: OR 1.26 (1.12–1.41) | age, sex, and education | 9 |
| Major depression: OR 1.43 (1.23–1.66) | ||||||||||||||
| El Ansari W., 2014 [55] | England, Walls, Ireland | cross-sectional | 2007–2008 | 3464 (2699 F; 765 M) mean: 24.9 ±8.6 | n.a. | 242 (M; F) | 20-items Modification of BDI | yes | 12-item questionnaire | no | several times a day | F: r = 0.008 p = 0.680 | crude model | 7 |
| M: r = −0.003 p = 0.942 | ||||||||||||||
| Elstgeest L.E.M., 2019 [56] | Italy | longitudinal study 3-y FU | 1998–2009 | baseline 1058 (579 F; 479 M) mean: 65.8 ±15.2 FU1: 960, FU2: 853, FU3: 757 | baseline: 187; FU1: 231; FU2: 145; FU3: 150 | 148 (M; F) | CES-D | yes | 240-FFQ | yes | Quartiles of standardized intake | β = −0.39 (−1.13, 0.36) p = 0.313 | baseline CES-D score, age, sex, marital status, education, PA, smoking, living disabilities, alcohol intake and energy intake. | 10 |
| Gibson-Smith D., 2020 [57] | the Netherlands | longitudinal 9-y FU | 2004 | 1634 (1108 F; 526 M = mean: 52.0 ± 13.2 | 414 depressed and 886 remission | 435 (M; F) | IDS-SR | yes | 258-FFQ | yes | n.a. | β = −0.05 (−0.11, −0.00) p = 0.05 | age, sex, education, marital status, PA, smoking status | 9 |
| Goh C.M.J., 2019 [58] | Singapore | cross-sectional | 2013 | 2565 (1448 F; 1117 M) range: 60–85 y | 425 subsyndromal; 177 depression | 0 | GMS-AGECAT | yes | National survey | no | n.a. | Depression: OR = 3.21 (1.02 10.14) p = 0.05 | crude model | 7 |
| Subsyndromal OR = 2.61 (1.20 5.67) p = 0.02 | ||||||||||||||
| Gregorio M.J., 2017 [59] | Portugal | cross-sectional | 2013–2015 | 7591 (4784 F; 2807 M) mean: 48.02 ± 18.02 | n.a. | 2562 (M; F) | HADS | yes | food questionnaire not further specified | n.a. | n.a. | OR = 1.50 (1.07 2.09) p = 0.018 | age, sex, education, employment, territorial units, smoking, PA and alcohol habits. | 9 |
| Jacka F.N., 2012 [60] | Australia | cross-sectional | 2009 | 1046 F range: 20–93 y | 60 | 81 | SCID-I/NP | yes | Cancer Council dietary questionnaire | yes | >57 g/day | OR = 1.82 (0.88 3.75) | age and dietary pattern score | 9 |
| Li Y., 2020 [61] | USA | cross-sectional | 2007–2014 | 17,845 (9102 F; 8743 M) range: 18–65 y | 1647; (1070 F; 577 M) | 0 | PHQ-9 | yes | 24-h dietary recall interviews by trained interviewers | yes | 0.20 g/kg per day | OR = 0.82 (0.43–1.54) | age, sex, race, marital status, education, income, BMI, diabetes, hypertension, smoking, alcohol, energy intake, fruit intake, vegetable intake, Mg intake, Zn intake, SFA intake, MUFA intake, PUFA intake and PA | 10 |
| Mikolajczyk R.T., 2009 [26] | Germany, Poland-Bulgaria | cross-sectional | 2005 | 1839 (1194 F; 645 M), mean: 20.6 ± 2.3 | n.a. | 264 (M; F) | M-BDI | yes | 12-item FFQ | no | n.a. | F: r = −1.38 p = 0.01 | country and all the other food components | 8 |
| M: r = −0.66 p = 0.34 | ||||||||||||||
| Noguchi R., 2013 [62] | Japan | cross-sectional | n.a. | 166 (62 F; 104 M) mean: 38.7 ± 10.2 | 75 (25 F; 50 M) | 0 | H-SDS | yes | BDHQ-56 foods | yes | n.a. | r = −0.159 | age, BMI and sex | 8 |
| Okubo R., 2019 [63] | Japan | longitudinal 5 y FU | 1990–2014 | 1112 (652 F; 460 M) mean: 73 y | 85 | 11,107 | PHQ-9 | yes | 147-FFQ | yes | 4 times/week | 27 cases/244 controls | crude model | 8 |
| Park Y., 2012 [64] | Korea | case-control | 2008–2010 | 168 (112 F; 56 M) mean: 44.85 ± 1.77 y | 80 (59 F; 21 M) | 0 | CES | yes | 91-FFQ | yes | >3.61 serving/week | OR = 4.39 (1.25–15.38) | Drinking, marital status, sleeping hours, education, job and energy except for energy intake | 8 |
| Rienks J., 2013 [65] | Australia | cross-sectional and longitudinal analysis 3-years FU | 2001–2004 | 8369 F in cross-sectional; mean: 52.5 ± 1.5 | 721 in cross-section; 660 in longitudinal | 2857 | CES | yes | 101-FFQ | yes | n.a. | OR = 1.06 (0.99–1.13) p = 0.11; | energy, smoking, PA, ability to manage on available income, occupation status, education, marital status, mean stress score and BMI | 10 |
| 7588 in longitudinal mean: 52.5 ± 1.5 | HR = 1.02 (0.95–1.10) p = 0.54 | |||||||||||||
| Sànchez-Villegas A., 2009 [66] | Spain | longitudinal 4.4 y FU | 1999–2005 | 10,094 (F and M) age n.a. | 480 (156 M, 324 F) | 5347 | self-reported | no | 136-FFQ | yes | 177 g/d M; 167 g/d F | HR= 1.35 (1.01–1.80) | sex, age, smoking, BMI, PA, energy intake, and employment | 8 |
| Won M.S., 2016 [67] | Korea | case-control | 2013 | 2236 F range: 19–64 y | 315 | 430 | self-reported | no | 112-FFQ | n.a. | 0.20 ± 0.02 servings/day | 19–29 y: 45 cases/322 controls; 30–49 y: 119 cases/958 controls; 50–64 y: 151 cases/641 controls | crude model | 5 |
| Zhou X., 2014 [27] | China | cross-sectional | 2012–2013 | 11,473 (6155 F; 5318 M) mean: 53.72 | n.a. | 0 | PHQ-9 | yes | food questionnaire not further specified | n.a. | ≥500 g/week | OR 0.61 (0.47–0.78) | crude model | 7 |
| Analysis | N. of Participants | ES (95% CI) |
|---|---|---|
| without potential overlapping effect | 192,185 | Fixed effect: 1.06 (1.02; 1.10) |
| Random effect: 1.08 (0.97; 1.29) | ||
| validated tool to assess meat intake | 209,959 | Fixed effect: 1.11 (1.07; 1.16) |
| Random effect: 1.18 (1.06; 1.32) | ||
| validated tool to diagnosis depression | 228,250 | Fixed effect: 1.07 (1.04; 1.12) |
| Random effect: 1.08 (0.97; 1.20) | ||
| prevalent depression | 152,279 | Fixed effect: 1.08 (1.04; 1.13) |
| Random effect: 1.07 (0.94; 1.23) | ||
| incident depression | 89,459 | Fixed effect: 1.08 (1.01; 1.15) |
| Random effect: 1.18 (1.02; 1.35) | ||
| quality score ≥ 8 | 219,389 | Fixed effect: 1.10 (1.05; 1.14) |
| Random effect: 1.14 (1.02; 1.26) | ||
| only women | 91,470 | Fixed effect: 1.03 (0.99; 1.08) |
| Random effect: 1.02 (0.91; 1.14) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nucci, D.; Fatigoni, C.; Amerio, A.; Odone, A.; Gianfredi, V. Red and Processed Meat Consumption and Risk of Depression: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6686. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186686
Nucci D, Fatigoni C, Amerio A, Odone A, Gianfredi V. Red and Processed Meat Consumption and Risk of Depression: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(18):6686. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186686
Chicago/Turabian StyleNucci, Daniele, Cristina Fatigoni, Andrea Amerio, Anna Odone, and Vincenza Gianfredi. 2020. "Red and Processed Meat Consumption and Risk of Depression: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 18: 6686. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17186686