Selecting Indicators to Monitor and Assess Environmental Health in a Portuguese Urban Setting: A Participatory Approach


Abstract
:1. Introduction
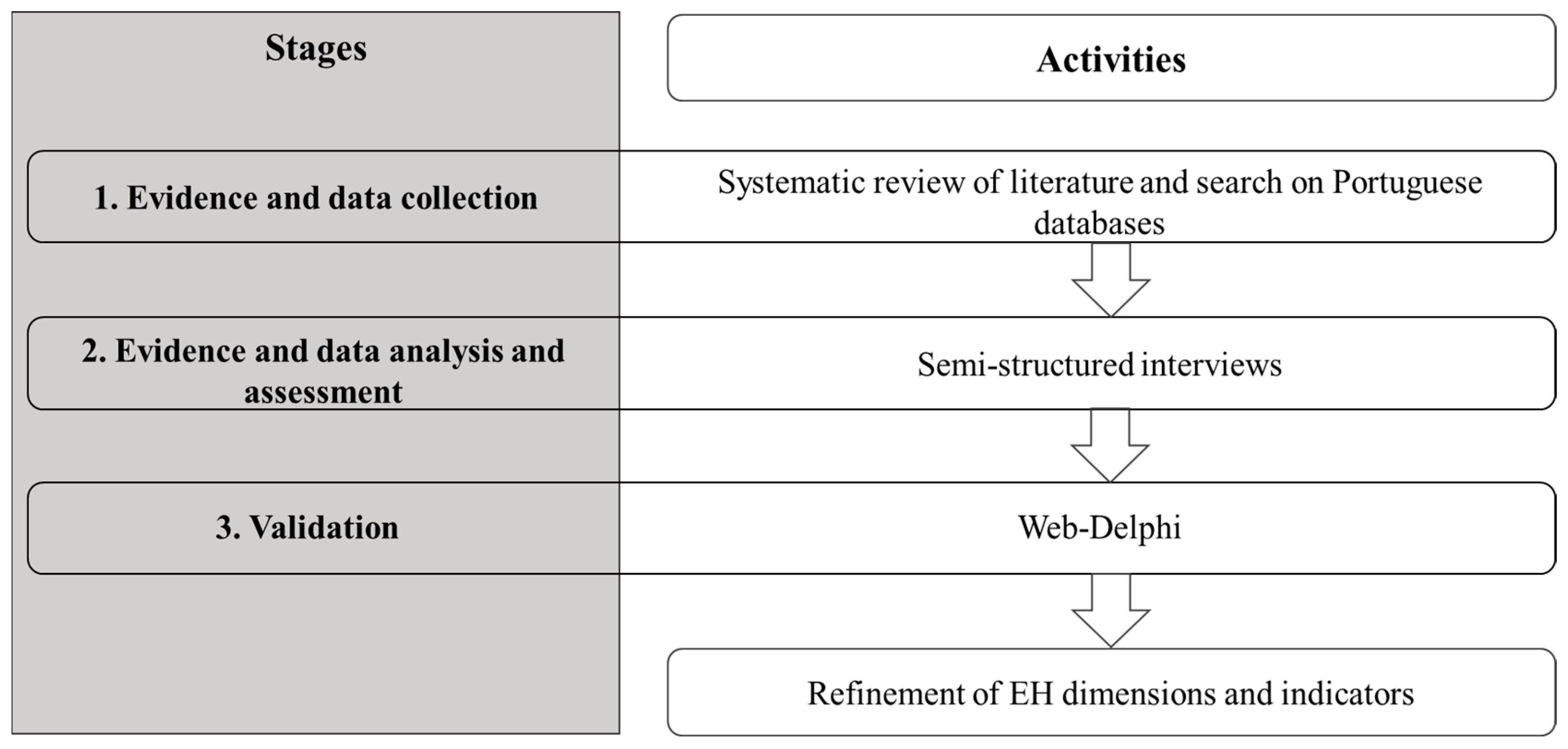
2. Materials and Methods
2.1. Evidence and Data Collection: Systematic Review of Literature and Search on Portuguese Databases
2.2. Evidence and Data Analysis and Assessment: Semi-Structured Interviews
2.3. Validation: Web-Delphi Process
2.3.1. Delphi Panel
2.3.2. Web-Delphi Design
2.3.3. Statistical Analysis
3. Results
3.1. Evidence and Data Collection: Systematic Review of Literature and Search of Portuguese Databases
3.2. Evidence and Data Analysis and Assessment: Semi-Structured Interviews
3.3. Validation: Web-Delphi Process
3.3.1. Panel Participation
3.3.2. Indicators
3.3.3. Group Agreement Analysis
4. Discussion
4.1. Methods
4.2. EH in Urban Settings
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development (Resolution A/RES/70/1 Adopted by the UN General Assembly on 25 September 2015); United Nations: New York, NY, USA, 2015; p. 35. [Google Scholar]
- Oliveira, G.M.; Vidal, D.G.; Ferraz, M.P.; Cabeda, J.; Pontes, M.; Maia, R.L.; Calheiros, J.M.; Barreira, E. Measuring Health Vulnerability: An Interdisciplinary Indicator Applied to Mainland Portugal. Int. J. Environ. Res. Public Health 2019, 16, 4121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, G.M.; Vidal, D.G.; Maia, R.L. Monitoring Portuguese living conditions at local scale: A case study based on sustainable development indicators. Int. J. Sustain. Dev. World Ecol. 2019, 27, 140–152. [Google Scholar] [CrossRef]
- Costa, C.; Santana, P.; Dimitroulopoulou, S.; Burström, B.; Borrell, C.; Schweikart, J.; Dzúrová, D.; Zangarini, N.; Katsouyanni, K.; Deboosere, P.; et al. Population Health Inequalities Across and Within European Metropolitan Areas through the Lens of the EURO-HEALTHY Population Health Index. Int. J. Environ. Res. Public Health 2019, 16, 836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez-Rubio, O.; Daher, C.; Fanjul, G.; Gascon, M.; Mueller, N.; Pajín, L.; Plasencia, A.; Rojas-Rueda, D.; Thondoo, M.; Nieuwenhuijsen, M.J. Urban health: An example of a “health in all policies” approach in the context of SDGs implementation. Glob. Health 2019, 15, 87. [Google Scholar] [CrossRef]
- Qiu, Y.; Lu, W.; Guo, J.; Sun, C.; Liu, X. Examining the Urban and Rural Healthcare Progress in Big Cities of China: Analysis of Monitoring Data in Dalian from 2008 to 2017. Int. J. Environ. Res. Public Health 2020, 17, 1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.Y.H.; Evans, M.B.; Wolff, P.E.; Gohlke, J.M. Environmental Health Priorities of Residents and Environmental Health Professionals: Implications for Improving Environmental Health Services in Rural Versus Urban Communities. J. Environ. Health 2017, 80, 28–36. [Google Scholar]
- United Nations, Department of Economic and Social Affiars, Population Division. The World’s Cities in 2018—Data Booklet; (ST/ESA/ SER.A/417); United Nations: New York, NY, USA, 2018. [Google Scholar]
- Sardain, A.; Tang, C.; Potvin, C. Towards a dashboard of sustainability indicators for Panama: A participatory approach. Ecol. Indic. 2016, 70, 545–556. [Google Scholar] [CrossRef] [Green Version]
- Ceretti, M.N.; Medeiros-Sousa, A.R.; Slovic, A.D. An Environmental Health Typology as a Contributor to Sustainable Regional Urban Planning: The Case of the Metropolitan Region of São Paulo (MRSP). Sustainability 2019, 11, 5800. [Google Scholar] [CrossRef] [Green Version]
- Guidotti, T.L. Environmental health needs a new paradigm, I. getting back in focus. Arch. Environ. Occup. Health 2018, 73, 267–269. [Google Scholar] [CrossRef] [Green Version]
- Brousmiche, D.; Occelli, F.; Genin, M.; Cuny, D.; Deram, A.; Lanier, C. Spatialized composite indices to evaluate environmental health inequalities: Meeting the challenge of selecting relevant variables. Ecol. Indic. 2020, 111, 106023. [Google Scholar] [CrossRef]
- Djalali, A.; Gianfrate, V.; Longo, D.; Vai, E. An advanced design approach to support urban transformations through multi-stakeholder collaborations. Strat. Des. Res. J. 2020, 12, 235–246. [Google Scholar] [CrossRef]
- Rydin, Y.; Bleahu, A.; Davies, M.; Dávila, J.D.; Friel, S.; De Grandis, G.; Groce, N.; Hallal, P.C.; Hamilton, I.; Howden-Chapman, P.; et al. Shaping cities for health: Complexity and the planning of urban environments in the 21st century. Lancet 2012, 379, 2079–2108. [Google Scholar] [CrossRef] [Green Version]
- Maroosi, M.; Mesdaghinia, A.; Alimohammadi, M.; Naddafi, K.; Mahvi, A.H.; Nodehi, R.N. Developing environmental health indicators [EHIs] for Iran based on the causal effect model. J. Environ. Health Sci. Eng. 2019, 17, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Lichtveld, M.; Covert, H.; Sherman, M.; Shankar, A.; Wickliffe, J.K.; Alcala, C.S. Advancing Environmental Health Literacy: Validated Scales of General Environmental Health and Environmental Media-Specific Knowledge, Attitudes and Behaviors. Int. J. Environ. Res. Public Health 2019, 16, 4157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyles, J.; Furgal, C. Indicators in Environmental Health: Identifying and Selecting Common Sets. Can. J. Public Health 2002, 93, S62–S67. [Google Scholar] [CrossRef]
- Hunter, D.J. Relationship between evidence and policy: A case of evidence-based policy or policy-based evidence? Public Health 2009, 123, 583–586. [Google Scholar] [CrossRef]
- Freitas, Â.; Santana, P.; Oliveira, M.D.; Almendra, R.; Costa, J.C.B.E.; Costa, C.A.B.E. Indicators for evaluating European population health: A Delphi selection process. BMC Public Health 2018, 18, 557. [Google Scholar] [CrossRef]
- Salgado, M.; Madureira, J.; Mendes, A.S.; Torres, A.; Teixeira, J.P.; Oliveira, M.D. Environmental determinants of population health in urban settings. A systematic review. BMC Public Health 2020, 20, 853. [Google Scholar] [CrossRef]
- Mason, K.; Lindberg, K.; Read, D.; Borman, B. The Importance of Using Public Health Impact Criteria to Develop Environmental Health Indicators: The Example of the Indoor Environment in New Zealand. Int. J. Environ. Res. Public Health 2018, 15, 1786. [Google Scholar] [CrossRef] [Green Version]
- Pineo, H.; Glonti, K.; Rutter, H.; Zimmermann, N.; Wilkinson, P.; Davies, M. Characteristics and use of urban health indicator tools by municipal built environment policy and decision-makers: A systematic review protocol. Syst. Rev. 2017, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Harbers, M.M.; Verschuuren, M.; De Bruin, A. Implementing the European Core Health Indicators (ECHI) in the Netherlands: An overview of data availability. Arch. Public Health 2015, 73, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badland, H.; Whitzman, C.; Lowe, M.; Davern, M.; Aye, L.; Butterworth, I.; Hes, D.; Giles-Corti, B. Urban liveability: Emerging lessons from Australia for exploring the potential for indicators to measure the social determinants of health. Soc. Sci. Med. 2014, 111, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Mao, F.; Li, Y.; Liu, J.; Zhang, Y.; Jiang, Y.; Zhao, D.; Chen, W.; Nicholas, S.; Zhang, Y.; et al. Construction of China cardiovascular health index. BMC Public Health 2018, 18, 937. [Google Scholar] [CrossRef] [Green Version]
- Firth, A.; O’Brien, S.M.; Guo, P.; Seymour, J.; Richardson, H.; Bridges, C.; Hocaoglu, M.B.; Grande, G.; Dzingina, M.; Higginson, I.J.; et al. Establishing key criteria to define and compare models of specialist palliative care: A mixed-methods study using qualitative interviews and Delphi survey. Palliat. Med. 2019, 33, 1114–1124. [Google Scholar] [CrossRef] [Green Version]
- Chun, S.; Nam, K. A public healthscape framework for assessing geriatric long-term care public hospitals in South Korea by a Delphi expert consultation. Build. Environ. 2019, 165, 106291. [Google Scholar] [CrossRef]
- Pikora, T.; Giles-Corti, B.; Bull, F.; Jamrozik, K.; Donovan, R. Developing a framework for assessment of the environmental determinants of walking and cycling. Soc. Sci. Med. 2003, 56, 1693–1703. [Google Scholar] [CrossRef]
- Ratnapradipa, D.; Brown, S.L.; Wodika, A.B. Examining the Breadth and Depth Of Environmental Health Through a Modified Delphi Technique. Am. J. Health Educ. 2011, 42, 50–57. [Google Scholar] [CrossRef]
- Allen, B.L.; Lees, J.; Cohen, A.K.; Jeanjean, M. Collaborative Workshops for Community Meaning-Making and Data Analyses: How Focus Groups Strengthen Data by Enhancing Understanding and Promoting Use. Int. J. Environ. Res. Public Health 2019, 16, 3352. [Google Scholar] [CrossRef] [Green Version]
- Ratnapradipa, D.; Middleton, W.K.; Wodika, A.B.; Brown, S.L.; Preihs, K. What does the public know about environmental health? A qualitative approach to refining an environmental health awareness instrument. J. Environ. Health 2015, 77, 22–28. [Google Scholar]
- Alshenqeeti, H. Interviewing as a Data Collection Method: A Critical Review. Engl. Linguist. Res. 2014, 3, 39–45. [Google Scholar] [CrossRef]
- Brewerton, P.; Millward, L. Organizational Research Methods; SAGE Publications, Ltd.: London, UK, 2001; pp. 67–113. [Google Scholar]
- Dalkey, N.; Helmer, O. An Experimental Application of the DELPHI Method to the Use of Experts. Manag. Sci. 1963, 9, 458–467. [Google Scholar] [CrossRef]
- Vieira, A.C.L.; Oliveira, M.D.; Costa, C.B.E. Enhancing knowledge construction processes within multicriteria decision analysis: The Collaborative Value Modelling framework. Omega 2020, 94, 102047. [Google Scholar] [CrossRef]
- Perveen, S.; Yigitcanlar, T.; Kamruzzaman, M.; Agdas, D. How can transport impacts of urban growth be modelled? An approach to consider spatial and temporal scales. Sustain. Cities Soc. 2020, 55, 102031. [Google Scholar] [CrossRef]
- Wang, W.-M.; Peng, H.-H. A Fuzzy Multi-Criteria Evaluation Framework for Urban Sustainable Development. Mathematics 2020, 8, 330. [Google Scholar] [CrossRef] [Green Version]
- Lisboa Green Capital 2020. Available online: https://lisboagreencapital2020.com/ (accessed on 29 June 2020).
- Subiyakto, A.; Ahlan, A.R.; Putra, S.J.; Kartiwi, M. Validation of Information System Project Success Model. SAGE Open 2015, 5, 215824401558165. [Google Scholar] [CrossRef] [Green Version]
- Petrisor, B.; Keating, J.; Schemitsch, E. Grading the evidence: Levels of evidence and grades of recommendation. Injury 2006, 37, 321–327. [Google Scholar] [CrossRef]
- Lawrence, R.J. Urban Environmental Health Indicators: Appraisal and Policy Directives. Rev. Environ. Health 2008, 23, 299–325. [Google Scholar] [CrossRef]
- PORDATA. Base de Dados de Portugal Contemporâneo. Available online: https://www.pordata.pt/Portugal (accessed on 30 September 2020).
- Van Dijk, J. Popularising Delphi method. Qual. Quant. 1989, 23, 189–203. [Google Scholar] [CrossRef]
- Barriball, K.L.; While, A. Collecting data using a semi-structured interview: A discussion paper. J. Adv. Nurs. 1994, 19, 328–335. [Google Scholar] [CrossRef]
- Dupras, C.; Birko, S.; Affdal, A.O.; Haidar, H.; Lemoine, M.-E.; Ravitsky, V. Governing the futures of non-invasive prenatal testing: An exploration of social acceptability using the Delphi method. Soc. Sci. Med. 2020, 112930. [Google Scholar] [CrossRef] [PubMed]
- Cerè, G.; Rezgui, Y.; Zhao, W. Urban-scale framework for assessing the resilience of buildings informed by a delphi expert consultation. Int. J. Disaster Risk Reduct. 2019, 36, 101079. [Google Scholar] [CrossRef]
- Taylor, S.J.; Bogdan, R. Introduction to Qualitative Research Methods: The Search for Meanings; John Wiley &Sons, Inc.: New York, NY, USA, 1984. [Google Scholar]
- Adam, L.; Jones, T.; Brömmelstroet, M.T. Planning for cycling in the dispersed city: Establishing a hierarchy of effectiveness of municipal cycling policies. Transportation 2018, 47, 503–527. [Google Scholar] [CrossRef] [Green Version]
- Degeling, C.; Johnson, J.; Ward, M.; Wilson, A.; Gilbert, G. A Delphi Survey and Analysis of Expert Perspectives on One Health in Australia. EcoHealth 2017, 14, 783–792. [Google Scholar] [CrossRef] [Green Version]
- Nor, M.Z. Developing a preliminary questionnaire for the faculty development programme needs of medical teachers using Delphi technique. J. Taibah Univ. Med Sci. 2019, 14, 495–501. [Google Scholar] [CrossRef]
- Von Der Gracht, H.A. Consensus measurement in Delphi studies. Technol. Forecast. Soc. Chang. 2012, 79, 1525–1536. [Google Scholar] [CrossRef]
- Cullerton, K.; Adams, J.; Francis, O.; Forouhi, N.; White, M. Building consensus on interactions between population health researchers and the food industry: Two-stage, online, international Delphi study and stakeholder survey. PLoS ONE 2019, 14, e0221250. [Google Scholar] [CrossRef] [Green Version]
- Welphi. 2019. Available online: http://www.welphi.com/ (accessed on 2 April 2020).
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–10015. [Google Scholar]
- Dalkey, N.; Brown, B.; Cochran, S. Use of self-ratings to improve group estimates. Technol. Forecast. 1970, 1, 283–291. [Google Scholar] [CrossRef]
- Meijering, J.V.; Kampen, J.K.; Tobi, H. Quantifying the development of agreement among experts in Delphi studies. Technol. Forecast. Soc. Chang. 2013, 80, 1607–1614. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Tisch, C.; Pearson, A.L.; Kingham, S.; Borman, B.; Briggs, D. Environmental health indicators: A review of initiatives worldwide. Manag. Environ. Qual. Int. J. 2014, 25, 446–466. [Google Scholar] [CrossRef]
- Goldman, L.; Coussens, C.M. Environmental Health Indicators: Bridging the Chasm of Public Health and the Environment—Workshop Summary; National Academic Press: Washington, DC, USA, 2004. [Google Scholar]
- Frumkin, H. Environmental Health: From Global to Local, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2010. [Google Scholar]
- Luo, R.; Zhang, C.; Liu, Y. Health Risk Assessment Indicators for the Left-Behind Elderly in Rural China: A Delphi Study. Int. J. Environ. Res. Public Health 2020, 17, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson-Nuñez, J.; Walters, J.P.; Charpentier, D. Exploring the challenges to sustainable rural drinking water services in Chile. Water Policy 2019, 21, 1251–1265. [Google Scholar] [CrossRef]
- Home, R.; Vieli, L. Psychosocial outcomes as motivations for urban gardening: A cross-cultural comparison of Swiss and Chilean gardeners. Urban For. Urban Green. 2020, 52, 126703. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J. Urban and transport planning, environmental exposures and health-new concepts, methods and tools to improve health in cities. Environ. Health 2016, 15 (Suppl. 1), 161–171. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, J.P.; Palma, P.; Simoes, S. Energy poverty vulnerability index: A multidimensional tool to identify hotspots for local action. Energy Rep. 2019, 5, 187–201. [Google Scholar] [CrossRef]
- Wu, Y.; Li, R.; Cui, L.; Meng, Y.; Cheng, H.; Fu, H. The high-resolution estimation of sulfur dioxide (SO2) concentration, health effect and monetary costs in Beijing. Chemosphere 2020, 241, 125031. [Google Scholar] [CrossRef]
- Dzhambov, A.; Markevych, I.; Tilov, B.; Dimitrova, D.D. Residential greenspace modifies the effect of road traffic noise exposure on mental health in youth. Eur. J. Public Health 2017, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Strosnider, H.; Kennedy, C.; Monti, M.; Yip, F. Rural and Urban Differences in Air Quality, 2008–2012, and Community Drinking Water Quality, 2010–2015—United States. MMWR. Surveill. Summ. 2017, 66, 1–10. [Google Scholar] [CrossRef]
- Da Silva, R.T.; Fleskens, L.; Van Delden, H.; Van Der Ploeg, M. Incorporating soil ecosystem services into urban planning: Status, challenges and opportunities. Landsc. Ecol. 2018, 33, 1087–1102. [Google Scholar] [CrossRef] [Green Version]
- Calzolari, C.; Tarocco, P.; Lombardo, N.; Marchi, N.; Ungaro, F. Assessing soil ecosystem services in urban and peri-urban areas: From urban soils survey to providing support tool for urban planning. Land Use Policy 2020, 99, 105037. [Google Scholar] [CrossRef]


{kind=link}
| Stage 2 | Stage 3 | ||
|---|---|---|---|
| Item | Interviews | 1st Round Web-Delphi | 2nd Round Web-Delphi |
| Gender, n (%) | |||
| Female | 6 (50%) | 14 (48%) | 10 (45%) |
| Male | 6 (50%) | 15 (51%) | 12 (55%) |
| Main area of expertise, n (%) | |||
| Built environment | 3 (25%) | 5 (17%) | 5 (23%) |
| Natural environment | 3 (25%) | 9 (31%) | 5 (23%) |
| Environmental health | 3 (25%) | 10 (35%) | 8 (36%) |
| National health regulation institutions | 3 (25%) | 5 (17%) | 4 (18%) |
| Built Environment Determinant | ||||
|---|---|---|---|---|
| Dimension | Indicator | Disagreement (%) | Agreement (%) | Included |
| Green Spaces | Number of zoos, botanic parks, and aquariums * | 75.0 | 0 | No |
| Protected area surface (km2) | 83.4 | 0 | No | |
| Protected area proportion (km2) | 75.0 | 0 | No | |
| Number of gardens and parks | 75.0 | 0 | No | |
| Area of leisure parks and gardens (m2) | 0 | 83.3 | Yes | |
| Area of community gardens (m2) | 0 | 83.3 | Yes | |
| Housing | Number of classic family housing buildings * | 83.3 | 0 | No |
| Number of buildings by geographic location and type * | 75.0 | 0 | No | |
| Mobility | Built-up areas (km2) * | 66.7 | 0 | No |
| Road vehicles by type and fuel * | 16.7 | 58.4 | Yes | |
| Traffic accidents with victims/1000 inhabitants | 66.7 | 0 | No | |
| Cycle roads (km) | 0 | 75.0 | Yes | |
| Road network (km) | 0 | 75.0 | Yes | |
| Proportion of resident population using individual mode of transport while commuting * | 66.7 | 0 | No | |
| Proportion of resident population using public transport mode during commuting * | 58.3 | 0 | No | |
| Safety | Police-reported crimes/1000 inhabitants * | 58.3 | 0 | No |
| Sanitation | Urban waste collection * | 58.3 | 0 | No |
| Population served by wastewater drainage systems * | 58.3 | 0 | No | |
| Natural Environment Determinant | ||||
| Air quality | PM2.5 (particulate matter) | 0 | 83.3 | Yes |
| PM10 (particulate matter) | 0 | 83.3 | Yes | |
| O3 (ozone) | 0 | 83.3 | Yes | |
| NO2 (nitrogen dioxide) | 0 | 83.3 | Yes | |
| NOx (nitrogen oxides) | 8.33 | 75.0 | Yes | |
| SO2 (sulfur dioxide) | 0 | 83.3 | Yes | |
| CO (carbon monoxide) | 0 | 83.3 | Yes | |
| C6H6 (benzene) | 8.33 | 75.0 | Yes | |
| Noise | Exposure to high noise | 75.0 | 16.7 | No |
| Suffering from noise * | 66.7 | 25.0 | No | |
| Lden (day-evening-night equivalent sound level) | 0 | 83.3 | Yes | |
| Ln (day-night equivalent sound level) | 0 | 83.3 | Yes | |
| Water quality | “Água segura” *,a | 0 | 91.7 | Yes |
| Public water supply * | 58.3 | 0 | No | |
| Soil | Soil organic carbon content *,b | 100 | 0 | No |
| Soil sealing index *,c | 75.0 | 16.7 | No | |
| Determinant | Dimension | Indicators | Agreement Rate (%) | Inclusion By |
|---|---|---|---|---|
| Built environment | Green spaces | Area of leisure parks and gardens | 63.6 | Absolute |
| Area of community gardens | 54.5 | Qualified | ||
| Housing | Energy poverty vulnerability index | 95.5 | Qualified | |
| Mobility | Cycle roads | 86.4 | Qualified | |
| Number of road vehicles | 81.8 | Qualified | ||
| Road network | 77.3 | Qualified | ||
| Natural environment | Air quality | PM2.5 | 86.4 | Absolute |
| PM10 | 63.6 | Absolute | ||
| O3 | 63.6 | Absolute | ||
| NO2 | 63.6 | Absolute | ||
| NOx | 59.1 | Absolute | ||
| SO2 | 86.4 | Qualified | ||
| CO | 59.1 | Absolute | ||
| C6H6 | 54.5 | Absolute | ||
| Noise | Lden | 90.9 | Qualified | |
| Ln | 63.6 | Absolute | ||
| Water quality | “Água segura” | 95.5 | Absolute |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salgado, M.; Vieira, A.C.L.; Torres, A.; Oliveira, M.D. Selecting Indicators to Monitor and Assess Environmental Health in a Portuguese Urban Setting: A Participatory Approach. Int. J. Environ. Res. Public Health 2020, 17, 8597. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228597
Salgado M, Vieira ACL, Torres A, Oliveira MD. Selecting Indicators to Monitor and Assess Environmental Health in a Portuguese Urban Setting: A Participatory Approach. International Journal of Environmental Research and Public Health. 2020; 17(22):8597. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228597
Chicago/Turabian StyleSalgado, Marta, Ana C. L. Vieira, Anália Torres, and Mónica D. Oliveira. 2020. "Selecting Indicators to Monitor and Assess Environmental Health in a Portuguese Urban Setting: A Participatory Approach" International Journal of Environmental Research and Public Health 17, no. 22: 8597. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228597