Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic



Abstract
:1. Introduction
2. Theory and Hypotheses
2.1. Preventive Behavior in the Case of a Pandemic
2.2. Health Belief Model and Resource Theory
2.3. Hypotheses from the HBM
2.3.1. Perceived Susceptibility
2.3.2. Perceived Severity
2.3.3. Perceived Benefits Versus Perceived Barriers
2.3.4. Self-Efficacy
2.3.5. Cues to Action
2.4. Hypotheses Based on Resource Theory
2.4.1. Income
2.4.2. Education
2.4.3. Knowledge
2.4.4. Personal Health Status
2.4.5. Social Support
3. Sample and Measures
4. Analysis and Findings
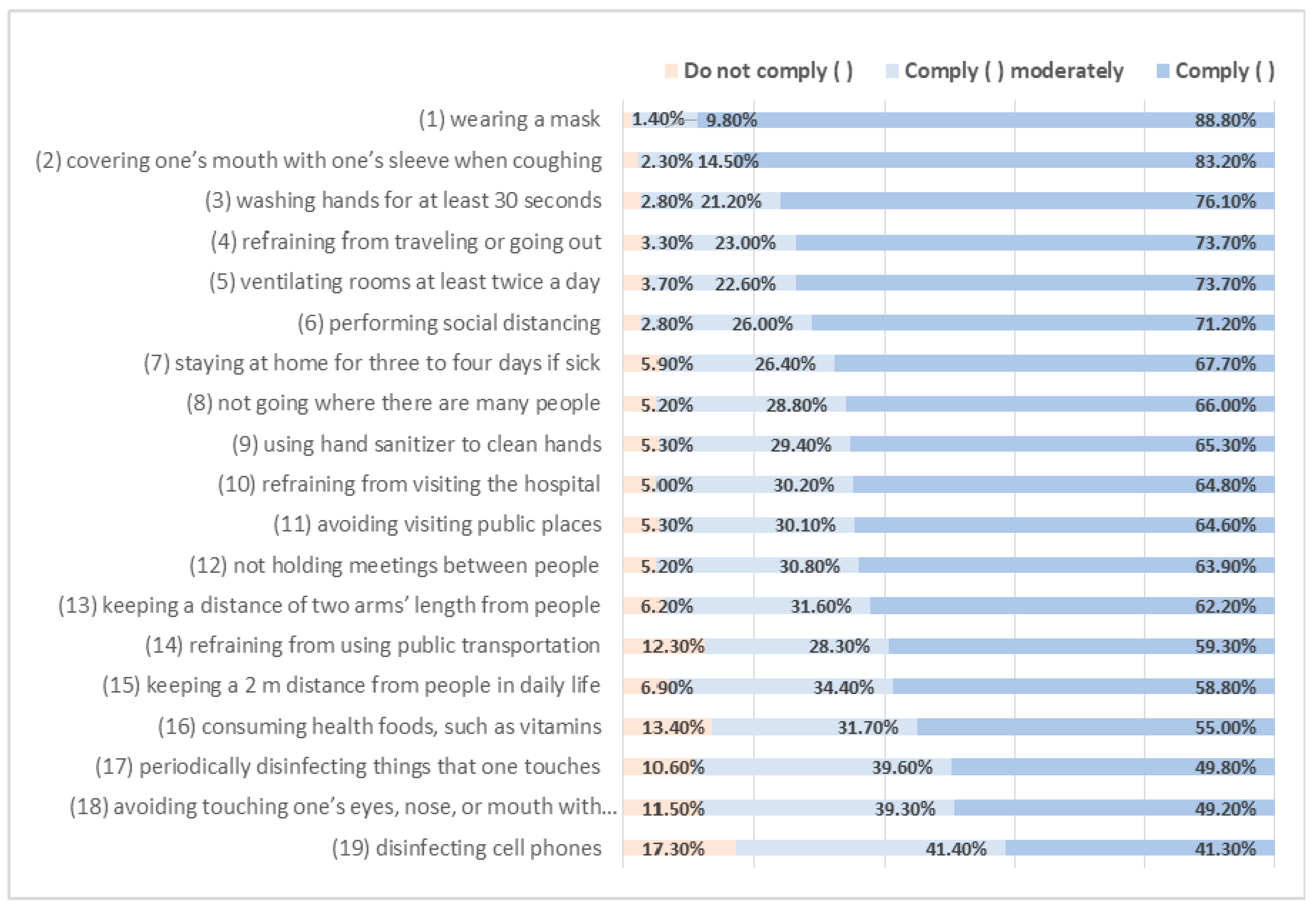
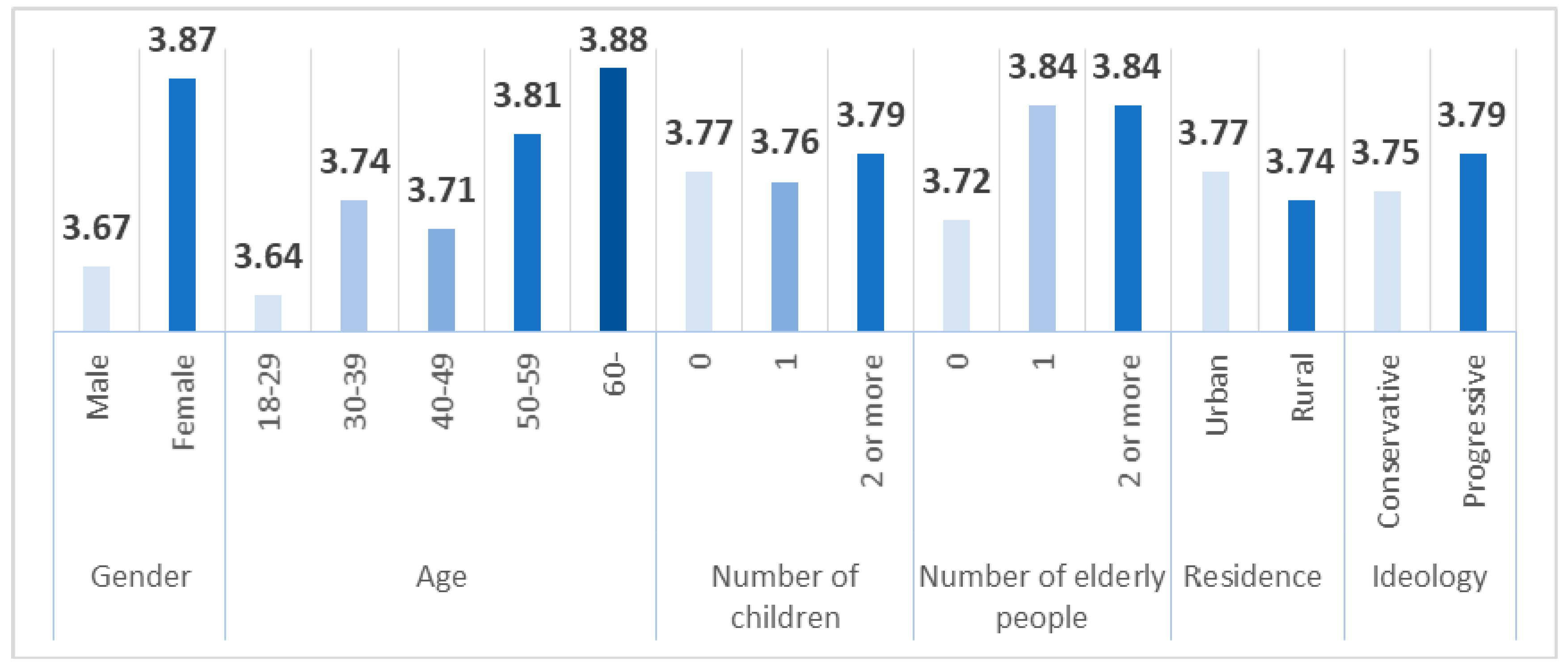
4.1. Descriptive Analysis
4.2. Regression Analysis
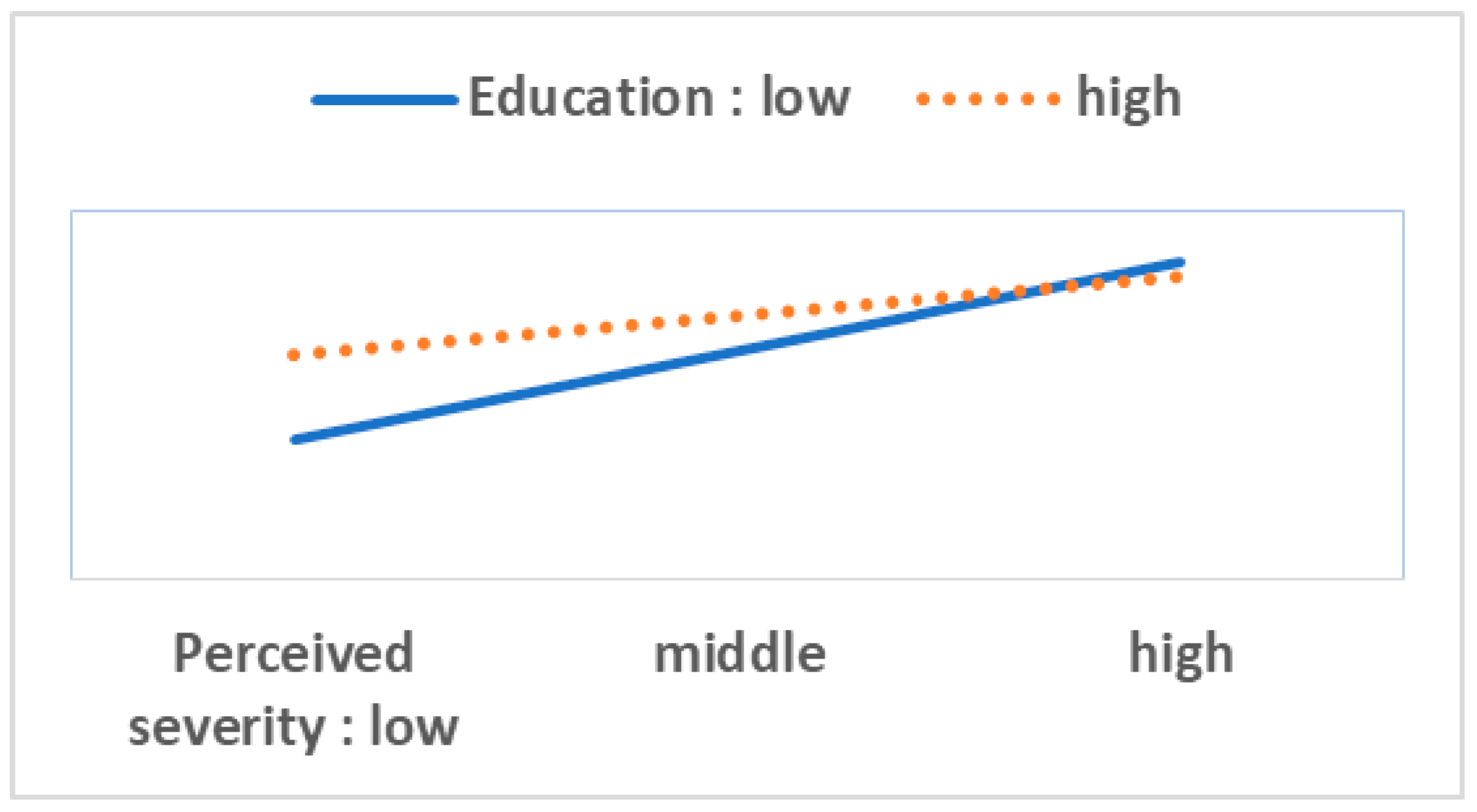
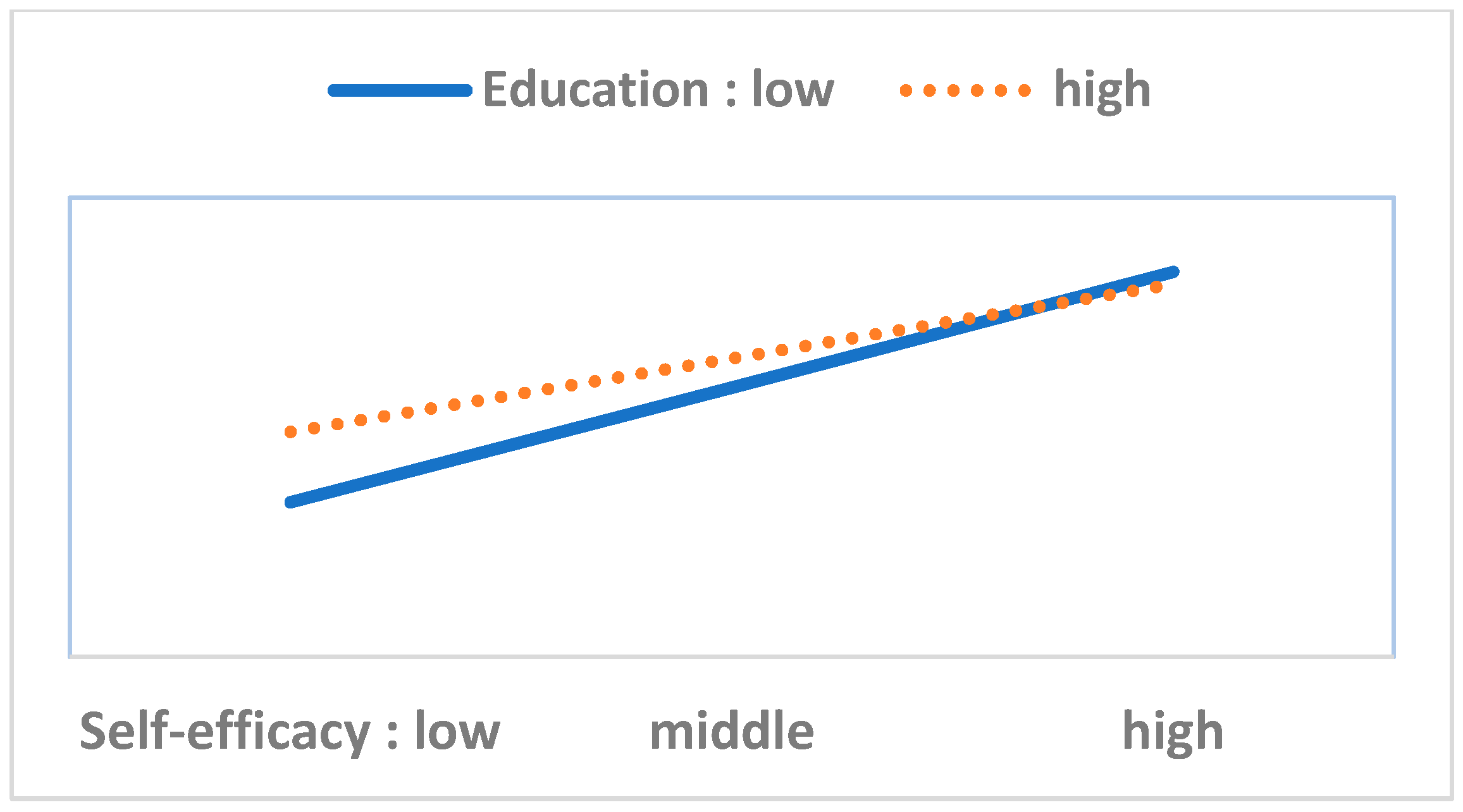
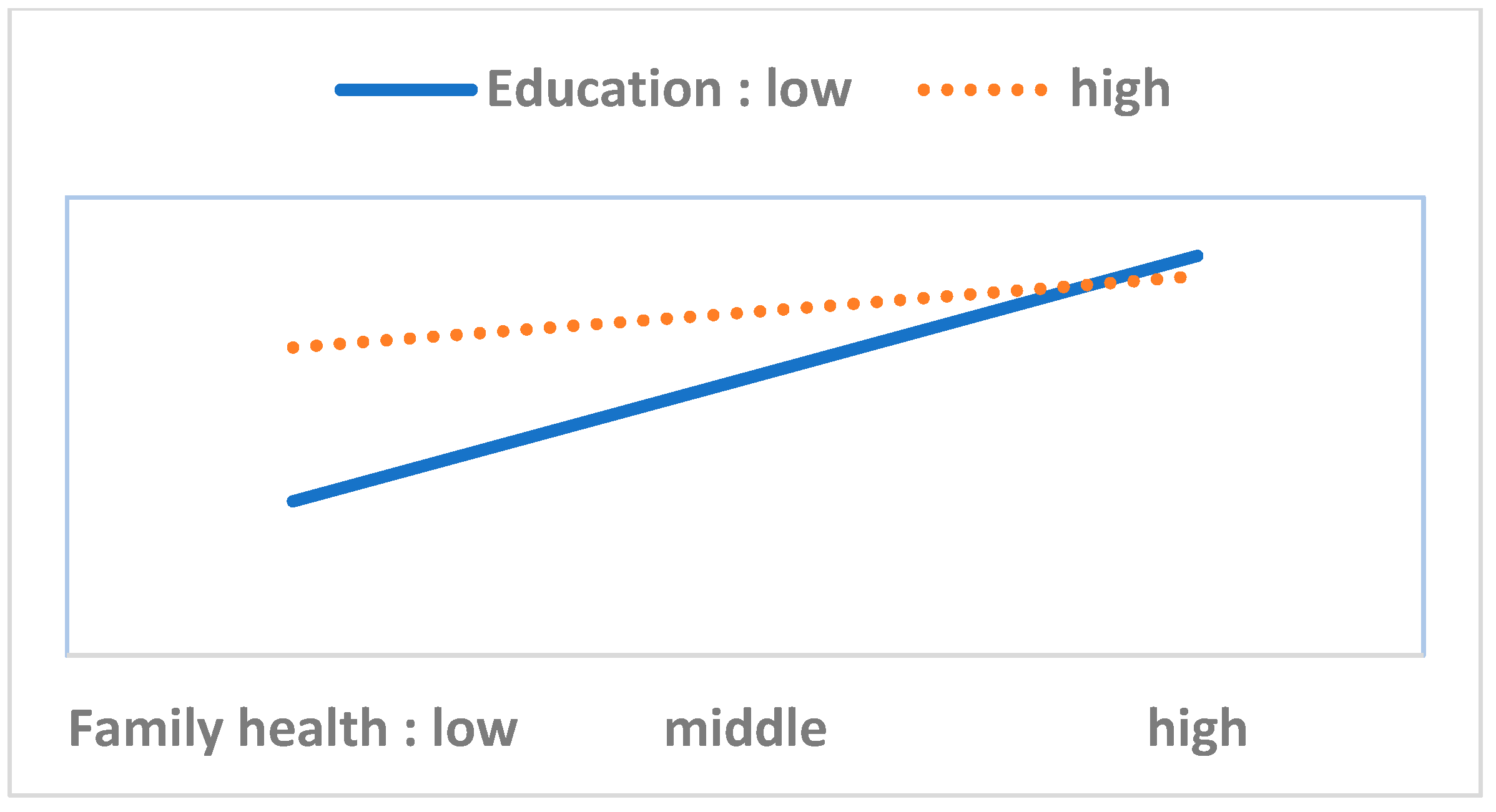
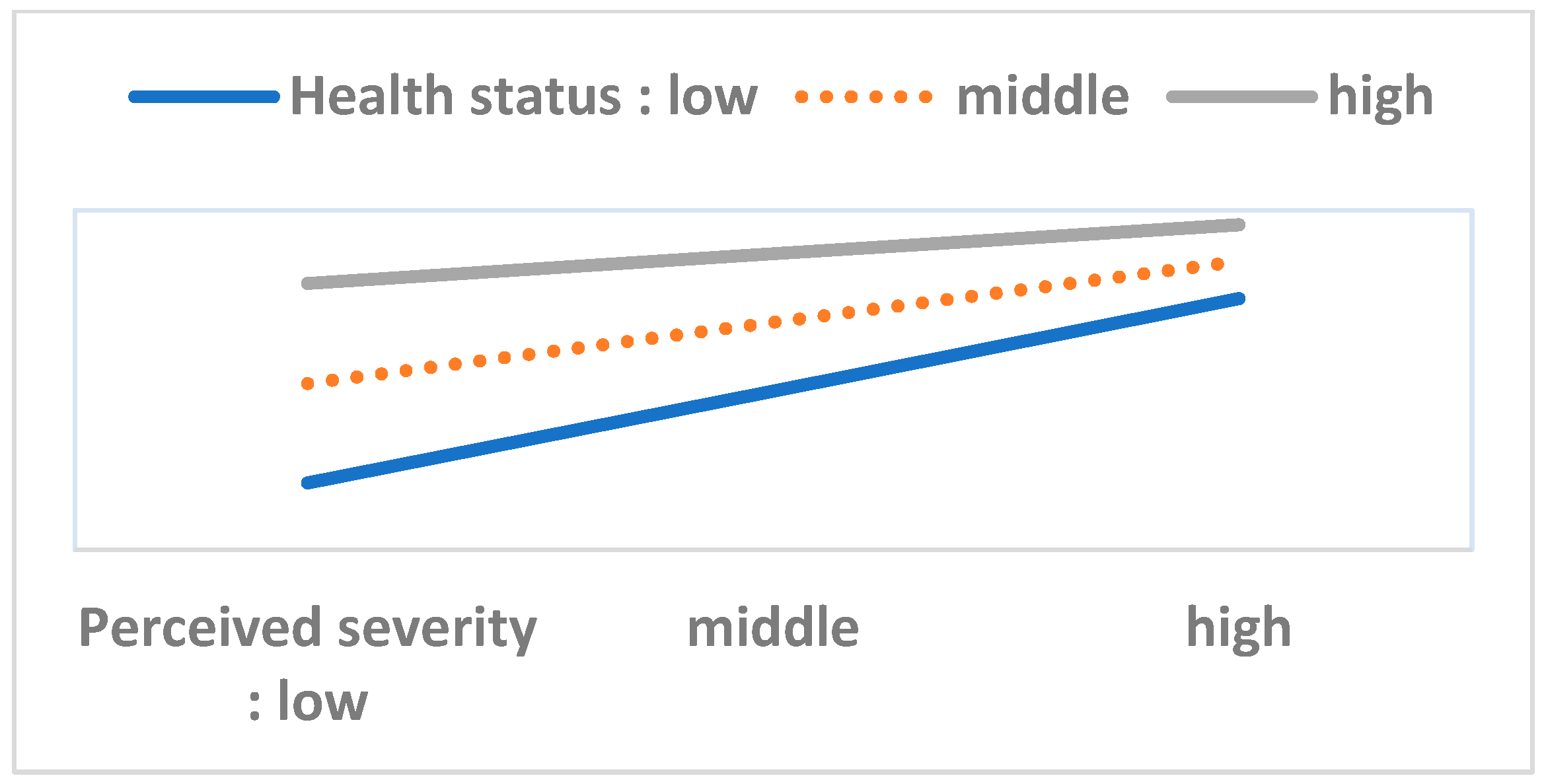
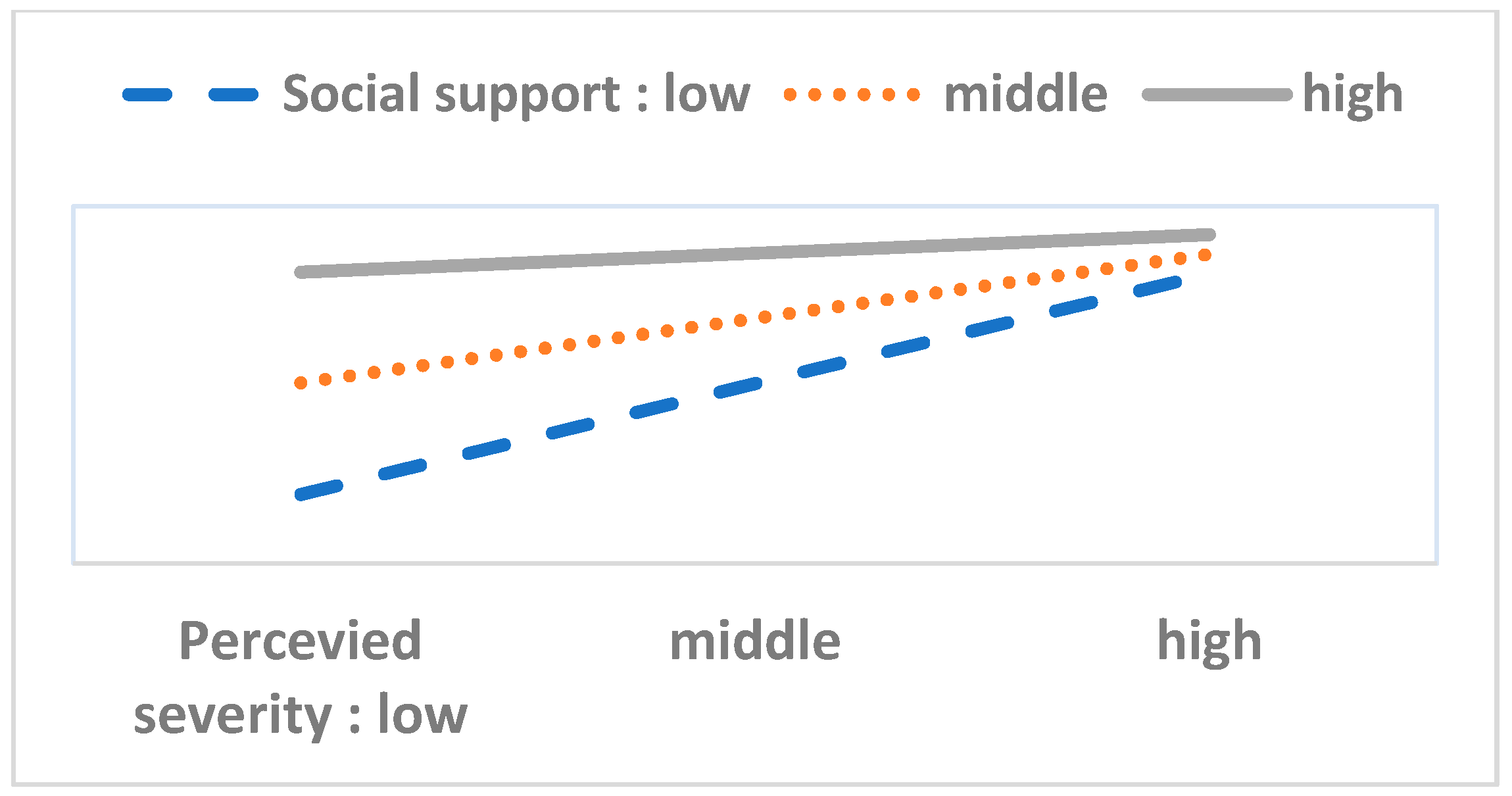
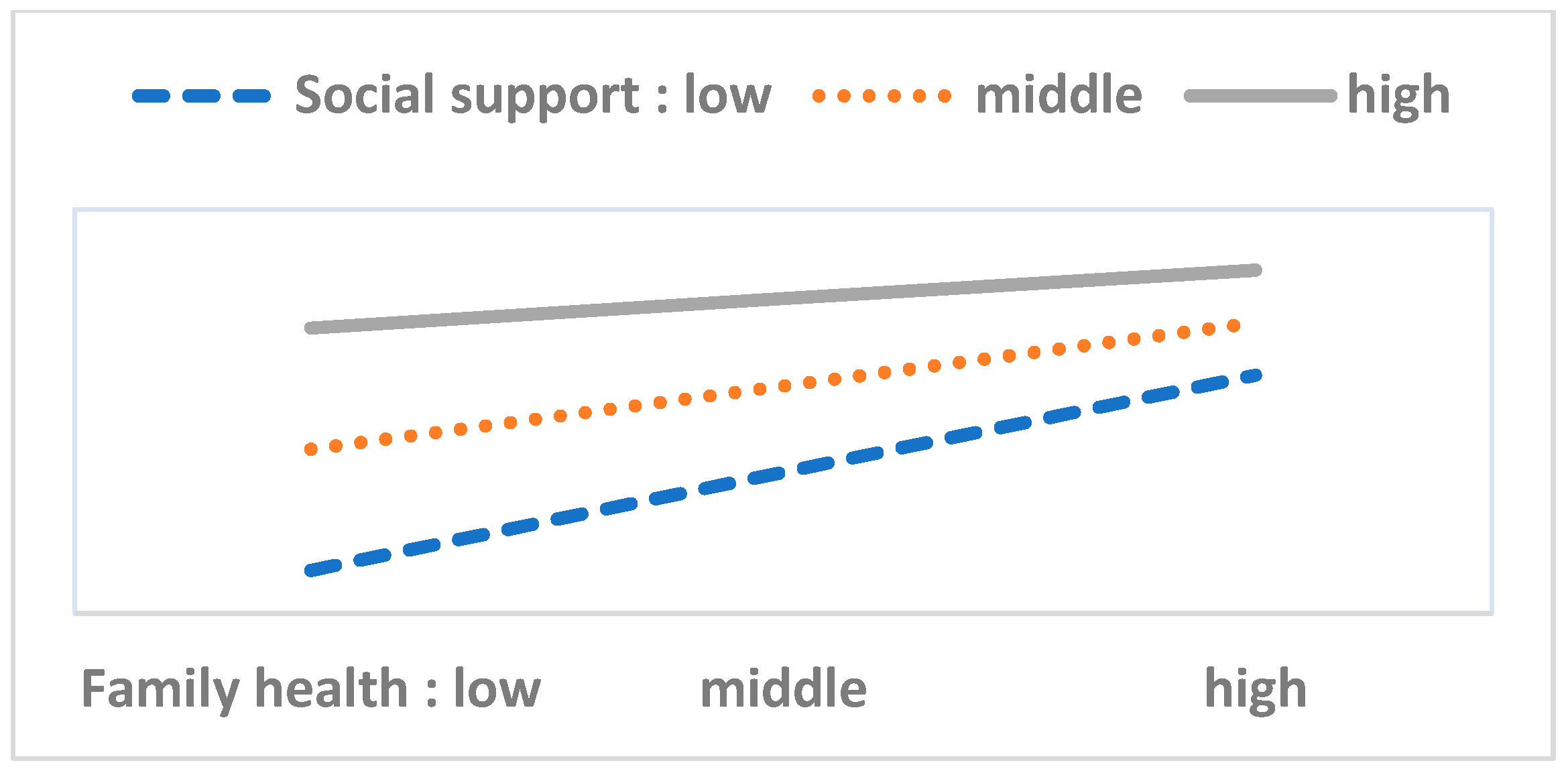
4.3. Moderating Analysis
5. Discussion and Implications
6. Limitations and Future Research
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 4 September 2020).
- Cvetković, V.M.; Nikolić, N.; Nenadić, U.R.; Öcal, A.K.; Noji, E.; Zečević, M. Preparedness and Preventive Behaviors for a Pandemic Disaster Caused by COVID-19 in Serbia. Int. J. Environ. Res. Public Health 2020, 17, 4124. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhao, X.; Feng, Q.; Liu, L.; Yao, Y.; Shi, J. Psychological assistance during the coronavirus disease 2019 outbreak in China. J. Health Psychol. 2020, 25, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.; Kim, Y.K.; Hua, J. Governance, technology and citizen behavior in pandemic: Lessons from COVID-19 in East Asia. Prog. Disaster Sci. 2020, 6, 100090. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Chan, H.H.; Yi, Y.Y.; Tang, A.; Wei, W.I.; Wong, Y.S.J. Community responses during the early phase of the COVID-19 epidemic in Hong Kong: Risk perception, information exposure and preventive measures. MedRxiv 2020, 26, 200500. [Google Scholar]
- Leung, G.; Lam, T.; Ho, L.; Ho, S.; Chan, B.; Wong, I.; Hedley, A.J.; Health, C. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. J. Epidemiol. Community Health 2003, 57, 857–863. [Google Scholar] [CrossRef] [Green Version]
- Seale, H.; Heywood, A.E.; McLaws, M.L.; Ward, K.F.; Lowbridge, C.P.; Van, D. Why do I need it? I am not at risk! Public perceptions towards the pandemic (H1N1) 2009 vaccine. BMC Infect. Dis. 2010, 10, 99. [Google Scholar] [CrossRef] [Green Version]
- Jose, R.; Narendran, M.; Bindu, A.; Beevi, N.; Manju, L.; Benny, P.V. Public perception and preparedness for the pandemic COVID 19: A Health Belief Model approach. Clin. Epidemiol. Glob. Health 2020. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Robbins, E.H.R.; Barger, L.K.; Facer-Childs, E.R.; Rajaratnam, S.M.W. COVID-19: Public compliance with and public support for stay-at-home mitigation strategies. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Brienen, N.C.J.; Timen, A.; Wallinga, J.; Steenbergen, J.E.V.; Teunis, P.F.M. The effect of mask use on the spread of influenza during a pandemic. Risk Anal. 2010, 30, 1210–1218. [Google Scholar] [CrossRef]
- Lau, J.T.; Griffiths, S.; Choi, K.C.; Lin, C. Prevalence of preventive behaviors and associated factors during early phase of the H1N1 influenza epidemic. Am. J. Infect. Control 2010, 38, 374–380. [Google Scholar] [CrossRef]
- Barr, M.; Raphael, B.; Taylor, M.; Stevens, G.; Jorm, L.; Giffin, M.; Lujic, S. Pandemic influenza in Australia: Using telephone surveys to measure perceptions of threat and willingness to comply. BMC Infect. Dis. 2008, 8, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, B.L.; Luo, W.; Li, H.M.; Zhang, Q.Q.; Li, W.T.; Li, W. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Chen, H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. [Google Scholar] [CrossRef] [PubMed]
- Shahnazi, H.; Ahmadi-Livani, M.; Pahlavanzadeh, B.; Rajabi, A.; Hamrah, M.; Charkazi, A. Assessing preventive health behaviors from COVID-19 Based on the Health Belief Model (HBM) among people in Golestan province: A cross-sectional study in Northern Iran. Res. Square 2020. [Google Scholar] [CrossRef]
- Lee, M.; You, M. Psychological and Behavioral Responses in South Korea During the Early Stages of Coronavirus Disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 2977. [Google Scholar] [CrossRef] [PubMed]
- Duan, T.; Jiang, H.; Deng, X.; Zhang, Q.; Wang, F. Government intervention, risk perception, and the adoption of protective action recommendations: Evidence from the COVID-19 prevention and control experience of china. Int. J. Environ. Res. Public Health 2020, 17, 3387. [Google Scholar] [CrossRef]
- Janz, N.K.; Marshall, H.B. The Health Belief Model: A decade later. Health Educ. Behav. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I. Historical origins of the Health Belief Model. Health Educ. Behav. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Carpenter, C. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [Green Version]
- Bränström, R.; Kristjansson, S.; Ullen, H. Risk perception, optimistic bias, and readiness to change sun related behavior. Eur. J. Public Health 2006, 16, 492–497. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Cheong, H.K.; Son, D.Y.; Kim, S.U.; Ha, C.M. Perceptions and behaviors related to hand hygiene for the prevention of H1N1 influenza transmission among Korean university students during the peak pandemic period. BMC Infect. Dis. 2010, 10, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durham, D.P.; Casman, E.A.; Albert, S.M. Deriving behavior model parameters from survey data: Self-protective behavior adoption during the 2009–2010 influenza a (H1N1) pandemic. Risk Anal. 2012, 32, 2020–2031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brug, J.; Aro, A.R.; Richardus, J.H. Risk perceptions and behavior: Towards pandemic control of emerging infectious diseases. Int. J. Behav. Med. 2009, 16, 3–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppin, A.; Aro, A.R. Risk perceptions related to SARS and avian influenza: Theoretical foundations of current empirical research. Int. J. Behav. Med. 2009, 16, 7–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foa, U.G.; Converse, J., Jr.; Törnblom, K.Y.; Foa, E.B. (Eds.) Resource Theory: Explorations and Applications; Academic Press: Cambridge, MA, USA, 1993. [Google Scholar]
- Lin, N. Social resources: A theory of social capital. Rev. Fr. Sociol. 1995, 36, 685–704. [Google Scholar] [CrossRef]
- Snyder, K. Risk perception and resource security for female agricultural workers. In Socioeconomic Aspects of Human Behavioral Ecology (Research in Economic Anthropology); Alvard, M., Ed.; Emerald Group Publishing Limited: Bingley, UK, 2004; Volume 23, pp. 271–292. [Google Scholar] [CrossRef]
- Solar, O.; Irwin, A. Social Determinants of Health Discussion Paper 2(Policy and Practice). In A Conceptual Framework for Action on the Social Determinants of Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Graham, H.; Kelly, M. Health Inequalities: Concepts, Frameworks and Policy; Health Development Agency: London, UK, 2004. [Google Scholar]
- Adler, N.E.; Stewart, J.; Cohen, S.; Cullen, M.; Roux, A.D.; Dow, W. MacArthur Foundation Research Network on Socioeconomic Status and Health; Reaching for a Healthier life: Facts on Socioeconomic Status and Health in the US; MacArthur Foundation: Chicago, IL, USA, 2007; p. 43. [Google Scholar]
- Enarson, E.; Walsh, S. Integrating Emergency Management and high-Risk Populations: Survey Report and Action Recommendations, Canadian Red Cross. 2007. Available online: http://www.redcross.ca/cmslib/general/dm_high_risk_populations.pdf (accessed on 30 May 2018).
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an effective health interventions design: An extension of the health belief model. Online J. Public Health Inform. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Harrison, J.A.; Mullen, P.D.; Green, L.W. A meta-analysis of studies of the Health Belief Model with adults. Health Educ. Res. 1992, 7, 107–116. [Google Scholar] [CrossRef] [PubMed]
- LaMorte, W.W. Behavioral Change Models. Available online: https://sphweb.bumc.bu.edu/otlt/mph-modules/sb/behavioralchangetheories/ (accessed on 19 December 2019).
- Cummings, K.M.; Becker, M.H.; Maile, M.C. Bringing the models together: An empirical approach to combining variables used to explain health actions. J. Behav. Med. 1980, 3, 123–145. [Google Scholar] [CrossRef] [Green Version]
- Armitage, C.J.; Conner, M. Social cognition models and health behaviour: A structured review. Psychol. Health 2000, 15, 173–189. [Google Scholar] [CrossRef] [Green Version]
- Prati, G.; Pietrantoni, L.; Zani, B. A social-cognitive model of pandemic influenza H1N1 risk perception and recommended behaviors in Italy. Risk Anal. 2010, 31, 645–656. [Google Scholar] [CrossRef] [PubMed]
- Karen, G.; Barbara, R.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020. [Google Scholar] [CrossRef]
- Conner, M. Health behaviors. In International Encyclopedia of the Social & Behavioral Sciences; Smelser, N.J., Baltes, P.B., Eds.; Pergamon: Oxford, UK, 2001. [Google Scholar] [CrossRef]
- Farooq, A.; Laato, S.; Islam, A. Impact of online information on self-isolation intention during the COVID-19 Pandemic: Cross-sectional study. J. Med. Internet Res. 2020, 22, e19128. [Google Scholar] [CrossRef] [PubMed]
- Raifman, M.A.; Raifman, J.R. Disparities in the population at risk of severe illness from COVID-19 by race/ethnicity and income. Am. J. Prev. Med. 2020, 59, 137–139. [Google Scholar] [CrossRef] [PubMed]
- The European Union for Georgia. Monitory Knowledge, Risk Perception, Preventive Behaviors and Public Trust in the Current Coronavirus Outbreak in Georgia. 2020. Available online: https://www.unicef.org/georgia/media/4736/file/COVID-19-Study-Analytical-Report-1-st-2nd-and-3rd-waves-Eng.pdf (accessed on 1 September 2020).
- Goodwin, R.; Haque, S.; Neto, F.; Myers, L.B. Initial psychological responses to Influenza A, H1N1 (“Swine flu”). BMC Infect. Dis. 2009, 9, 166. [Google Scholar] [CrossRef] [Green Version]
- Ibuka, Y.; Chapman, G.B.; Meyers, L.A.; Li, M.; Galvani, A.P. The dynamics of risk perceptions and precautionary behavior in response to 2009 (H1N1) pandemic influenza. BMC Infect. Dis. 2010, 10, 296. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator—Mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Fischhoff, B.; Slovic, P.; Lichtenstein, S.; Read, S.; Combs, B. How safe is safe enough? A psychometric study of attitudes towards technological risks and benefits. Policy Sci. 1978, 9, 127–152. [Google Scholar] [CrossRef]
- Slovic, P. The Perception of Risk; Routledge Taylor & Francis Group: New York, NY, USA, 2000. [Google Scholar]
- Stern, P.C.; Dietz, T.; Abel, T.; Guagnano, G.A.; Kalof, L. A value-belief-norm theory of support for social movements: The case of environmentalism. Hum. Ecol. Rev. 1999, 6, 81–97. [Google Scholar]
- Kasperson, R.E.; Renn, O.; Slovic, P.; Brown, H.S.; Emel, J.; Goble, R.; Kasperson, J.X.; Ratick, S. The social amplification of risk: A conceptual framework. Risk Anal. 1988, 8, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Owuor, C.O. Implications of Using Likert Data in Multiple Regression Analysis. Ph.D. Thesis, The University of British Columbia, Vencover, BC, Canada, 2001. [Google Scholar]
- Lubke, G.H.; Muthen, B.O. Applying multigroup confirmatory factor models for continuous outcomes to Likert scale data complicates meaningful group comparisons. Struct. Equ. Modeling 2004, 11, 514–534. [Google Scholar] [CrossRef]
- Kim, S. Irresolvable cultural conflicts and conservation/development arguments: Analysis of Korea’s Saemangeum project. Policy Sci. 2003, 36, 125–149. [Google Scholar] [CrossRef]
- Kim, S.; Kim, H. Does cultural capital matter? Cultural divide and quality of life. Soc. Indic. Res. 2009, 93, 295–313. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S. Exploring the effect of four factors on affirmative action programs for women. Asian J. Women’s Stud. 2014, 20, 31–70. [Google Scholar]
- Kim, S.; Kim, S. Impact of the Fukushima nuclear accident on belief in rumors: The role of risk perception and communication. Sustainability 2017, 9, 2188. [Google Scholar] [CrossRef] [Green Version]
- Ryu, Y.; Kim, S.; Kim, S. Does Trust Matter? Analyzing the impact of trust on the perceived risk and acceptance of nuclear power energy. Sustainability 2018, 10, 758. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Kim, S. Analysis of the impact of values and perception on climate change skepticism and its implication for public policy. Climate 2018, 6, 99. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.-A.; Kim, S.; Lee, J.E. Analyzing the determinants of individual action on climate change by specifying the roles of six values in South Korea. Sustainability 2019, 11, 1834. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Lee, J.E.; Kim, D. Searching for the next new energy in energy transition: Comparing the impacts of economic incentives on local acceptance of fossil fuels, renewable, and nuclear energies. Sustainability 2019, 11, 2037. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.J.; Kim, S.; Kim, S. Searching for new directions for energy policy: Testing three causal models of risk perception, attitude, and behavior in nuclear energy context. Int. J. Environ. Res. Public Health 2020, 17, 7403. [Google Scholar] [CrossRef]
- Kim, S.; Kwon, S.A.; Lee, J.E.; Ahn, B.-C.; Lee, J.H.; An, C.; Kitagawa, K.; Kim, D.; Wang, J. Analyzing the role of resource factors in citizens’ intention to pay for and participate in disaster management. Sustainability 2020, 12, 3377. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, D. Does government make people happy? Exploring new research directions for government’s roles in happiness. J. Happiness Stud. 2011, 13, 875–899. [Google Scholar] [CrossRef]
- Kim, S.; Choi, S.-O.; Wang, J. Individual perception vs. structural context: Searching for multilevel determinants of social acceptance of new science and technology across 34 countries. Sci. Public Policy 2013, 5741, 44–57. [Google Scholar] [CrossRef]
- Ryu, Y.; Kim, S. Testing the heuristic/systematic information-processing model (HSM) on the perception of risk after the Fukushima nuclear accidents. J. Risk Res. 2014, 18, 1–20. [Google Scholar] [CrossRef]
- Wang, J.; Kim, S. Comparative analysis of public attitudes toward nuclear power energy across 27 European countries by applying the multilevel model. Sustainability 2018, 10, 1518. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, S. Exploring the determinants of perceived risk of Middle East Respiratory Syndrome (MERS) in Korea. Int. J. Environ. Res. Public Health 2018, 15, 1168. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Kim, S. Searching for new directions for energy policy: Testing the cross-effect of risk perception and cyberspace factors on online/offline opposition to nuclear energy in South Korea. Sustainability 2019, 11, 1368. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Belief Model | Resource Theory | |
|---|---|---|
| Theoretical background | Psychology | Politics, sociology, economics |
| Main variables | Perceived susceptibility/severity, perceived benefits/barriers, efficacy, action cues | Economic wealth/income, education, knowledge, social support/networks |
| Individual behavior | Independent of others | Depends on structural resource constraints |
| Strengths | Highlights the internal psychological structure of decisions | Shows the external and objective determinants of behavior |
| Limits | Disregards the context Provides weak general explanations | Dismisses individual perception and cognition |
| Concept | Measures | Reliability |
|---|---|---|
| 1. Susceptibility | I am more likely to be at risk for COVID-19 than others. I live in an environment where I can be exposed to the COVID-19 infection. | 0.759 |
| 2. Severity | Diseases caused by the COVID-19 infection have very serious consequences. Diseases caused by the COVID-19 infection will have a major impact on my life. | 0.781 |
| 3. Perceived barriers | Excessive efforts are being made to comply with actions for COVID-19 prevention. There are many obstacles to complying with actions for COVID-19 prevention. | 0.503 |
| 4. Perceived benefit | The benefits outweigh the costs of complying with actions for COVID-19 prevention. The benefits outweigh the inconvenience of following actions for COVID-19 prevention. | 0.575 |
| 5. Self-efficacy | If I try, I can fully practice preventive actions. I have enough ability to take actions for COVID-19 prevention. | 0.865 |
| 6. Knowledge | I am familiar with the COVID-19 infection. I know more about COVID-19 than others. | 0.840 |
| 7. Personal health status | I am healthy. I am in good health compared to other people. | 0.901 |
| 8. Social support | I have good relationships with a lot of people. I can get help from others when I’m in trouble. | 0.800 |
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Beta | B | SE | Beta | B | SE | Beta | B | SE | Beta | |||
| Constant | 3.182 | 0.067 | 2.106 | 0.147 | 2.507 | 0.086 | 1.071 | 0.156 | ||||||
| Sociodemographic factors | Gender (female) | 0.197 *** | 0.027 | 0.181 | 0.184 *** | 0.024 | 0.169 | |||||||
| Age | 0.005 *** | 0.001 | 0.125 | 0.004 *** | 0.001 | 0.105 | ||||||||
| Number of elderly people | 0.078 ** | 0.033 | 0.071 | 0.097 *** | 0.03 | 0.088 | ||||||||
| Number of children | 0.057 * | 0.032 | 0.047 | 0.046 | 0.028 | 0.038 | ||||||||
| Residence (rural) | −0.026 | 0.041 | −0.016 | −0.002 | 0.036 | −0.001 | ||||||||
| Ideology (progressive) | 0.049 * | 0.028 | 0.045 | −0.034 | 0.025 | −0.031 | ||||||||
| Health belief factors | Perceived susceptibility | −0.041 ** | 0.017 | −0.062 | −0.038 ** | 0.016 | −0.057 | |||||||
| Perceived severity | 0.104 *** | 0.017 | 0.151 | 0.085 *** | 0.017 | 0.124 | ||||||||
| Perceived barriers | −0.009 | 0.018 | −0.012 | −0.015 | 0.017 | −0.02 | ||||||||
| Perceived benefit | 0.057 *** | 0.019 | 0.075 | 0.032 * | 0.018 | 0.043 | ||||||||
| Self-efficacy of preventive behavior | 0.22 *** | 0.02 | 0.29 | 0.171 *** | 0.019 | 0.225 | ||||||||
| Action cues | Knowing someone who is infected | −0.02 | 0.075 | −0.006 | −0.027 | 0.07 | −0.009 | |||||||
| Family health (poor) | 0.031 * | 0.016 | 0.046 | 0.051 *** | 0.015 | 0.077 | ||||||||
| Media exposure | 0.083 *** | 0.017 | 0.118 | 0.047 *** | 0.016 | 0.066 | ||||||||
| Resource factors | Income | −0.021 | 0.03 | −0.017 | −0.007 | 0.027 | −0.005 | |||||||
| Education | −0.03 | 0.027 | −0.027 | 0.038 | 0.026 | 0.034 | ||||||||
| Knowledge | 0.149 *** | 0.021 | 0.177 | 0.112 *** | 0.02 | 0.133 | ||||||||
| Personal health status | 0.102 *** | 0.017 | 0.15 | 0.089 *** | 0.017 | 0.132 | ||||||||
| Social support | 0.146 *** | 0.021 | 0.184 | 0.094 *** | 0.019 | 0.118 | ||||||||
| F-value | 16.328 *** | 40.710 *** | 44.518 * | 31.639 *** | ||||||||||
| R2/Adjusted R2 | 0.061/0.057 | 0.177/0.173 | 0.128/0.125 | 0.286/0.277 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Kim, S. Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228666
Kim S, Kim S. Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(22):8666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228666
Chicago/Turabian StyleKim, Sunhee, and Seoyong Kim. 2020. "Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 17, no. 22: 8666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228666