
Association between Dietary Pattern, Lifestyle, Anthropometric Status, and Anemia-Related Biomarkers among Adults: A Population-Based Study from 2001 to 2015

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
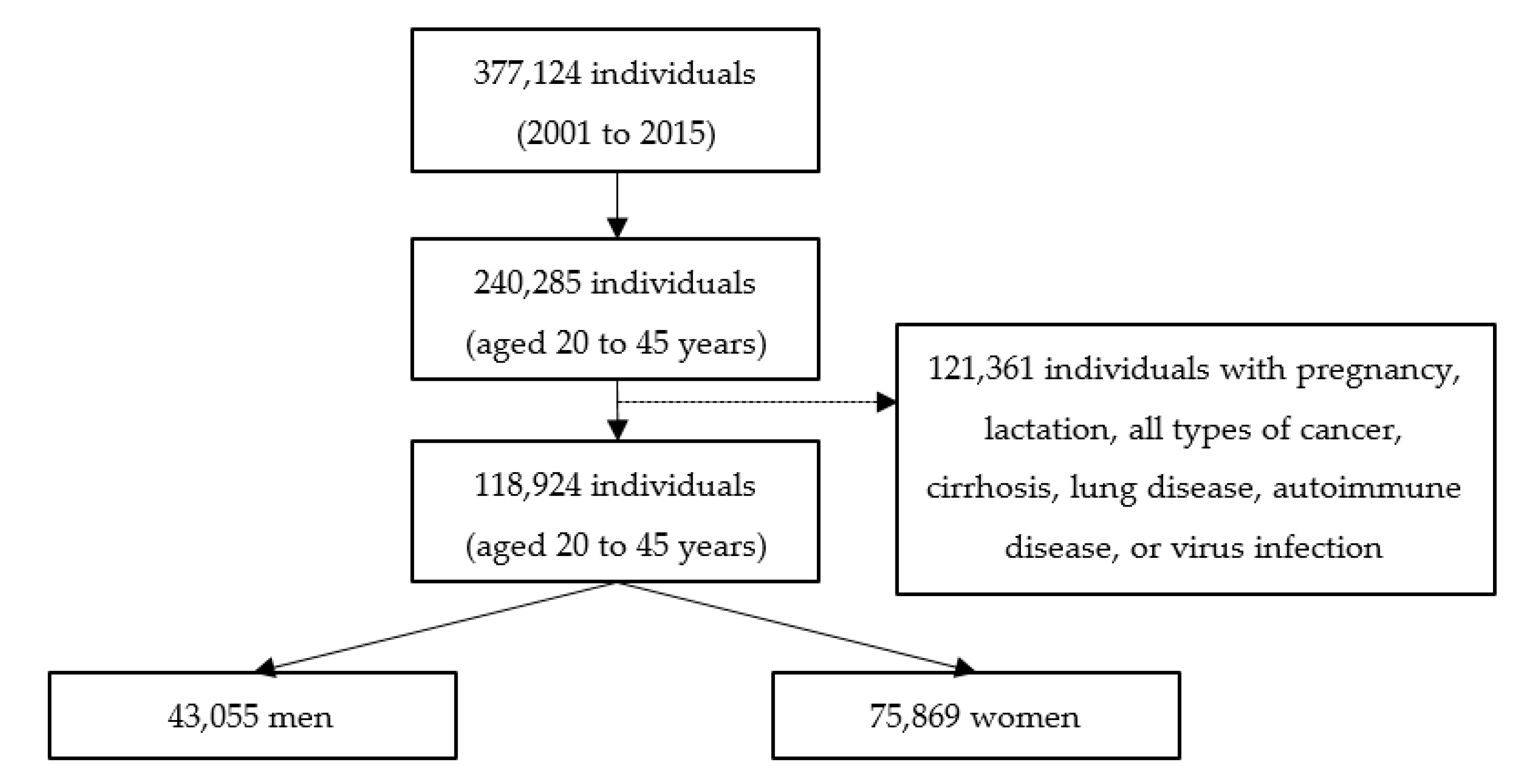
2.1. Data Source and Study Participants
2.2. Anthropometric and Biochemical Data
2.3. Dietary Assessment and Other Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
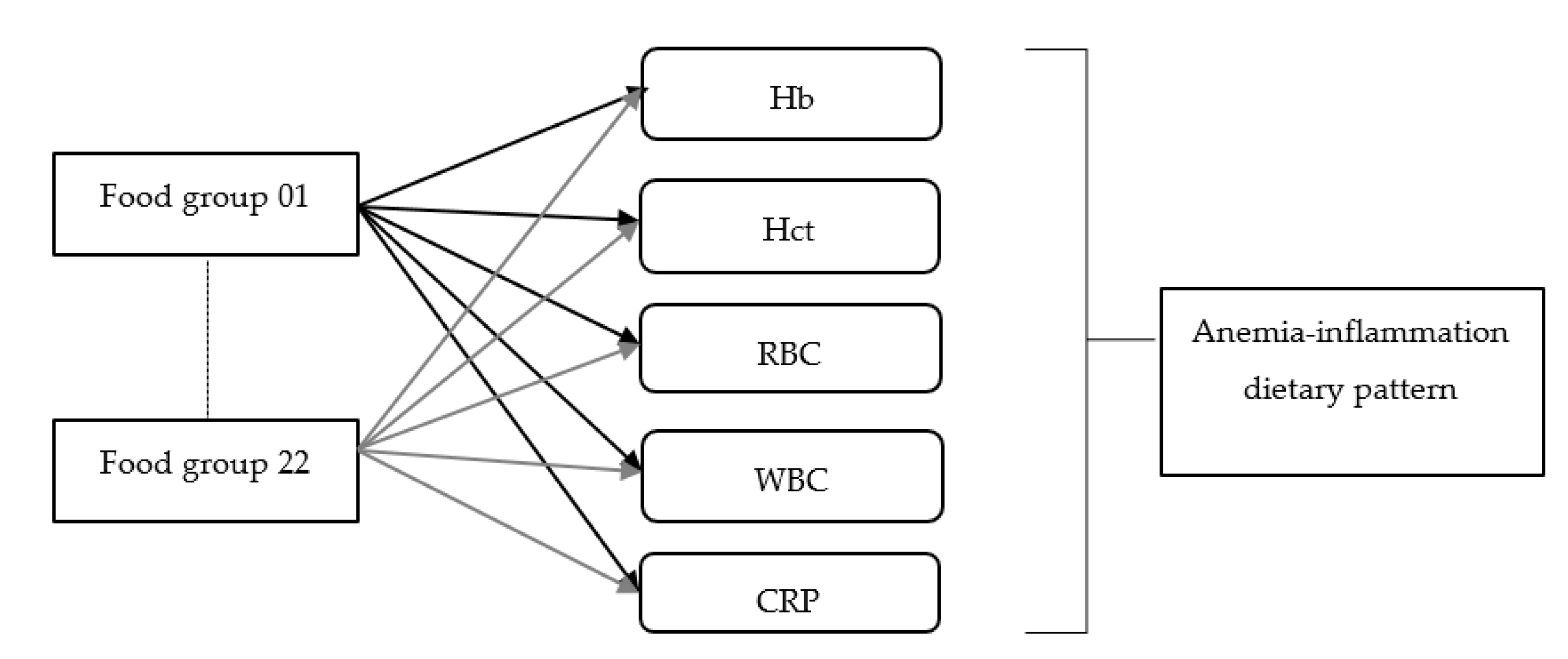
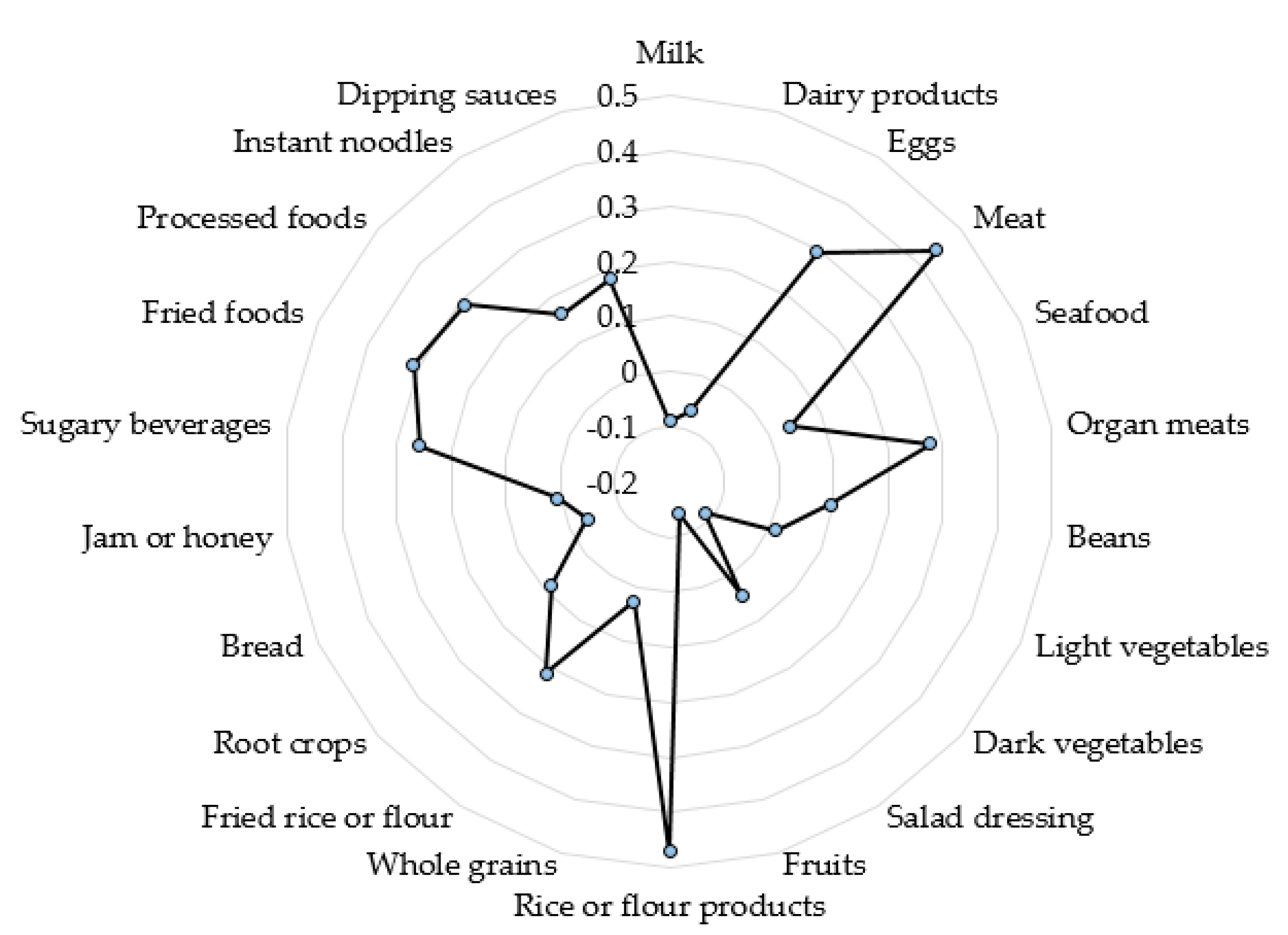
3.2. Anemia-Inflammation Dietary Pattern
3.3. Association of Lifestyle and Anthropometric Data with Anemia
3.4. Association between Lifestyle, Anthropometric Data, and Anemia-Related Biomarkers
3.5. Association between Dietary Pattern, Anemia, and Anemia-Related Biomarkers
4. Discussion
4.1. Lifestyle and Anemia
4.2. Anthropometric Data and Anemia
4.3. Dietary Pattern and Anemia
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, X.; Wu, Z.; Chen, Y.; Zhu, J.; Dong, X.; Fu, C.; Jiang, Q. Increased prevalence and incidence of anemia among adults in transforming rural China: Two cross-sectional surveys. BMC Public Health 2015, 15, 1302. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M.; Nutrition Impact Model Study Group (Anaemia). Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: A systematic analysis of population-representative data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [Green Version]
- Mengesha, M.B.; Dadi, G.B. Prevalence of anemia among adults at Hawassa University referral hospital, Southern Ethiopia. BMC Hematol. 2019, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Le, C.H. The Prevalence of anemia and moderate-severe anemia in the US population (NHANES 2003-2012). PLoS ONE 2016, 11, e0166635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mugisha, J.O.; Baisley, K.; Asiki, G.; Seeley, J.; Kuper, H. Prevalence, types, risk factors and clinical correlates of anaemia in older people in a rural Ugandan population. PLoS ONE 2013, 8, e78394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, W.H.; Wu, H.J.; Yeh, C.J.; Chuang, S.Y.; Chang, H.Y.; Yeh, N.H.; Hsieh, Y.T. Diet and health trends in Taiwan: Comparison of two nutrition and health surveys from 1993–1996 and 2005–2008. Asia Pac. J. Clin. Nutr. 2011, 20, 238–250. [Google Scholar] [PubMed]
- Khan, Z.A.; Khan, T.; Bhardwaj, A.; Aziz, S.J.; Sharma, S. Underweight as a risk factor for nutritional anaemia-a cross-sectional study among undergraduate students of a medical college of Haryana. Indian J. Community Health 2018, 30, 63–69. [Google Scholar]
- Mast, A.E.; Steele, W.R.; Johnson, B.; Wright, D.J.; Cable, R.G.; Carey, P.; Gottschall, J.L.; Kiss, J.E.; Simon, T.L.; Murphy, E.L.; et al. Population-based screening for anemia using first-time blood donors. Am. J. Hematol. 2012, 87, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Shin, C.; Baik, I. Associations between lifestyle factors and iron overload in Korean adults. Clin. Nutr. Res. 2016, 5, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Jackowska, M.; Kumari, M.; Steptoe, A. Sleep and biomarkers in the English Longitudinal Study of Ageing: Associations with C-reactive protein, fibrinogen, dehydroepiandrosterone sulfate and hemoglobin. Psychoneuroendocrinology 2013, 38, 1484–1493. [Google Scholar] [CrossRef]
- Liu, X.; Song, Q.; Hu, W.; Han, X.; Gan, J.; Zheng, X.; Wang, X.; Wu, S. Night sleep duration and risk of incident anemia in a Chinese population: A prospective cohort study. Sci. Rep. 2018, 8, 3975. [Google Scholar] [CrossRef]
- Zhang, F.; Tapera, T.M.; Gou, J. Application of a new dietary pattern analysis method in nutritional epidemiology. BMC Med. Res. Methodol. 2018, 18, 119. [Google Scholar] [CrossRef]
- Kurniawan, A.L.; Hsu, C.Y.; Rau, H.H.; Lin, L.Y.; Chao, J.C.J. Inflammatory dietary pattern predicts dyslipidemia and anemia in middle-aged and older Taiwanese adults with declined kidney function: A cross-sectional population study from 2008 to 2010. Nutrients 2019, 11, 2052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary pattern, serum magnesium, ferritin, C-reactive protein and anaemia among older people. Clin. Nutr. 2017, 36, 444–4451. [Google Scholar] [CrossRef] [PubMed]
- Chin, C.C.; Kuo, Y.H.; Yeh, C.Y.; Chen, J.S.; Tang, R.; Changchien, C.R.; Wang, J.Y.; Huang, W.S. Role of body mass index in colon cancer patients in Taiwan. World J. Gastroenterol. 2012, 18, 4191. [Google Scholar] [CrossRef] [PubMed]
- Verma, M.; Rajput, M.; Sahoo, S.S.; Kaur, N.; Rohilla, R. Correlation between the percentage of body fat and surrogate indices of obesity among adult population in rural block of Haryana. J. Family Med. Prim. Care 2016, 5, 154–159. [Google Scholar] [CrossRef] [Green Version]
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; De Benoist, B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009, 12, 444–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyu, L.C.; Lin, C.F.; Chang, F.H.; Chen, H.F.; Lo, C.C.; Ho, H.F. Meal distribution, relative validity and reproducibility of a meal-based food frequency questionnaire in Taiwan. Asia Pac. J. Clin. Nutr. 2007, 16, 766–776. [Google Scholar]
- MJ Group. MJ Health Screening Center Questionnaire QR-121-1 MJ2011.06-1104TW. Available online: https://www.mjlife.com/index.aspx?lang=chi&fn=index (accessed on 3 August 2020).
- Muga, M.A.; Owili, P.O.; Hsu, C.Y.; Rau, H.H.; Chao, J.C.J. Association between dietary patterns and cardiovascular risk factors among middle-aged and elderly adults in Taiwan: A population-based study from 2003 to 2012. PLoS ONE 2016, 11, e0157745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nettleton, J.A.; Steffen, L.M.; Ni, H.; Liu, K.; Jacobs, D.R., Jr. Dietary patterns and risk of incident type 2 diabetes in Multi-Ethnic Study of Atherosclerosis (MESA). Diabetes Care 2008, 31, 1777–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, K.A.; Sijtsma, F.P.; Nettleton, J.A.; Steffen, L.M.; Van Horn, L.; Shikany, J.M.; Gross, M.D.; Mursu, J.; Traber, M.G.; Jacobs, D.R., Jr. Dietary patterns are associated with plasma F2-isoprostanes in an observational cohort study of adults. Free Radic. Biol. Med. 2013, 57, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Kurniawan, A.L.; Hsu, C.-Y.; Lee, H.-A.; Rau, H.-H.; Paramastri, R.; Syauqy, A.; Chao, J.C.J. Comparing two methods for deriving dietary patterns associated with risk of metabolic syndrome among middle-aged and elderly Taiwanese adults with impaired kidney function. BMC Med. Res. Methodol. 2020, 20, 255. [Google Scholar] [CrossRef] [PubMed]
- Batis, C.; Mendez, M.; Gordon-Larsen, P.; Sotres-Alvarez, D.; Adair, L.; Popkin, B. Using both principal component analysis and reduced rank regression to study dietary patterns and diabetes in Chinese adults. Public Health Nutr. 2016, 19, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Hisa, K.; Haruna, M.; Hikita, N.; Sasagawa, E.; Yonezawa, K.; Suto, M.; Ota, E. Prevalence of and factors related to anemia among Japanese adult women: Secondary data analysis using health check-up database. Sci. Rep. 2019, 9, 17048. [Google Scholar] [CrossRef]
- Sandhya, M.; Satyanarayana, U.; Mohanty, S.; Basalingappa, D.R. Impact of chronic cigarette smoking on platelet aggregation and coagulation profile in apparently healthy male smokers. Int. J. Clin. Exp. Physiol. 2015, 2, 128–133. [Google Scholar]
- Waseem, S.M.A.; Alvi, A.B. Correlation between anemia and smoking: Study of patients visiting different outpatient departments of Integral Institute of Medical Science and Research, Lucknow. Natl. J. Physiol. Pharm. Pharmacol. 2020, 10, 149–154. [Google Scholar] [CrossRef]
- Nordenberg, D.; Yip, R.; Binkin, N.J. The effect of cigarette smoking on hemoglobin levels and anemia screening. JAMA 1990, 264, 1556–1559. [Google Scholar] [CrossRef]
- Sharma, A.J.; Addo, O.Y.; Mei, Z.; Suchdev, P.S. Reexamination of hemoglobin adjustments to define anemia: Altitude and smoking. Ann. N. Y. Acad. Sci. 2019, 1450, 190–203. [Google Scholar] [CrossRef] [Green Version]
- Pollini, G.; Maugeri, U.; Bernardo, A.; Bianchi, I.; Flak, E.; Jedrychowski, W. Erythrocytes parameters due to aging, smoking, alcohol consumption and occupational activity in a working population of petrochemical industry. The Pavia Study. G. Ital. Med. Lav. 1989, 11, 237–240. [Google Scholar]
- Lewis, G.; Wise, M.P.; Poynton, C.; Godkin, A. A case of persistent anemia and alcohol abuse. Nat. Clin. Pract. Gastroenterol. Hepatol. 2007, 4, 521–526. [Google Scholar] [CrossRef]
- Berad, A.; Chand, V. Study to compare hematological parameters in alcoholic and non-alcoholic individuals. Natl. J. Physiol. Pharm. Pharmacol. 2019, 9, 1176–1179. [Google Scholar] [CrossRef]
- Ballard, H.S. The hematological complications of alcoholism. Alcohol Health Res. World 1997, 21, 42–52. [Google Scholar] [CrossRef] [Green Version]
- Kandasamy, K.; Prasad, A.; Surendran, A.; Sebastian, A.C.; Rajagopal, S.S.; Ramanathan, S. Epidemiological study of prevalence of anemia and associated risk factors in a rural community; a home-based screening. Asian J. Pharm. Clin. Res. 2017, 10, 307–309. [Google Scholar]
- Nishida, T.; Sakakibara, H. Low lymphocyte count in underweight Japanese women. Environ. Health Prev. Med. 2008, 13, 345–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumarmi, S.; Puspitasari, N.; Handajani, R.; Wirjatmadi, B. Underweight as a risk factor for iron depletion and iron-deficient erythropoiesis among young women in rural areas of East Java, Indonesia. Malays. J. Nutr. 2016, 22, 219–232. [Google Scholar]
- González-Domínguez, Á.; Visiedo-García, F.M.; Domínguez-Riscart, J.; González-Domínguez, R.; Mateos, R.M.; Lechuga-Sancho, A.M. Iron metabolism in obesity and metabolic syndrome. Int. J. Mol. Sci. 2020, 21, 5529. [Google Scholar] [CrossRef] [PubMed]
- Fleming, R.E. Iron and inflammation: Cross-talk between pathways regulating hepcidin. Int. J. Mol. Med. 2008, 86, 491–494. [Google Scholar] [CrossRef]
- Ganz, T.; Nemeth, E. Iron imports. IV. Hepcidin and regulation of body iron metabolism. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 290, G199–G203. [Google Scholar] [CrossRef] [Green Version]
- Tussing-Humphreys, L.M.; Liang, H.; Nemeth, E.; Freels, S.; Braunschweig, C.A. Excess adiposity, inflammation, and iron-deficiency in female adolescents. J. Am. Diet. Assoc. 2009, 109, 297–302. [Google Scholar] [CrossRef]
- Paterson, E.N.; Neville, C.E.; Silvestri, G.; Montgomery, S.; Moore, E.; Silvestri, V.; Cardwell, C.R.; MacGillivray, T.J.; Max-well, A.P.; Woodside, J.V.; et al. Dietary patterns and chronic kidney disease: A cross-sectional association in the Irish Nun Eye Study. Sci. Rep. 2018, 8, 6654. [Google Scholar] [CrossRef]
- Zárate-Ortiz, A.G.; Melse-Boonstra, A.; Rodríguez-Ramírez, S.; Hernández-Cordero, S.; Feskens, E.J.M. Dietary patterns and the double burden of malnutrition in Mexican adolescents: Results from ENSANUT-2006. Nutrients 2019, 11, 2753. [Google Scholar] [CrossRef] [Green Version]
- Hayeemad, S.; Pradipasen, M.; Satheannoppakao, W.; Kaseamsub, R. Dietary Pattern and Factors Associated with Anemia among Female Adolescents in Islam Private Schools. In Proceedings of the 2nd International Conference on Humanities and Social Sciences, Prince of Songkla University, Hat Yai, Thailand, 10 April 2010; Available online: http://fs.libarts.psu.ac.th/research/conference/proceedings-2/8pdf/001.pdf (accessed on 3 August 2020).
- Wang, D.; Karvonen-Gutierrez, C.A.; Jackson, E.A.; Elliott, M.R.; Appelhans, B.M.; Barinas-Mitchell, E.; Bielak, L.F.; Huang, M.H.; Baylin, A. Western dietary pattern derived by multiple statistical methods is prospectively associated with subclinical carotid atherosclerosis in midlife women. J. Nutr. 2020, 150, 579–591. [Google Scholar]
- Hasanefendić, B.; Hajrović, A.; Begović, E.; Uzunalić, H. The Ratio of Hematological Parameters and Markers of Inflammation in Patients with Iron Deficiency and Pernicious Anemia. In Proceedings of the International Conference on Medical and Biological Engineering; Springer: Berlin, Germany, 2017; pp. 769–773. [Google Scholar]
- Shi, Z.; Hu, X.; Yuan, B.; Pan, X.; Dai, Y.; Holmboe-Ottesen, G. Association between dietary patterns and anaemia in adults from Jiangsu Province in Eastern China. Br. J. Nutr. 2006, 96, 906–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boccio, J.R.; Iyengar, V. Iron deficiency: Causes, consequences, and strategies to overcome this nutritional problem. Biol. Trace Elem. Res. 2003, 94, 1–32. [Google Scholar] [CrossRef]
- López, M.A.; Martos, F.C. Iron availability: An updated review. Int. J. Food Sci. Nutr. 2004, 55, 597–606. [Google Scholar] [CrossRef]
- Matsunaga, A.; Yamamoto, A.; Mizukami, E. Determination of phytic acid in various foods by indirect photometric ion chromatography. Food Hygiene Safety Sci. 1988, 29, 408–412. [Google Scholar] [CrossRef] [Green Version]
- Kito, A.; Imai, E. The Association with dietary patterns and risk of anemia in Japanese elderly. J. Nutr. Sci. Vitaminol. 2020, 66, 32–40. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | All Subjects (n = 118,924) | Subjects without Anemia (n = 106,023) | Subjects with Anemia (n = 12,901) | p |
|---|---|---|---|---|
| Demographic and lifestyle data | ||||
| Age, years | 33.6 ± 6.5 | 33.4 ± 6.5 | 35.3 ± 6.5 | 0.262 |
| Gender | <0.001 | |||
| Men | 43,055 (36.2%) | 42,543 (98.8%) b | 512 (1.2%) b | |
| Women | 75,869 (63.8%) | 63,480 (83.7%) b | 12,389 (16.3%) b | |
| Smoking | <0.001 | |||
| Non-smoker | 95,733 (80.5%) | 83,842 (79.1%) | 11,891 (92.2%) | |
| Past smoker | 4617 (3.9%) | 4352 (4.1%) | 265 (2.1%) | |
| Current smoker | 18,574 (15.6%) | 17,829 (16.8%) | 745 (5.7%) | |
| Drinking alcohol | <0.001 | |||
| No | 106,721 (89.7%) | 94,461 (89.1%) | 12,260 (95.0%) | |
| Yes | 12,203 (10.3%) | 11,562 (10.9%) | 641 (5.0%) | |
| Chewing betel nut | <0.001 | |||
| No | 118,657 (99.8%) | 105,761 (99.8%) | 12,896 (99.9%) | |
| Yes | 267 (0.2%) | 262 (0.2%) | 5 (0.1%) | |
| Sleep duration | <0.001 | |||
| <6 h | 98,970 (83.2%) | 88,358 (83.3%) | 10,612 (82.3%) | |
| 6–8 h | 19,554 (16.4%) | 17,318 (16.3%) | 2236 (17.3%) | |
| >8 h | 400 (0.4%) | 347 (0.4%) | 53 (0.4%) | |
| Physical activity | <0.001 | |||
| ≤2 h/week | 101,809 (85.6%) | 90,347 (85.2%) | 11,462 (88.8%) | |
| >2 h/week | 17,115 (14.4%) | 15,676 (14.8%) | 1439 (11.2%) | |
| Prevalence of chronic diseases | ||||
| Hypertension | 5446 (4.6%) | 5058 (4.8%) | 388 (3.0%) | <0.001 |
| Diabetes | 1538 (1.3%) | 1378 (1.3%) | 160 (1.2%) | 0.258 |
| Anthropometric measurements | ||||
| Body mass index, kg/m2 c | <0.001 | |||
| Underweight | 14,333 (12.1%) | 12,414 (11.7%) | 1919 (14.9%) | |
| Normal | 72,838 (61.3%) | 63,965 (60.3%) | 8873 (68.8%) | |
| Overweight | 20,348 (17.1%) | 18,902 (17.8%) | 1446 (11.2%) | |
| Obese | 11,405 (9.5%) | 10,742 (10.2%) | 663 (5.1%) | |
| Central obesity d | 12,981 (10.9%) | 12,048 (11.4%) | 933 (0.9%) | <0.001 |
| Anemia or inflammatory biomarkers | ||||
| Hemoglobin, mmol/L | 8.6 ± 1.1 | 8.8 ± 0.8 | 6.8 ± 0.7 | <0.001 |
| Hematocrit, % | 41.1 ± 4.6 | 41.9 ± 3.8 | 33.7 ± 2.9 | <0.001 |
| Red blood cells, 106/μL | 4.7 ± 0.5 | 4.7 ± 0.5 | 4.5 ± 0.6 | <0.001 |
| White blood cells, 103/μL | 6.0 ± 1.7 | 5.6 ± 2.2 | 6.1 ± 1.6 | <0.001 |
| C-reactive protein, nmol/L | 18.8 ± 34.7 | 18.7 ± 40.5 | 18.9 ± 33.9 | 0.130 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Lifestyle | ||||
| Smoking (ref: non-smoker) | ||||
| Past smoker | 0.29 (0.27, 0.32) | 0.001 | 0.68 (0.63, 0.74) | 0.001 |
| Current smoker | 0.43 (0.38, 0.49) | 0.001 | 0.74 (0.64, 0.86) | 0.001 |
| Drinking alcohol (ref: no drinking) | 2.55 (2.31, 2.81) | 0.001 | 1.46 (1.32, 1.61) | 0.001 |
| Sleep duration (ref: 6–8 h) | ||||
| Short sleep duration (<6 h) | 1.22 (0.91, 1.62) | 0.188 | 1.12 (0.83, 1.50) | 0.695 |
| Long sleep duration (>8 h) | 1.04 (0.98, 1.19) | 0.140 | 1.01 (0.96, 1.07) | 0.468 |
| Inactive physical activity b (ref: >2 h/week) | 1.38 (1.31, 1.46) | 0.001 | 0.97 (0.89, 1.05) | 0.433 |
| Anthropometric measurements | ||||
| Body mass index c (ref: normal) | ||||
| Underweight | 2.58 (2.33, 2.88) | 0.001 | 1.20 (1.10, 1.42) | 0.001 |
| Overweight | 1.24 (1.11, 1.38) | 0.001 | 1.23 (1.10, 1.38) | 0.001 |
| Obese | 2.27 (2.07, 2.49) | 0.001 | 1.34 (1.22, 1.48) | 0.001 |
| Central obesity d (ref: normal) | 1.64 (1.51, 1.77) | 0.001 | 1.28 (1.18, 1.39) | 0.001 |
| Hb (mmol/L) β (95% CI) | Hct (%) β (95% CI) | RBC (106/μL) β (95% CI) | WBC (103/μL) β (95% CI) | CRP (nmol/L) β (95% CI) | |
|---|---|---|---|---|---|
| Lifestyle | |||||
| Smoking (ref: non-smoker) | |||||
| Past smoker | 0.18 (0.17, 0.19) * | 0.09 (−0.10, 0.20) | −0.00 (−0.02, 0.01) | 0.13 (0.07, 0.19) ** | −0.29 (−1.51, 0.91) |
| Current smoker | 0.29 (0.28, 0.32) ** | 0.74 (0.68, 0.80) ** | 0.00 (−0.01, 0.01) | 0.68 (0.65, 0.71) ** | 1.21 (0.52, 1.89) ** |
| Drinking alcohol (ref: no drinking) | −0.08 (−0.09, −0.06) ** | 0.06 (−0.01, 0.13) | −0.05 (−0.05, −0.04) ** | −0.02 (−0.06, 0.02) | 0.35 (−0.42, 1.13) |
| Sleep duration (ref: 6–8 h) | |||||
| Short sleep duration (<6 h) | −0.02 (−0.03, −0.01) * | −0.03 (−0.08, 0.02) | 0.00 (−0.03, 0.04) | 0.28 (0.03, 0.53) * | 2.31 (−3.15, 7.77) |
| Long sleep duration (>8 h) | −0.03 (−0.10, 0.04) | −0.03 (−0.33, 0.27) | 0.00 (−0.00, 0.01) | 0.02 (−0.05, 0.01) | −0.24 (−0.92, 0.43) |
| Inactive physical activity b (ref: >2 h/week) | −0.01 (−0.02, −0.01) ** | −0.33 (−0.39, −0.26) ** | −0.03 (−0.03, −0.02) ** | 0.14 (0.11, 0.17) * | 1.17 (0.55, 1.79) * |
| Anthropometric measurements | |||||
| Body mass index c (ref: normal) | |||||
| Underweight | −0.02 (−0.03, 0.01) | −0.22 (−0.91, 0.72) | −0.22 (−0.20, −0.23) ** | −0.25 (−0.28, −0.22) ** | 0.77 (−0.14, 1.59) |
| Overweight | −0.05 (−0.07, −0.03) ** | −0.45 (−0.53, −0.37) ** | −0.02 (−0.03, −0.01) ** | 0.42 (0.38, 0.45) ** | 3.52 (2.86, 4.18) ** |
| Obese | −0.13 (−0.15, −0.11) ** | −0.86 (−0.93, −0.78) ** | −0.09 (−0.10, −0.08) ** | 0.73 (0.68, 0.78) ** | 9.58 (8.43, 10.70) ** |
| Central obesity d (ref: normal) | −0.14 (−0.15, −0.12) ** | −0.78 (−0.84, −0.71) ** | −0.06 (−0.07, −0.05) ** | 0.35 (0.31, 0.39) ** | 9.60 (8.67, 10.53) ** |
| Anemia OR (95% CI) | Anemia-Related Biomarkers | |||||
|---|---|---|---|---|---|---|
| Hb (mmol/L) β (95% CI) | Hct (%) β (95% CI) | RBC (106/μL) β (95% CI) | WBC (103/μL) β (95% CI) | CRP (nmol/L) β (95% CI) | ||
| Model 1 (ref: T1) | ||||||
| T2 | 1.43 (1.36, 1.50) ** | −0.26 (−0.28, −0.24) ** | −1.19 (−1.26, −1.13) ** | −0.12 (−0.13, −0.12) ** | 0.19 (0.17, 0.22) ** | 0.09 (0.09, 1.2) ** |
| T3 | 1.87 (1.78, 1.95) ** | −0.48 (−0.49, −0.46) ** | −2.21 (−2.27, −2.15) ** | −0.23 (−0.24, −0.23) ** | 0.34 (0.29, 0.41) ** | 1.90 (1.59, 2.60) ** |
| Model 2 (ref: T1) | ||||||
| T2 | 1.09 (1.01, 1.10) ** | −0.11 (−0.12, −0.10) ** | −0.12 (−0.13, −0.09) ** | −0.00 (−0.01, −0.00) ** | 0.12 (0.00, 0.12) ** | 0.38 (−0.11, 1.03) |
| T3 | 1.10 (1.00, 1.23) ** | −0.24 (−0.26, −0.24) ** | −0.24 (−0.24, −0.09) ** | −0.03 (−0.03, −0.02) ** | 0.17 (0.17, 0.21) ** | 1.70 (1.12, 2.37) ** |
| Model 3 (ref: T1) | ||||||
| T2 | 1.30 (1.27, 1.41) ** | −0.01 (−0.02, −0.00) ** | −0.01 (−0.10, −0.01) ** | −0.01 (−0.01, −0.00) ** | 0.04 (0.01, 0.07) ** | 0.64 (0.19, 0.89) ** |
| T3 | 1.59 (1.51, 1.67) ** | −0.03 (−0.04, −0.02) ** | −0.04 (−0.01, −0.09) ** | −0.02 (−0.03, −0.02) ** | 0.08 (0.05, 0.10) ** | 1.64 (0.50, 2.21) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paramastri, R.; Hsu, C.-Y.; Lee, H.-A.; Lin, L.-Y.; Kurniawan, A.L.; Chao, J.C.-J. Association between Dietary Pattern, Lifestyle, Anthropometric Status, and Anemia-Related Biomarkers among Adults: A Population-Based Study from 2001 to 2015. Int. J. Environ. Res. Public Health 2021, 18, 3438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073438
Paramastri R, Hsu C-Y, Lee H-A, Lin L-Y, Kurniawan AL, Chao JC-J. Association between Dietary Pattern, Lifestyle, Anthropometric Status, and Anemia-Related Biomarkers among Adults: A Population-Based Study from 2001 to 2015. International Journal of Environmental Research and Public Health. 2021; 18(7):3438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073438
Chicago/Turabian StyleParamastri, Rathi, Chien-Yeh Hsu, Hsiu-An Lee, Li-Yin Lin, Adi Lukas Kurniawan, and Jane C.-J. Chao. 2021. "Association between Dietary Pattern, Lifestyle, Anthropometric Status, and Anemia-Related Biomarkers among Adults: A Population-Based Study from 2001 to 2015" International Journal of Environmental Research and Public Health 18, no. 7: 3438. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073438