
Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
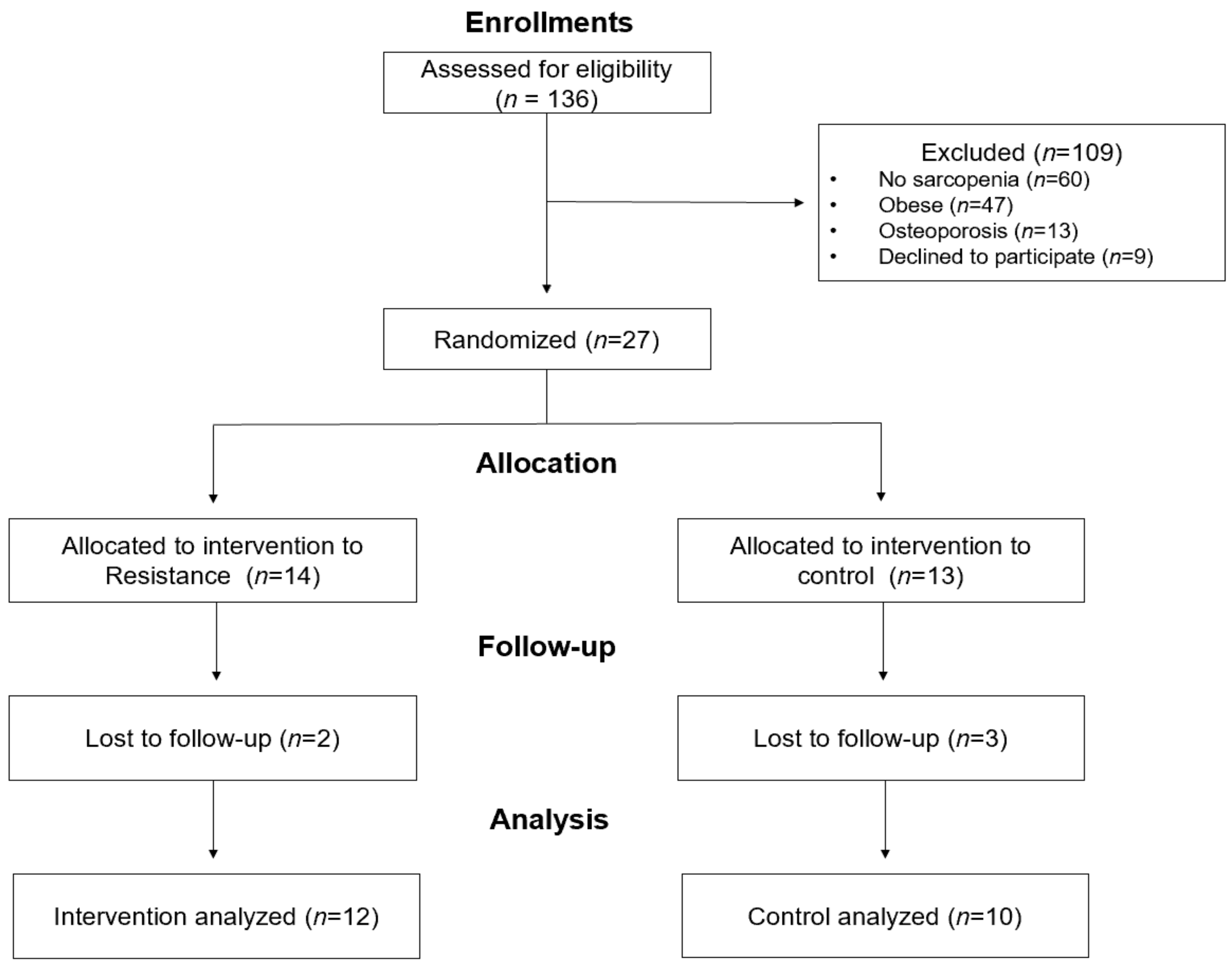
2.1. Participants
2.2. Anthropometric Measurements
2.3. Body Composition
2.4. Functional Fitness
2.5. Mid-Thigh Composition
2.6. Maximal Isometric Muscle Strength
2.7. Biochemical Markers
2.8. Intervention
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodds, R.M.; Roberts, H.C.; Cooper, C.; Sayer, A.A. The Epidemiology of Sarcopenia. J. Clin. Densitom. 2015, 18, 461–466. [Google Scholar] [CrossRef] [Green Version]
- Yeung, S.S.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexi Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S. Gender differences in physical activity and walking among older adults. J. Women Aging 2005, 17, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Mackenzie, T.A.; Barre, L.K.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity and mortality in older adults: Results from the National Health and Nutrition Examination Survey III. Eur. J. Clin. Nutr. 2014, 68, 1001–1007. [Google Scholar] [CrossRef] [Green Version]
- Drescher, C.; Konishi, M.; Ebner, N.; Springer, J. Loss of muscle mass: Current developments in cachexia and sarcopenia focused on biomarkers and treatment. J. Cachexi Sarcopenia Muscle 2015, 6, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Payette, H.; Roubenoff, R.; Jacques, P.F.; Dinarello, C.A.; Wilson, P.W.; Abad, L.W.; Harris, T. Insulin-like growth factor-1 and interleukin 6 predict sarcopenia in very old community-living men and women: The Framingham Heart Study. J. Am. Geriatr. Soc. 2003, 51, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; James, R.S.; Cox, V.M.; Seebacher, F.; Tallis, J. Age-related changes in isolated mouse skeletal muscle function are dependent on sex, muscle, and contractility mode. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2020, 319, R296–R314. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Adamek, M.; Gonzalez, M.C.; Jia, G.; Thomas, D.M. Assessing skeletal muscle mass: Historical overview and state of the art. J. Cachexi Sarcopenia Muscle 2014, 5, 9–18. [Google Scholar] [CrossRef]
- Seo, M.W.; Jung, S.W.; Kim, S.W. Comparisons of Muscle Quality and Muscle Growth Factor between Sarcopenic and Non-Sarcopenic Older Women. Int. J. Environ. Res. Public Health 2020, 17, 6581. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Vitale, J.; Sconfienza, L.M. Imaging of sarcopenia: Old evidence and new insights. Eur. Radiol. 2020, 30, 2199–2208. [Google Scholar] [CrossRef]
- Parker, L.; Caldow, M.K.; Watts, R.; Levinger, P.; Cameron-Smith, D.; Levinger, I. Age and sex differences in human skeletal muscle fibrosis markers and transforming growth factor-β signaling. Eur. J. Appl. Physiol. 2017, 117, 1463–1472. [Google Scholar] [CrossRef]
- Ismaeel, A.; Kim, J.-S.; Kirk, J.S.; Smith, R.S.; Bohannon, W.T.; Koutakis, P. Role of Transforming Growth Factor-β in Skeletal Muscle Fibrosis: A Review. Int. J. Mol. Sci. 2019, 20, 2446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latres, E.; Mastaitis, J. Activin A more prominently regulates muscle mass in primates than does GDF8. Nat. Commun. 2017, 8, 15153. [Google Scholar] [CrossRef] [Green Version]
- Han, X.; Møller, L.L.V. Mechanisms involved in follistatin-induced hypertrophy and increased insulin action in skeletal muscle. J. Cachexia Sarcopenia Muscle 2019, 10, 1241–1257. [Google Scholar] [CrossRef] [Green Version]
- Calvani, R.; Marini, F.; Cesari, M.; Tosato, M.; Anker, S.D.; von Haehling, S.; Miller, R.R.; Bernabei, R.; Landi, F.; Marzetti, E.; et al. Biomarkers for physical frailty and sarcopenia: State of the science and future developments. J. Cachexi Sarcopenia Muscle 2015, 6, 278–286. [Google Scholar] [CrossRef]
- Ebner, N.; Steinbeck, L.; Doehner, W.; Anker, S.D.; von Haehling, S. Highlights from the 7th Cachexia Conference: Muscle wasting pathophysiological detection and novel treatment strategies. J. Cachexi Sarcopenia Muscle 2014, 5, 27–34. [Google Scholar] [CrossRef]
- Mafi, F.; Biglari, S.; Ghardashi Afousi, A.; Gaeini, A.A. Improvement in Skeletal Muscle Strength and Plasma Levels of Follistatin and Myostatin Induced by an 8-Week Resistance Training and Epicatechin Supplementation in Sarcopenic Older Adults. J. Aging Phys. Act. 2019, 27, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef]
- Krause, M.; Crognale, D.; Cogan, K.; Contarelli, S.; Egan, B.; Newsholme, P.; De Vito, G. The effects of a combined bodyweight-based and elastic bands resistance training, with or without protein supplementation, on muscle mass, signaling and heat shock response in healthy older people. Exp. Gerontol. 2019, 115, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Vikberg, S.; Sörlén, N.; Brandén, L.; Johansson, J.; Nordström, A.; Hult, A.; Nordström, P. Effects of Resistance Training on Functional Strength and Muscle Mass in 70-Year-Old Individuals With Pre-sarcopenia: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2019, 20, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, Y.; Tanimoto, M.; Oba, N.; Sanada, K.; Miyachi, M.; Ishii, N. Effect of resistance training using bodyweight in the elderly: Comparison of resistance exercise movement between slow and normal speed movement. Geriatr. Gerontol. Int. 2015, 15, 1270–1277. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Huang, S.W.; Ku, J.W.; Hsiao, D.J.; Liou, T.H. Effects of elastic band exercise on lean mass and physical capacity in older women with sarcopenic obesity: A randomized controlled trial. Sci. Rep. 2018, 8, 2317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Song, M.; Cho, B.L.; Lim, J.Y.; Song, W.; Kim, S.H. The effects of an integrated health education and exercise program in community-dwelling older adults with hypertension: A randomized controlled trial. Patient Educ. Couns. 2011, 82, 133–137. [Google Scholar] [CrossRef]
- Colado, J.C.; Garcia-Masso, X.; Triplett, T.N.; Flandez, J.; Borreani, S.; Tella, V. Concurrent validation of the OMNI-resistance exercise scale of perceived exertion with Thera-band resistance bands. J. Strength Cond. Res. 2012, 26, 3018–3024. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuku, S.; Kajioka, T.; Endo, H.; Abbott, R.D.; Curb, J.D.; Yano, K. Favorable effects of non-instrumental resistance training on fat distribution and metabolic profiles in healthy elderly people. Eur. J. Appl. Physiol. 2007, 99, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Martone, A.M.; Marzetti, E.; Calvani, R.; Picca, A.; Tosato, M.; Santoro, L.; Di Giorgio, A.; Nesci, A.; Sisto, A.; Santoliquido, A.; et al. Exercise and Protein Intake: A Synergistic Approach against Sarcopenia. Biomed. Res. Int. 2017, 2017, 2672435. [Google Scholar] [CrossRef]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Jacob, K.J.; Chevalier, S.; Lamarche, M.; Morais, J.A. Leucine Supplementation Does Not Alter Insulin Sensitivity in Prefrail and Frail Older Women following a Resistance Training Protocol. J. Nutr. 2019, 149, 959–967. [Google Scholar] [CrossRef]
- Maltais, M.L.; Ladouceur, J.P.; Dionne, I.J. The Effect of Resistance Training and Different Sources of Postexercise Protein Supplementation on Muscle Mass and Physical Capacity in Sarcopenic Elderly Men. J. Strength Cond. Res. 2016, 30, 1680–1687. [Google Scholar] [CrossRef] [PubMed]
- Strandberg, E.; Edholm, P.; Ponsot, E.; Wåhlin-Larsson, B.; Hellmén, E.; Nilsson, A.; Engfeldt, P.; Cederholm, T.; Risérus, U.; Kadi, F. Influence of combined resistance training and healthy diet on muscle mass in healthy elderly women: A randomized controlled trial. J. Appl. Physiol. 2015, 119, 918–925. [Google Scholar] [CrossRef] [Green Version]
- Beavers, K.M.; Beavers, D.P.; Martin, S.B.; Marsh, A.P.; Lyles, M.F.; Lenchik, L.; Shapses, S.A.; Nicklas, B.J. Change in Bone Mineral Density During Weight Loss with Resistance Versus Aerobic Exercise Training in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1582–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez-Campillo, R.; Castillo, A.; de la Fuente, C.I.; Campos-Jara, C.; Andrade, D.C.; Álvarez, C.; Martínez, C.; Castro-Sepúlveda, M.; Pereira, A.; Marques, M.C.; et al. High-speed resistance training is more effective than low-speed resistance training to increase functional capacity and muscle performance in older women. Exp. Gerontol. 2014, 58, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Martins, W.R.; Safons, M.P.; Bottaro, M.; Blasczyk, J.C.; Diniz, L.R.; Fonseca, R.M.; Bonini-Rocha, A.C.; de Oliveira, R.J. Effects of short term elastic resistance training on muscle mass and strength in untrained older adults: A randomized clinical trial. BMC Geriatr. 2015, 15, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Addison, O.; Marcus, R.L.; Lastayo, P.C.; Ryan, A.S. Intermuscular fat: A review of the consequences and causes. Int. J. Endocrinol. 2014, 2014, 309570. [Google Scholar] [CrossRef] [Green Version]
- Reding, K.W.; Brubaker, P.; D’Agostino, R., Jr.; Kitzman, D.W.; Nicklas, B.; Langford, D.; Grodesky, M.; Hundley, W.G. Increased skeletal intermuscular fat is associated with reduced exercise capacity in cancer survivors: A cross-sectional study. Cardiooncology 2019, 5, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, M.; Schober-Halper, B.; Oesen, S.; Franzke, B.; Tschan, H.; Bachl, N.; Strasser, E.M.; Quittan, M.; Wagner, K.H.; Wessner, B. Effects of elastic band resistance training and nutritional supplementation on muscle quality and circulating muscle growth and degradation factors of institutionalized elderly women: The Vienna Active Ageing Study (VAAS). Eur. J. Appl. Physiol. 2016, 116, 885–897. [Google Scholar] [CrossRef] [Green Version]
- Hanna, A.; Frangogiannis, N.G. The Role of the TGF-β Superfamily in Myocardial Infarction. Front. Cardiovasc. Med. 2019, 6, 140. [Google Scholar] [CrossRef]


{kind=link}
| Variables | RT (n = 12) | CON (n = 10) | p-Value |
|---|---|---|---|
| Age (yrs) | 70.3 ± 5.38 | 72.9 ± 4.75 | 0.239 |
| Body height (cm) | 152.9 ± 4.92 | 151.4 ± 5.45 | 0.505 |
| Body weight (kg) | 53.4 ± 4.39 | 51.5 ± 5.64 | 0.396 |
| BMI (kg·m−2) | 22.9 ± 2.02 | 22.4 ± 1.52 | 0.579 |
| Waist circumference (cm) | 76.2 ± 5.18 | 77.4 ± 4.56 | 0.564 |
| Hip circumference (cm) | 89.6 ± 4.38 | 90.6 ± 4.27 | 0.598 |
| WHR | 0.85 ± 0.04 | 0.85 ± 0.03 | 0.804 |
| Exercise Program | Type | Part | Contents |
|---|---|---|---|
| (Time) | |||
| Warm-Up | Stretching (5 min) | Whole-Body | Stretching, Walking |
| Main exercise | Resistance (50 min) | Upper body | Shoulder press, Front raise, Lateral raise, Biceps curl, Triceps extension, Kick back, Crunch, Bent over row, Seated row, Back extension (prone), Push up (beginner) |
| Lower body | Squat, Lunge, Lying leg abduction, Leg kick back, Pelvic lift, Leg raise, Toe & Heel raise | ||
| Cool-down | Stretching (5 min) | Whole-body | Static stretching |
| Exercise | Phase (weeks) | Repetitions | Sets | Intensity |
|---|---|---|---|---|
| (OMNI Scale/Color) | ||||
| Resistance training | 1 | 6 | 3 | 4/Yellow |
| 2 | 8 | 3 | 4/Yellow | |
| 3 | 10 | 3 | 5/Yellow | |
| 4 | 12 | 3 | 5/Yellow | |
| 5 | 10 | 4 | 6/Yellow | |
| 6 | 10 | 4 | 6/Yellow | |
| 7 | 12 | 5 | 6/Yellow | |
| 8 | 12 | 5 | 6/Yellow | |
| 9 | 15 | 3 | 7/Yellow | |
| 10 | 15 | 3 | 7/Yellow | |
| 11 | 15 | 3 | 7/Yellow | |
| 12 | 15 | 3 | 7/Yellow | |
| 13 | 15 | 4 | 8/Yellow | |
| 14 | 15 | 4 | 8/Yellow | |
| 15 | 15 | 5 | 8/Yellow | |
| 16 | 15 | 5 | 8/Yellow |
| Variables | Group | Baseline | Post | d | Univariate Interaction (η2p) | Manova Interaction (η2p) |
|---|---|---|---|---|---|---|
| Body weight (kg) | RT | 53.4 ± 4.39 | 53.3 ± 4.39 | 0.07 | 0.072 (0.004) | 1.392 (0.247) |
| CG | 51.5 ± 5.64 | 51.3 ± 5.95 | 0.15 | |||
| BMI (kg·m−2) | RT | 22.9 ± 2.02 | 22.9 ± 2.02 | 0.01 | 0.019 (0.001) | |
| CG | 22.4 ± 1.52 | 22.4 ± 1.58 | 0.04 | |||
| Waist circumference (cm) | RT | 76.2 ± 5.18 | 76.1 ± 4.18 | 0.04 | 2.068 (0.094) | |
| CG | 77.4 ± 4.56 | 78.4 ± 5.60 | 0.71 | |||
| Hip circumference (cm) | RT | 89.6 ± 4.38 | 89.9 ± 3.68 | 0.17 | 1.593 (0.074) | |
| CG | 90.6 ± 4.27 | 90.1 ± 4.00 | 0.42 | |||
| WHR | RT | 0.85 ± 0.04 | 0.85 ± 0.04 | 0.19 | 7.188 * (0.264) | |
| CG | 0.85 ± 0.03 | 0.87 ± 0.04 ++ | 1.04 | |||
| Fat mass (kg) | RT | 19.1 ± 3.11 | 19.2 ± 3.21 | 0.12 | 0.288 (0.014) | 0.397 (0.062) |
| CG | 17.5 ± 3.58 | 17.4 ± 3.77 | 0.11 | |||
| Fat-free mass (kg) | RT | 31.6 ± 2.10 | 31.9 ± 1.87 | 0.46 | 1.414 (0.066) | |
| CG | 31.5 ± 2.58 | 31.5 ± 2.87 | 0.10 | |||
| ASM (kg) | RT | 12.3 ± 0.96 | 12.4 ± 0.77 | 0.25 | 2.645 (0.117) | |
| CG | 12.4 ± 0.95 | 12.2 ± 1.10 | 0.43 | |||
| Percent body fat (%) | RT | 36.3 ± 3.74 | 36.3 ± 3.82 | 0.02 | 0.028 (0.001) | |
| CG | 34.4 ± 3.85 | 34.3 ± 4.14 | 0.08 | |||
| Whole-body BMC (g) | RT | 1574.36 ± 193.79 | 1566.75 ± 189.47 | 0.35 | 0.421 (0.021) | 1.083 (0.253) |
| CG | 1460.46 ± 210.27 | 1446.86 ± 206.42 | 0.63 | |||
| Whole body BMD (g·cm−2) | RT | 0.951 ± 0.071 | 0.949 ± 0.071 | 0.11 | 0.108 (0.005) | |
| CG | 0.915 ± 0.058 | 0.916 ± 0.061 | 0.03 | |||
| Lumbar BMC (g) | RT | 47.71 ± 9.15 | 47.48 ± 9.47 | 0.14 | 1.965 (0.089) | |
| CG | 41.50 ± 8.46 | 40.46 ± 7.88 | 0.09 | |||
| Lumbar BMD (g·cm−2) | RT | 0.834 ± 0.110 | 0.833 ± 0.121 | 0.04 | 0.589 (0.029) | |
| CG | 0.761 ± 0.102 | 0.755 ± 0.097 | 0.40 | |||
| Femur BMC (g) | RT | 23.01 ± 3.53 | 22.97 ± 3.03 | 0.03 | 0.031 (0.002) | |
| CG | 20.09 ± 3.73 | 19.98 ± 3.53 | 0.15 | |||
| Femur BMD (g·cm−2) | RT | 0.729 ± 0.090 | 0.734 ± 0.085 | 0.26 | 0.168 (0.008) | |
| CG | 0.650 ± 0.105 | 0.652 ± 0.104 | 0.31 |
| Variables | Group | Baseline | Post | d | Univariate Interaction (η2p) | Manova Interaction (η2p) |
|---|---|---|---|---|---|---|
| 30-s chair stand (n) | RT | 15.5 ± 4.50 | 20.3 ± 5.16 +++ | 1.69 | 20.608 *** (0.507) | 10.880 *** (0.813) |
| CG | 12.1 ± 3.07 | 12.1 ± 3.14 | 0.00 | |||
| 30-s arm curl (n) | RT | 16.3 ± 3.68 | 21.2 ± 3.69 +++ | 2.48 | 45.996 *** (0.697) | |
| CG | 13.9 ± 3.25 | 13.1 ± 2.60 | 0.41 | |||
| Chair sit-and-reach (cm) | RT | 19.8 ± 7.15 | 24.3 ± 6.94 ++ | 1.39 | 37.101 *** (0.650) | |
| CG | 6.2 ± 10.56 | 3.5 ± 10.08 ++ | 1.33 | |||
| 8-foot up-and-go (s) | RT | 5.7 ± 0.45 | 5.1 ± 0.45 +++ | 1.77 | 29.831 *** (0.599) | |
| CG | 5.9 ± 0.65 | 6.3 ± 0.77 + | 0.79 | |||
| 2-min step test (n) | RT | 91.3 ± 11.01 | 108.3 ± 11.04 ++ | 1.20 | 22.453 *** (0.529) | |
| CG | 86.7 ± 12.96 | 75.1 ± 18.92 + | 0.83 | |||
| Grip strength (kg) | RT | 20.8 ± 2.93 | 24.3 ± 2.25 +++ | 1.72 | 41.123 *** (0.673) | |
| CG | 18.6 ± 3.07 | 17.3 ± 3.61 + | 0.99 | |||
| Gait speed (m·s−1) | RT | 0.96 ± 0.08 | 1.14 ± 0.11 +++ | 1.84 | 23.635 *** (0.542) | |
| CG | 0.93 ± 0.09 | 0.95 ± 0.09 | 0.43 |
| Variables | Variables | Group | Baseline | Post | d | Univariate Interaction (η2p) | Manova Interaction (η2p) |
|---|---|---|---|---|---|---|---|
| Mid-Thigh Muscle Quality | MVIC (N·m) | RT | 112.4 ± 21.60 | 123.5 ± 18.87 + | 1.09 | 7.417 (0.271) | |
| CG | 97.6 ± 30.94 | 93.7 ± 25.47 | 0.25 | ||||
| RMVIC (N·m·kg−1) | RT | 209.9 ± 32.18 | 231.8 ± 30.25 + | 1.20 | 7.560 (0.274) | ||
| CG | 195.4 ± 76.53 | 186.6 ± 61.29 | 0.26 | ||||
| TTV (cm2) | RT | 142.3 ± 17.60 | 142.5 ± 19.28 | 0.02 | 0.168 (0.008) | ||
| CG | 138.5 ± 20.12 | 140.2 ± 15.56 | 0.25 | ||||
| TFV (cm2) | RT | 62.9 ± 15.43 | 61.7 ± 15.97 | 0.19 | 2.965 (0.129) | 7.579 * (0.752) | |
| CG | 60.7 ± 13.00 | 64.5 ± 9.52 | 0.53 | ||||
| TMV (cm2) | RT | 74.8 ± 6.77 | 76.6 ± 7.48 | 0.44 | 4.872 * (0.196) | ||
| CG | 72.3 ± 8.86 | 71.0 ± 9.48 | 0.71 | ||||
| TSFV (cm2) | RT | 46.9 ± 17.36 | 46.3 ± 16.09 | 0.07 | 0.585 (0.028) | ||
| CG | 44.7 ± 10.89 | 46.4 ± 7.41 | 0.27 | ||||
| IMAT (cm2) | RT | 16.0 ± 4.60 | 15.4 ± 3.15 | 0.25 | 7.381 * (0.270) | ||
| CG | 16.1 ± 3.90 | 18.1 ± 3.75 ++ | 1.06 | ||||
| Muscle Growth Regulator | Follistatin (pg·mL−1) | RT | 2113.75 ± 409.28 | 2652.85 ± 704.18 + | 0.81 | 4.960 * (0.199) | 2.476 (0.292) |
| CG | 2241.85 ± 669.91 | 2255.45 ± 564.02 | 0.04 | ||||
| GDF-8 (pg·mL−1) | RT | 2294.43 ± 686.62 | 2193.11 ± 618.91 | 0.19 | 1.494 (0.070) | ||
| CG | 1616.52 ± 650.70 | 1784.22 ± 529.69 | 0.33 | ||||
| GDF-15 (pg·mL−1) | RT | 902.00 ± 406.93 | 961.81 ± 355.81 | 0.43 | 0.943 (0.045) | ||
| CG | 831.03 ± 262.84 | 949.32 ± 326.74 | 0.83 | ||||
| Activin A (pg·mL−1) | RT | 399.81 ± 93.59 | 362.42 ± 76.83 | 0.45 | 0.011 (0.001) | ||
| CG | 340.37 ± 61.61 | 305.94 ± 53.01 | 0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, M.-W.; Jung, S.-W.; Kim, S.-W.; Lee, J.-M.; Jung, H.C.; Song, J.-K. Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136762
Seo M-W, Jung S-W, Kim S-W, Lee J-M, Jung HC, Song J-K. Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(13):6762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136762
Chicago/Turabian StyleSeo, Myong-Won, Sung-Woo Jung, Sung-Woo Kim, Jung-Min Lee, Hyun Chul Jung, and Jong-Kook Song. 2021. "Effects of 16 Weeks of Resistance Training on Muscle Quality and Muscle Growth Factors in Older Adult Women with Sarcopenia: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 13: 6762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136762