
An Assessment of Health Outcomes and Methylmercury Exposure in Munduruku Indigenous Women of Childbearing Age and Their Children under 2 Years Old

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Population
2.2. Study Design
2.3. Data Collection
2.3.1. Interviews
2.3.2. Mercury Analysis
2.3.3. Nutritional Status
2.3.4. Neurological Status
2.4. Statistical Analysis
3. Results
3.1. Description of the Studied Population
3.2. Interviews
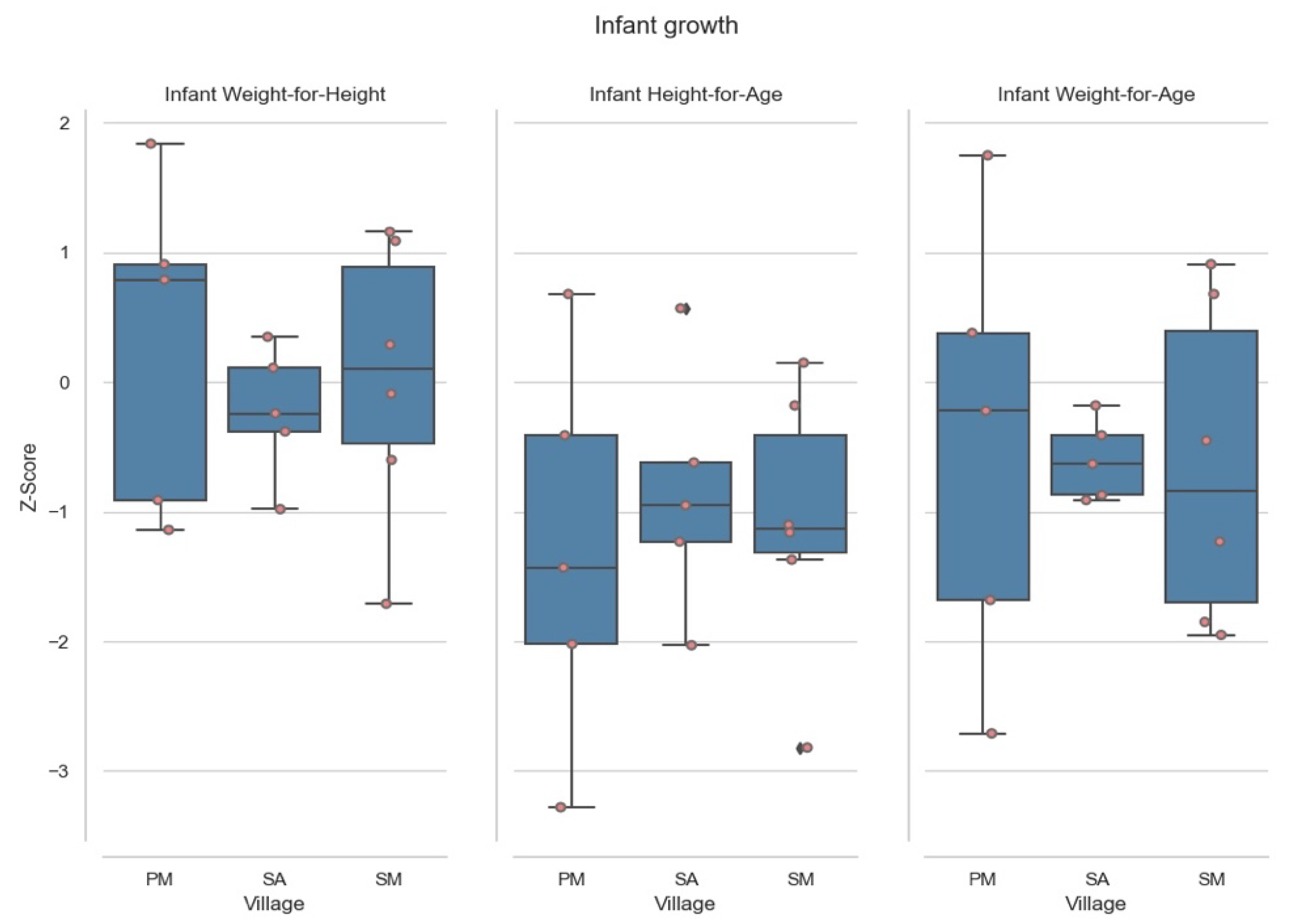
3.3. Nutritional Status Evaluation
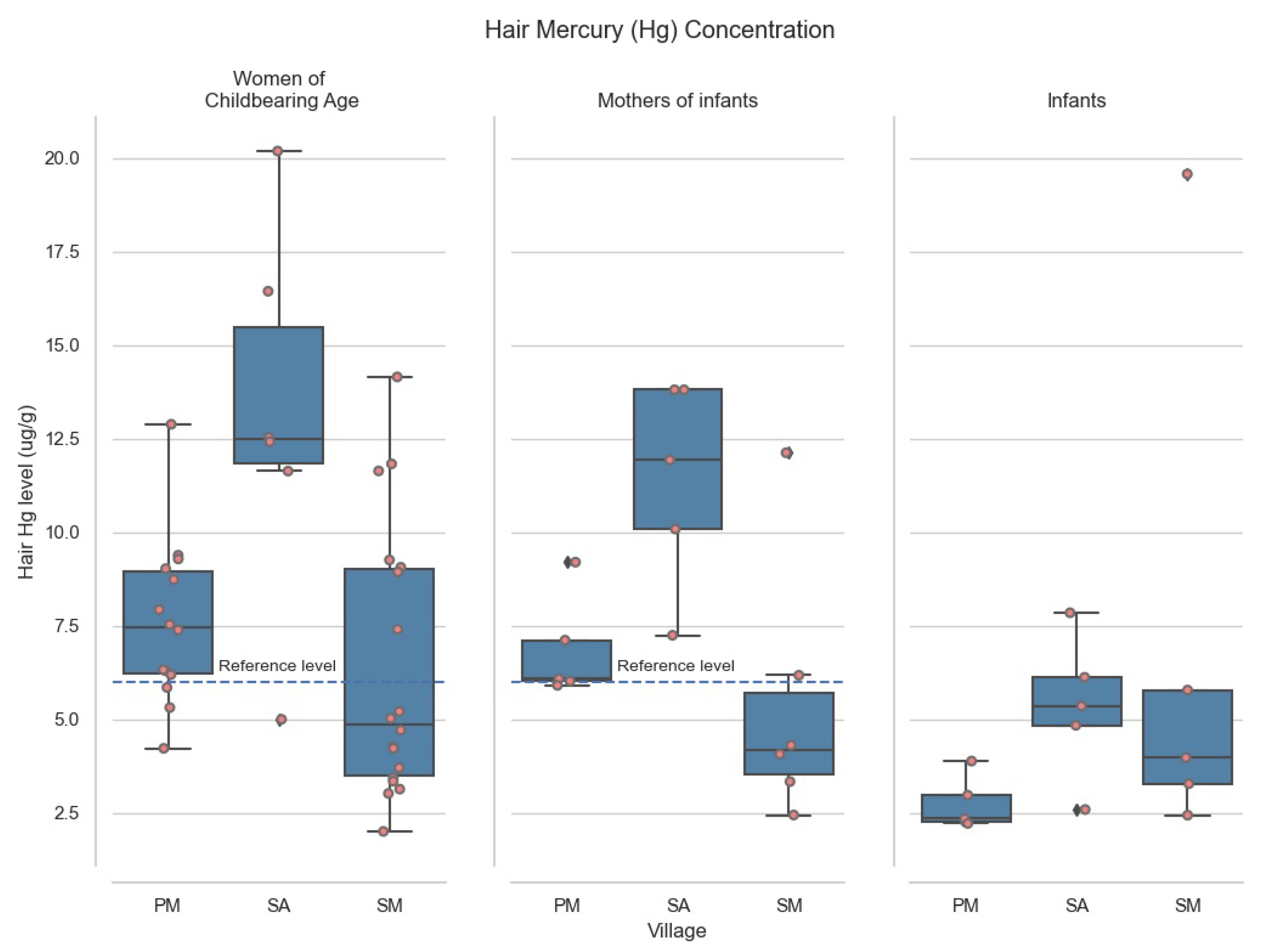
3.4. Hair Methylmercury Levels in Women of Childbearing Age
3.5. Hair Methylmercury Levels in Infants
3.6. Neurodevelopment Results of the Infants Studied under Two
3.7. Comparison between Villages
4. Discussion
4.1. H-Hg in Women of Childbearing Age
4.2. H-Hg in Infants
4.3. Interactions between Maternal and Infant H-Hg
4.4. H-Hg by Village
4.5. Nutrition and Growth
4.6. Infant Mortality
4.7. Where Can We Go from Here?
- Encourage training and education in nutritional best practices with a focus on the 1000 days window;
- Improve education around breastfeeding and encourage comprehensive weaning practices post six months;
- Identify those infants at risk of anemia, for example those with extended breastfeeding, and provide sufficient nutritional drinks and iron supplementation;
- Work closely with the National Unified health system and the Indigenous Special Sanitary Districts to help develop continuous, accessible, and culturally sensitive pre- (greater than four visits) and post-natal health care;
- Help develop methods to specifically catch those fish high in Omega-3′s and low in MeHg (i.e., those lower in the food chain);
- Encourage the Brazilian government to align with the Minamata convention and Planet Gold’s global initiative to reduce Mercury pollution in ASGM sites;
- Condemn the government for its active encouragement of illegal gold mining in the Munduruku area.
4.8. Limitations
5. Conclusions
- This study was borne out of a request from the leaders of these Munduruku communities, exemplifying the experience of vulnerability within the communities;
- These already vulnerable Munduruku communities suffer chronic exposure to levels of MeHg above 6.0 µg/g reference levels, known to negatively impact on adult health and infant growth and development;
- Ongoing health inequalities are contributing to higher rates of anemia, stunting and infant mortality, preventing individuals in these Munduruku communities from reaching their full potential;
- Simple, culturally sensitive intervention is needed to reduce poor health outcomes and interrupt this cycle of poverty.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Darling, J.C.; Bamidis, P.D.; Burberry, J.; Rudolf, M.C.J. The First Thousand Days: Early, Integrated and Evidence-Based Approaches to Improving Child Health: Coming to a Population near You? Arch. Dis. Child. 2020, 105, 837–841. [Google Scholar] [CrossRef] [PubMed]
- English, K.; Lau, C.; Jagals, P. The Unique Vulnerabilities of Children to Environmental Hazards. In Early-life Environmental Exposure and Disease: Facts and Perspectives; Xia, Y., Ed.; Springer: Singapore, 2020; pp. 103–112. ISBN 9789811537974. [Google Scholar]
- Dórea, J.G. Environmental Exposure to Low-Level Lead (Pb) Co-Occurring with Other Neurotoxicants in Early Life and Neurodevelopment of Children. Environ. Res. 2019, 177, 108641. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, T.; Axelrad, D.; Kyle, A.; Nweke, O.; Miller, G. America’s Children and the Environment: Measures of Contaminants, Body Burdens, and Illnesses; U.S. EPA: Cincinnati, OH, USA, 2003.
- House of Commons Health and Social Care Committee. Parliamentary Copyright House of Commons: First 1000 Days of Life. 2019, p. 58. Available online: https://publications.parliament.uk/pa/cm201719/cmselect/cmhealth/1496/1496.pdf (accessed on 12 August 2021).
- First 1000 Days Australia First 1000 Days Australia. Available online: https://www.first1000daysaustralia.com (accessed on 12 August 2021).
- Thousand Days Why 1000 Days. Available online: https://thousanddays.org/why-1000-days/ (accessed on 12 August 2021).
- United Nations Goal 2: Zero Hunger. Available online: https://www.un.org/sustainabledevelopment/hunger/ (accessed on 12 August 2021).
- United Nations Goal 2: Health. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 12 August 2021).
- Crespo-Lopez, M.E.; Augusto-Oliveira, M.; Lopes-Araújo, A.; Santos-Sacramento, L.; Yuki Takeda, P.; Macchi, B.d.M.; do Nascimento, J.L.M.; Maia, C.S.F.; Lima, R.R.; Arrifano, G.P. Mercury: What Can We Learn from the Amazon? Environ. Int. 2021, 146, 106223. [Google Scholar] [CrossRef] [PubMed]
- da Silva Brabo, E.; de Oliveira Santos, E.; de Jesus, I.M.; Mascarenhas, A.F.; de Freitas Faial, K. Mercury Contamination of Fish and Exposures of an Indigenous Community in Pará State, Brazil. Environ. Res. 2000, 84, 197–203. [Google Scholar] [CrossRef]
- de Vasconcellos, A.C.S.; Hallwass, G.; Bezerra, J.G.; Aciole, A.N.S.; Meneses, H.N.d.M.; Lima, M.d.O.; de Jesus, I.M.; Hacon, S.d.S.; Basta, P.C. Health Risk Assessment of Mercury Exposure from Fish Consumption in Munduruku Indigenous Communities in the Brazilian Amazon. Int. J. Environ. Res. Public Health 2021, 18, 7940. [Google Scholar] [CrossRef]
- Vega, C.M.; Orellana, J.D.Y.; Oliveira, M.W.; Hacon, S.S.; Basta, P.C. Human Mercury Exposure in Yanomami Indigenous Villages from the Brazilian Amazon. Int. J. Environ. Res. Public Health 2018, 15, 1051. [Google Scholar] [CrossRef] [Green Version]
- Dórea, J.G.; de Souza, J.R.; Rodrigues, P.; Ferrari, I.; Barbosa, A.C. Hair Mercury (Signature of Fish Consumption) and Cardiovascular Risk in Munduruku and Kayabi Indians of Amazonia. Environ. Res. 2005, 97, 209–219. [Google Scholar] [CrossRef]
- Santos, E.; de Jesus, I.; Câmara, V.; Brabo, E.; Loureiro, E.; Mascarenhas, A.; Weirich, J.; Luiz, R.; Cleary, D. Mercury Exposure in Munduruku Indians from the Community of Sai Cinza, State of Pará, Brazil. Environ. Res. 2002, 90, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Coimbra, C.E.; Santos, R.V.; Welch, J.R.; Cardoso, A.M.; de Souza, M.C.; Garnelo, L.; Rassi, E.; Follér, M.-L.; Horta, B.L. The First National Survey of Indigenous People’s Health and Nutrition in Brazil: Rationale, Methodology, and Overview of Results. BMC Public Health 2013, 13, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Leite, M.S.; Cardoso, A.M.; Coimbra, C.E.; Welch, J.R.; Gugelmin, S.A.; Lira, P.C.I.; Horta, B.L.; Santos, R.V.; Escobar, A.L. Prevalence of Anemia and Associated Factors among Indigenous Children in Brazil: Results from the First National Survey of Indigenous People’s Health and Nutrition. Nutr. J. 2013, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Orellana, J.D.Y.; Coimbra, C.E.A., Jr.; Lourenço, A.E.P.; Santos, R.V. Estado nutricional e anemia em crianças Suruí, Amazônia, Brasil. J. Pediatr. (Rio J.) 2006, 82, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Orellana, J.D.Y.; Gatica-Domínguez, G.; Vaz, J.d.S.; Neves, P.A.R.; de Vasconcellos, A.C.S.; de Souza Hacon, S.; Basta, P.C. Intergenerational Association of Short Maternal Stature with Stunting in Yanomami Indigenous Children from the Brazilian Amazon. Int. J. Environ. Res. Public Health 2021, 18, 9130. [Google Scholar] [CrossRef] [PubMed]
- Orellana, J.D.Y.; Marrero, L.; Alves, C.L.M.; Ruiz, C.M.V.; Hacon, S.S.; Oliveira, M.W.; Basta, P.C. Association of severe stunting in indigenous Yanomami children with maternal short stature: Clues about the intergerational transmission. Cien Saude Colet 2019, 24, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Manjong, F.T.; Verla, V.S.; Egbe, T.O.; Nsagha, D.S. Risk Factors of under Nutrition among Indigenous Children under Five Years in Developing Countries: A Scoping Review. J. Public Health Epidemiol. 2020, 12, 340–348. [Google Scholar] [CrossRef]
- Cunha, M.P.L.; Marques, R.C.; Dórea, J.G. Child Nutritional Status in the Changing Socioeconomic Region of the Northern Amazon, Brazil. Int. J. Environ. Res. Public Health 2017, 15, 15. [Google Scholar] [CrossRef] [Green Version]
- Santos, R.V.; Borges, G.M.; de Campos, M.B.; Queiroz, B.L.; Coimbra, C.E.A.; Welch, J.R. Indigenous Children and Adolescent Mortality Inequity in Brazil: What Can We Learn from the 2010 National Demographic Census? SSM Popul. Health 2020, 10, 100537. [Google Scholar] [CrossRef]
- Gava, C.; Cardoso, A.M.; Basta, P.C. Infant Mortality by Color or Race from Rondônia, Brazilian Amazon. Rev. Saúde Pública 2017, 51, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Lobo, F.D.L.; Costa, M.; Novo, E.M.L.d.M.; Telmer, K. Distribution of Artisanal and Small-Scale Gold Mining in the Tapajós River Basin (Brazilian Amazon) over the Past 40 Years and Relationship with Water Siltation. Remote Sens. 2016, 8, 579. [Google Scholar] [CrossRef] [Green Version]
- Asner, G.P.; Llactayo, W.; Tupayachi, R.; Luna, E.R. Elevated Rates of Gold Mining in the Amazon Revealed through High-Resolution Monitoring. Proc. Natl. Acad. Sci. USA 2013, 110, 18454–18459. [Google Scholar] [CrossRef] [Green Version]
- Cremers, L.; De Theije, M. Small-Scale Gold Mining in the Amazon. Small-Scale Gold Min. Amaz. 2013, 1, 1–16. [Google Scholar]
- Guimarães, J.R.D.; Roulet, M.; Lucotte, M.; Mergler, D. Mercury Methylation along a Lake–Forest Transect in the Tapajós River Floodplain, Brazilian Amazon: Seasonal and Vertical Variations. Sci. Total Environ. 2000, 261, 91–98. [Google Scholar] [CrossRef]
- Santos-Sacramento, L.; Arrifano, G.P.; Lopes-Araújo, A.; Augusto-Oliveira, M.; Albuquerque-Santos, R.; Takeda, P.Y.; Souza-Monteiro, J.R.; Macchi, B.M.; do Nascimento, J.L.M.; Lima, R.R.; et al. Human Neurotoxicity of Mercury in the Amazon: A Scoping Review with Insights and Critical Considerations. Ecotoxicol. Environ. Saf. 2021, 208, 111686. [Google Scholar] [CrossRef]
- Lebel, J.; Mergler, D.; Branches, F.; Lucotte, M.; Amorim, M.; Larribe, F.; Dolbec, J. Neurotoxic Effects of Low-Level Methylmercury Contamination in the Amazonian Basin. Environ. Res. 1998, 79, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; White, R.F.; Nielsen, A.; Cleary, D.; de Oliveira Santos, E.C. Methylmercury Neurotoxicity in Amazonian Children Downstream from Gold Mining. Environ. Health Perspect. 1999, 107, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Dolbec, J.; Mergler, D.; Sousa Passos, C.-J.; Sousa de Morais, S.; Lebel, J. Methylmercury Exposure Affects Motor Performance of a Riverine Population of the Tapajós River, Brazilian Amazon. Int. Arch. Occup. Environ. Health 2000, 73, 195–203. [Google Scholar] [CrossRef]
- Khoury, E.D.T.; Souza, G.d.S.; Costa, C.A.d.; Araújo, A.A.K.d.; Oliveira, C.S.B.d.; Silveira, L.C.d.L.; Pinheiro, M.d.C.N. Somatosensory Psychophysical Losses in Inhabitants of Riverside Communities of the Tapajós River Basin, Amazon, Brazil: Exposure to Methylmercury Is Possibly Involved. PLoS ONE 2015, 10, e0144625. [Google Scholar] [CrossRef]
- Oliveira, C.S.; Nogara, P.A.; Ardisson-Araújo, D.M.P.; Aschner, M.; Rocha, J.B.T.; Dórea, J.G. Neurodevelopmental Effects of Mercury. Adv. Neurotoxicol. 2018, 2, 27–86. [Google Scholar] [CrossRef]
- Nyland, J.F.; Wang, S.B.; Shirley, D.L.; Santos, E.O.; Ventura, A.M.; de Souza, J.M.; Silbergeld, E.K. Fetal and Maternal Immune Responses to Methylmercury Exposure: A Cross-Sectional Study. Environ. Res. 2011, 111, 584–589. [Google Scholar] [CrossRef] [Green Version]
- Cordier, S.; Garel, M.; Mandereau, L.; Morcel, H.; Doineau, P.; Gosme-Seguret, S.; Josse, D.; White, R.; Amiel-Tison, C. Neurodevelopmental Investigations among Methylmercury-Exposed Children in French Guiana. Environ. Res. 2002, 89, 1–11. [Google Scholar] [CrossRef] [Green Version]
- dos Santos Freitas, J.; da Costa Brito Lacerda, E.M.; da Silva Martins, I.C.V.; Rodrigues, D.; Bonci, D.M.O.; Cortes, M.I.T.; Corvelo, T.C.O.; Ventura, D.F.; de Lima Silveira, L.C.; da Conceição Nascimento Pinheiro, M.; et al. Cross-Sectional Study to Assess the Association of Color Vision with Mercury Hair Concentration in Children from Brazilian Amazonian Riverine Communities. NeuroToxicology 2018, 65, 60–67. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; McCarty, K.M.; Steckling, N.; Lettmeier, B. Mercury Exposure and Children’s Health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 186–215. [Google Scholar] [CrossRef] [Green Version]
- Bose-O’Reilly, S.; Lettmeier, B.; Matteucci Gothe, R.; Beinhoff, C.; Siebert, U.; Drasch, G. Mercury as a Serious Health Hazard for Children in Gold Mining Areas. Environ. Res. 2008, 107, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Koos, B.J.; Longo, L.D. Mercury Toxicity in the Pregnant Woman, Fetus, and Newborn Infant: A Review. Am. J. Obstet. Gynecol. 1976, 126, 390–409. [Google Scholar] [CrossRef]
- Santos-Lima, C.d.; Mourão, D.d.S.; Carvalho, C.F.d.; Souza-Marques, B.; Vega, C.M.; Gonçalves, R.A.; Argollo, N.; Menezes-Filho, J.A.; Abreu, N.; Hacon, S.d.S. Neuropsychological Effects of Mercury Exposure in Children and Adolescents of the Amazon Region, Brazil. NeuroToxicology 2020, 79, 48–57. [Google Scholar] [CrossRef]
- Stern, A.H.; Smith, A.E. An Assessment of the Cord Blood:Maternal Blood Methylmercury Ratio: Implications for Risk Assessment. Env. Health Perspect. 2003, 111, 1465–1470. [Google Scholar] [CrossRef] [Green Version]
- Reuben, A.; Frischtak, H.; Berky, A.; Ortiz, E.J.; Morales, A.M.; Hsu-Kim, H.; Pendergast, L.L.; Pan, W.K. Elevated Hair Mercury Levels Are Associated with Neurodevelopmental Deficits in Children Living Near Artisanal and Small-Scale Gold Mining in Peru. GeoHealth 2020, 4, e2019GH000222. [Google Scholar] [CrossRef]
- Joint, F.A.O.; WHO Expert Committee on Food Additives; World Health Organization. Evaluation of Certain Food Additives and the Contaminants Mercury, Lead, and Cadmium: Sixteenth Report of the Joint FAO/WHO Expert Committee on Food Additives, Geneva, 4–12 April 1972; World Health Organization: Geneva, Switzerland, 1972. [Google Scholar]
- US EPA. Reference Dose for Methylmercury (External Review Draft, 2000); U.S. Environmental Protection Agency: Washington, DC, USA, 2000.
- WHO; FAO. Evaluation of Certain Food Additives and Contaminants: Sixty-First Report of the Joint FAO/WHO Expert Committee on Food Additives; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Joint, F.A.O.; WHO Expert Committee on Food Additives. Toxicological Evaluation of Certain Food Additives and Contaminants; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Crump, K.S.; Kjellström, T.; Shipp, A.M.; Silvers, A.; Stewart, A. Influence of Prenatal Mercury Exposure upon Scholastic and Psychological Test Performance: Benchmark Analysis of a New Zealand Cohort. Risk Anal. 1998, 18, 701–713. [Google Scholar] [CrossRef]
- Marinho, J.S.; Lima, M.O.; de Oliveira Santos, E.C.; de Jesus, I.M.; da Conceição, N.; Pinheiro, M.; Alves, C.N.; Muller, R.C.S. Mercury Speciation in Hair of Children in Three Communities of the Amazon, Brazil. Biomed. Res. Int 2014, 2014, 945963. [Google Scholar] [CrossRef] [PubMed]
- De Castro, N.S.S.; Lima, M.D.O. Hair as a Biomarker of Long Term Mercury Exposure in Brazilian Amazon: A Systematic Review. Int. J. Environ. Res. Public Heal. 2018, 15, 500. [Google Scholar] [CrossRef] [Green Version]
- Bastos, W.R.; Gomes, J.P.O.; Oliveira, R.C.; Almeida, R.; Nascimento, E.L.; Bernardi, J.V.E.; de Lacerda, L.D.; da Silveira, E.G.; Pfeiffer, W.C. Mercury in the Environment and Riverside Population in the Madeira River Basin, Amazon, Brazil. Sci. Total Environ. 2006, 368, 344–351. [Google Scholar] [CrossRef]
- Basta, P.C.; Viana, P.V.S.; Vasconcellos, A.C.; Perisse, A.R.S.; Hofer, C.B.; Paifa, N.S.; Kempton, J.W.; Ciampi de Andrade, D.; Oliveira, R.A.A.; Achatz, R.W.; et al. Mercury Exposure in Munduruku Indigenous Communities from Brazilian Amazon: Methodologi-Cal Background and an Overview of the Principal Results. Int. J. Environ. Res. Public Health 2021, 18, 9222. [Google Scholar] [CrossRef] [PubMed]
- Joint, F.A.O. WHO Food Standards Programme Codex Committee on Contaminants in Foods Tenth Session Rotterdam, The Netherlands; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Achatz, R.W.; Vasconcellos, A.C.; Pereira, L.; Viana, P.V.S.; Basta, P.C. Impacts of the Goldmining and Chronic Methylmercury Exposure on the Good-Living and Mental Health of Munduruku Native Communities in the Amazon Basin. Int. J. Environ. Res. Public Health 2021, 18, 8994. [Google Scholar] [CrossRef]
- PNI. Calendário Nacional de Vacinação Dos Povos Indígenas; Secretaria de estado de saude: Goiania, Brazil, 2020. [Google Scholar]
- Estima, N.M.; Alves, S.V. Mortes Maternas e de Mulheres Em Idade Reprodutiva Na População Indígena, Pernambuco, 2006–2012 *. Epidemiol. E Serviços De Saúde 2019, 28, 2–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garnelo, L.; Horta, B.L.; Escobar, A.L.; Santos, R.V.; Cardoso, A.M.; Welch, J.R.; Tavares, F.G.; Coimbra, C.E.A., Jr. Avaliação da atenção pré-natal ofertada às mulheres indígenas no Brasil: Achados do Primeiro Inquérito Nacional de Saúde e Nutrição dos Povos Indígenas. Cad. Saúde Pública 2019, 35, e00181318. [Google Scholar] [CrossRef] [PubMed]
- Marrugo-Negrete, J.; Verbel, J.O.; Ceballos, E.L.; Benitez, L.N. Total Mercury and Methylmercury Concentrations in Fish from the Mojana Region of Colombia. Env. Geochem. Health 2008, 30, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Kehrig, H.A.; Costa, M.; Moreira, I.; Malm, O. Total and Methylmercury in a Brazilian Estuary, Rio de Janeiro. Mar. Pollut. Bull. 2002, 44, 1018–1023. [Google Scholar] [CrossRef]
- Souza-Araujo, J.; Giarrizzo, T.; Lima, M.O.; Souza, M.B.G. Mercury and Methyl Mercury in Fishes from Bacajá River (Brazilian Amazon): Evidence for Bioaccumulation and Biomagnification. J. Fish. Biol. 2016, 89, 249–263. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidance for Identifying Populations at Risk from Mercury Exposure; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Berglund, M.; Lind, B.; Björnberg, K.A.; Palm, B.; Einarsson, O.; Vahter, M. Inter-Individual Variations of Human Mercury Exposure Biomarkers: A Cross-Sectional Assessment. Env. Health 2005, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Clarkson, T.W.; Magos, L. The Toxicology of Mercury and Its Chemical Compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. Available online: https://www.who.int/publications-detail-redirect/924154693X (accessed on 14 August 2021).
- Frankenburg, W.K.; Dodds, J.; Archer, P.; Shapiro, H.; Bresnick, B. The Denver II: A Major Revision and Restandardization of the Denver Developmental Screening Test. Pediatrics 1992, 89, 91–97. [Google Scholar] [PubMed]
- Harada, M.; Nakanishi, J.; Yasoda, E.; Pinheiro, M.d.C.N.; Oikawa, T.; de Assis Guimarâes, G.; da silva Cardoso, B.; Kizaki, T.; Ohno, H. Mercury Pollution in the Tapajos River Basin, Amazon: Mercury Level of Head Hair and Health Effects. Environ. Int. 2001, 27, 285–290. [Google Scholar] [CrossRef]
- Malm, O.; Guimarães, J.R.D.; Castro, M.B.; Bastos, W.R.; Viana, J.P.; Branches, F.J.P.; Silveira, E.G.; Pfeiffer, W.C. Follow-up of Mercury Levels in Fish, Human Hair and Urine in the Madeira and Tapajós Basins, Amazon, Brazil. Water Air Soil Pollut. 1997, 97, 45–51. [Google Scholar] [CrossRef]
- Berzas Nevado, J.J.; Rodríguez Martín-Doimeadios, R.C.; Guzmán Bernardo, F.J.; Jiménez Moreno, M.; Herculano, A.M.; do Nascimento, J.L.M.; Crespo-López, M.E. Mercury in the Tapajós River Basin, Brazilian Amazon: A Review. Environ. Int. 2010, 36, 593–608. [Google Scholar] [CrossRef]
- Barbosa, A.C.; Silva, S.R.L.; Dórea, J.G. Concentration of Mercury in Hair of Indigenous Mothers and Infants from the Amazon Basin. Arch. Environ. Contam. Toxicol. 1998, 34, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, A.C.; Jardim, W.; Dórea, J.G.; Fosberg, B.; Souza, J. Hair Mercury Speciation as a Function of Gender, Age, and Body Mass Index in Inhabitants of the Negro River Basin, Amazon, Brazil. Arch. Environ. Contam. Toxicol. 2001, 40, 439–444. [Google Scholar] [CrossRef]
- Oliveira, R.C.; Dórea, J.G.; Bernardi, J.V.E.; Bastos, W.R.; Almeida, R.; Manzatto, A.G. Fish Consumption by Traditional Subsistence Villagers of the Rio Madeira (Amazon): Impact on Hair Mercury. Ann. Hum. Biol. 2010, 37, 629–642. [Google Scholar] [CrossRef]
- Vieira, S.M.; de Almeida, R.; Holanda, I.B.B.; Mussy, M.H.; Galvão, R.C.F.; Crispim, P.T.B.; Dórea, J.G.; Bastos, W.R. Total and Methyl-Mercury in Hair and Milk of Mothers Living in the City of Porto Velho and in Villages along the Rio Madeira, Amazon, Brazil. Int. J. Hyg. Environ. Health 2013, 216, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Geer, L.A.; Persad, M.D.; Palmer, C.D.; Steuerwald, A.J.; Dalloul, M.; Abulafia, O.; Parsons, P.J. Assessment of Prenatal Mercury Exposure in a Predominately Caribbean Immigrant Community in Brooklyn, NY. J. Environ. Monit. 2012, 14, 1035. [Google Scholar] [CrossRef] [PubMed]
- Björnberg, K.A.; Vahter, M.; Petersson-Grawé, K.; Glynn, A.; Cnattingius, S.; Darnerud, P.O.; Atuma, S.; Aune, M.; Becker, W.; Berglund, M. Methyl Mercury and Inorganic Mercury in Swedish Pregnant Women and in Cord Blood: Influence of Fish Consumption. Environ. Health Perspect. 2003, 111, 637–641. [Google Scholar] [CrossRef] [Green Version]
- Muckle, G.; Ayotte, P.; Dewailly, E.; Jacobson, S.; Jacobson, J. Prenatal Exposure of the Northern Québec Inuit Infants to Environmental Contaminants. Environ. Health Perspect. 2001, 109, 1291–1299. [Google Scholar]
- Fletcher, A.M.; Gelberg, K.H. An Analysis of Mercury Exposures Among the Adult Population in New York State. J. Community Health 2013, 38, 529–537. [Google Scholar] [CrossRef]
- Woods, J.S.; Heyer, N.J.; Echeverria, D.; Russo, J.E.; Martin, M.D.; Bernardo, M.F.; Luis, H.S.; Vaz, L.; Farin, F.M. Modification of Neurobehavioral Effects of Mercury by a Genetic Polymorphism of Coproporphyrinogen Oxidase in Children. Neurotoxicol. Teratol. 2012, 34, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Arrifano, G.P.F.; Martín-Doimeadios, R.C.R.; Jiménez-Moreno, M.; Fernández-Trujillo, S.; Augusto-Oliveira, M.; Souza-Monteiro, J.R.; Macchi, B.M.; Alvarez-Leite, J.I.; do Nascimento, J.L.M.; Amador, M.T.; et al. Genetic Susceptibility to Neurodegeneration in Amazon: Apolipoprotein E Genotyping in Vulnerable Populations Exposed to Mercury. Front. Genet. 2018, 9, 285. [Google Scholar] [CrossRef] [Green Version]
- Gundacker, C.; Gencik, M.; Hengstschläger, M. The Relevance of the Individual Genetic Background for the Toxicokinetics of Two Significant Neurodevelopmental Toxicants: Mercury and Lead. Mutat. Res. 2010, 705, 130–140. [Google Scholar] [CrossRef]
- Perini, J.A.; Silva, M.C.; Vasconcellos, A.C.S.d.; Viana, P.V.S.; Lima, M.O.; Jesus, I.M.; Kempton, J.W.; Oliveira, R.A.A.; Hacon, S.S.; Basta, P.C. Genetic Polymorphism of Delta Aminolevulinic Acid Dehydratase (ALAD) Gene and Symptoms of Chronic Mercury Exposure in Munduruku Indigenous Children within the Brazilian Amazon. Int. J. Environ. Res. Public Health 2021, 18, 8746. [Google Scholar] [CrossRef]
- Basu, N.; Horvat, M.; Evers, D.C.; Zastenskaya, I.; Weihe, P.; Tempowski, J. A State-of-the-Science Review of Mercury Biomarkers in Human Populations Worldwide between 2000 and 2018. Environ. Health Perspect 2018, 126, 106001. [Google Scholar] [CrossRef] [Green Version]
- Yokoo, E.M.; Valente, J.G.; Grattan, L.; Schmidt, S.L.; Platt, I.; Silbergeld, E.K. Low Level Methylmercury Exposure Affects Neuropsychological Function in Adults. Environ. Health 2003, 2, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Raposo, R.d.S.; Pinto, D.V.; Moreira, R.; Dias, R.P.; Fontes Ribeiro, C.A.; Oriá, R.B.; Malva, J.O. Methylmercury Impact on Adult Neurogenesis: Is the Worst Yet to Come from Recent Brazilian Environmental Disasters? Front. Aging. Neurosci. 2020, 12, 394. [Google Scholar] [CrossRef] [PubMed]
- Silbernagel, S.M.; Carpenter, D.O.; Gilbert, S.G.; Gochfeld, M.; Groth, E.; Hightower, J.M.; Schiavone, F.M. Recognizing and Preventing Overexposure to Methylmercury from Fish and Seafood Consumption: Information for Physicians. J. Toxicol. 2011, 2011, e983072. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.C.; Abreu, L.; Bernardi, J.V.E.; Dórea, J.G. Traditional Living in the Amazon: Extended Breastfeeding, Fish Consumption, Mercury Exposure and Neurodevelopment. Ann. Hum. Biol. 2016, 43, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.C.; Bernardi, J.V.E.; Dórea, J.G.; de Fatima, R.; Moreira, M.; Malm, O. Perinatal Multiple Exposure to Neurotoxic (Lead, Methylmercury, Ethylmercury, and Aluminum) Substances and Neurodevelopment at Six and 24 Months of Age. Environ. Pollut. 2014, 187, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.G.; Marques, R.C.; Isejima, C. Neurodevelopment of Amazonian Infants: Antenatal and Postnatal Exposure to Methyl- and Ethylmercury. J. Biomed. Biotechnol. 2012, 2012, e132876. [Google Scholar] [CrossRef] [Green Version]
- Barbone, F.; Valent, F.; Pisa, F.; Daris, F.; Fajon, V.; Gibicar, D.; Logar, M.; Horvat, M. Prenatal Low-Level Methyl Mercury Exposure and Child Development in an Italian Coastal Area. NeuroToxicology 2020, 81, 376–381. [Google Scholar] [CrossRef]
- Marques, R.C.; Dórea, J.G.; McManus, C.; Leão, R.S.; Brandão, K.G.; Marques, R.C.; Vieira, I.H.I.; Guimarães, J.-R.D.; Malm, O. Hydroelectric Reservoir Inundation (Rio Madeira Basin, Amazon) and Changes in Traditional Lifestyle: Impact on Growth and Neurodevelopment of Pre-School Children. Public Health Nutr. 2011, 14, 661–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golding, J.; Gregory, S.; Iles-Caven, Y.; Hibbeln, J.; Emond, A.; Taylor, C.M. Associations between Prenatal Mercury Exposure and Early Child Development in the ALSPAC Study. Neurotoxicology 2016, 53, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Children’s Health and the Environment. A Global Perspective: A Resource Manual for the Health Sector; Pronczuk-Garbino, J., Ed.; World Health Organization: Geneva, Switzerland, 2005; ISBN 978-92-4-156292-8. [Google Scholar]
- Ruggieri, F.; Majorani, C.; Domanico, F.; Alimonti, A. Mercury in Children: Current State on Exposure through Human Biomonitoring Studies. Int. J. Environ. Res. Public Health 2017, 14, 519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, E.O.; Jesus, I.M.d.; Câmara, V.d.M.; Brabo, E.d.S.; Jesus, M.I.d.; Fayal, K.F.; Asmus, C.I.R.F. Correlation between Blood Mercury Levels in Mothers and Newborns in Itaituba, Pará State, Brazil. Cad. Saude Publica 2007, 23, S622–S629. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, M.; Murata, K.; Nakai, K.; Satoh, H. Difference in Methylmercury Exposure to Fetus and Breast-Feeding Offspring: A Mini-Review. J. Environ. Health Sci. 2015, 31, 179–186. [Google Scholar]
- Grandjean, P.; Jørgensen, P.J.; Weihe, P. Human Milk as a Source of Methylmercury Exposure in Infants. Env. Health Perspect 1994, 102, 74–77. [Google Scholar] [CrossRef] [Green Version]
- Marques, R.C.; Dórea, J.G.; Bastos, W.R.; Malm, O. Changes in Children Hair-Hg Concentrations during the First 5 Years: Maternal, Environmental and Iatrogenic Modifying Factors. Regul. Toxicol. Pharm. 2007, 49, 17–24. [Google Scholar] [CrossRef]
- National Research Council. Risk Characterization and Public Health Implications. In Toxicological Effects of Methylmercury; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Passos, C.J.S.; Mergler, D.; Lemire, M.; Fillion, M.; Guimarães, J.R.D. Fish Consumption and Bioindicators of Inorganic Mercury Exposure. Sci. Total Environ. 2007, 373, 68–76. [Google Scholar] [CrossRef]
- Dolbec, J.; Mergler, D.; Larribe, F.; Roulet, M.; Lebel, J.; Lucotte, M. Sequential Analysis of Hair Mercury Levels in Relation to Fish Diet of an Amazonian Population, Brazil. Sci. Total Environ. 2001, 271, 87–97. [Google Scholar] [CrossRef]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Khambalia, A.Z.; Aimone, A.M.; Zlotkin, S.H. Burden of Anemia among Indigenous Populations. Nutr. Rev. 2011, 69, 693–719. [Google Scholar] [CrossRef] [PubMed]
- McCann, J.C.; Ames, B.N. An Overview of Evidence for a Causal Relation between Iron Deficiency during Development and Deficits in Cognitive or Behavioral Function. Am. J. Clin. Nutr. 2007, 85, 931–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.; Hector, D. Benefits of Breastfeeding. N S W Public Health Bull. 2005, 16, 42–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNICEF. Breastfeeding: A Mother’s Gift, for Every Child; United Nations Children’s Fund: New York, NY, USA, 2018. [Google Scholar]
- Dube, K.; Schwartz, J.; Mueller, M.J.; Kalhoff, H.; Kersting, M. Iron Intake and Iron Status in Breastfed Infants during the First Year of Life. Clin. Nutr. 2010, 29, 773–778. [Google Scholar] [CrossRef]
- Friel, J.K.; Aziz, K.; Andrews, W.L.; Harding, S.V.; Courage, M.L.; Adams, R.J. A Double-Masked, Randomized Control Trial of Iron Supplementation in Early Infancy in Healthy Term Breast-Fed Infants. J. Pediatr. 2003, 143, 582–586. [Google Scholar] [CrossRef]
- Baker, R.D.; Greer, F.R.; Nutrition, T.C. on Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0–3 Years of Age). Pediatrics 2010, 126, 1040–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sing, K.A.; Hryhorczuk, D.; Saffirio, G.; Sinks, T.; Paschal, D.C.; Sorensen, J.; Chen, E.H. Organic Mercury Levels among the Yanomama of the Brazilian Amazon Basin. Ambio A J. Hum. Environ. 2003, 32, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Bánhidy, F.; Ács, N.; Puhó, E.H.; Czeizel, A.E. Iron Deficiency Anemia: Pregnancy Outcomes with or without Iron Supplementation. Nutrition 2011, 27, 65–72. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T. Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. J. Nutr. 2001, 131, 676S–688S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bothwell, T.H. Iron Requirements in Pregnancy and Strategies to Meet Them. Am. J. Clin. Nutr. 2000, 72, 257S–264S. [Google Scholar] [CrossRef]
- World Health Organization. Prevalence of Anaemia in Women of Reproductive Age (Aged 15–49) (%); WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Dorea, J.; Barbosa, A.C.; Ferrari, I.; de Souza, J.R. Mercury in Hair and in Fish Consumed by Riparian Women of the Rio Negro, Amazon, Brazil. Int. J. Environ. Health Res. 2003, 13, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.C.; Bernardi, J.V.E.; Dorea, C.C.; Dórea, J.G. Intestinal Parasites, Anemia and Nutritional Status in Young Children from Transitioning Western Amazon. Int. J. Environ. Res. Public Health 2020, 17, 577. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, G.F.; Oliveira, T.R.R.; Ikejiri, A.T.; Galvao, T.F.; Silva, M.T.; Pereira, M.G. Prevalence of Obesity and Overweight in an Indigenous Population in Central Brazil: A Population-Based Cross-Sectional Study. Obes. Facts 2015, 8, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Capelli, J.D.C.S.; Koifman, S. Avaliação do estado nutricional da comunidade indígena Parkatêjê, Bom Jesus do Tocantins, Pará, Brasil. Cad. Saúde Pública 2001, 17, 433–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valeggia, C.R.; Snodgrass, J.J. Health of Indigenous Peoples. Annu. Rev. Anthropol. 2015, 44, 117–135. [Google Scholar] [CrossRef] [Green Version]
- Eggersdorfer, M.; Kraemer, K.; Ruel, M.; Van Ameringen, M.; Biesalski, H.K.; Bloem, M.; Chen, J.; Lateef, A.; Mannar, V. The Road to Good Nutrition: Basel, Switzerland; 2013; ISBN 978-3-318-02550-7. Available online: https://www.nutri-facts.org/content/dam/nutrifacts/media/media-books/The_Road_to_Good_Nutrition.pdf (accessed on 14 August 2021).
- Gubert, M.B.; Spaniol, A.M.; Segall-Corrêa, A.M.; Pérez-Escamilla, R. Understanding the Double Burden of Malnutrition in Food Insecure Households in Brazil. Matern. Child Nutr. 2017, 13, e12347. [Google Scholar] [CrossRef]
- Gracey, M.; King, M. Indigenous Health Part 1: Determinants and Disease Patterns. Lancet 2009, 374, 65–75. [Google Scholar] [CrossRef]
- Tallman, P.S.; Valdes-Velasquez, A.; Sanchez-Samaniego, G. The “Double Burden of Malnutrition” in the Amazon: Dietary Change and Drastic Increases in Obesity and Anemia over 40 Years among the Awajún. Ecol. Food Nutr. 2021, 26, 1–23. [Google Scholar] [CrossRef]
- Ramirez-Zea, M.; Kroker-Lobos, M.F.; Close-Fernandez, R.; Kanter, R. The Double Burden of Malnutrition in Indigenous and Nonindigenous Guatemalan Populations. Am. J. Clin. Nutr. 2014, 100, 1644S–1651S. [Google Scholar] [CrossRef] [Green Version]
- Piperata, B.A. Nutritional Status of Ribeirinhos in Brazil and the Nutrition Transition. Am. J. Phys. Anthropol. 2007, 133, 868–878. [Google Scholar] [CrossRef]
- DETER-INPE. Deforesation Warning; Instituto Nacional de Pesquisas Espaciais: São Paulo, Brazil, 2020. [Google Scholar]
- Christian, P.; Murray-Kolb, L.E.; Khatry, S.K.; Katz, J.; Schaefer, B.A.; Cole, P.M.; Leclerq, S.C.; Tielsch, J.M. Prenatal Micronutrient Supplementation and Intellectual and Motor Function in Early School-Aged Children in Nepal. JAMA 2010, 304, 2716–2723. [Google Scholar] [CrossRef] [Green Version]
- Murray-Kolb, L.E.; Khatry, S.K.; Katz, J.; Schaefer, B.A.; Cole, P.M.; LeClerq, S.C.; Morgan, M.E.; Tielsch, J.M.; Christian, P. Preschool Micronutrient Supplementation Effects on Intellectual and Motor Function in School-Aged Nepalese Children. Arch. Pediatr. Adolesc. Med. 2012, 166, 404–410. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Office of Research the First 1000 Days of Life: The Brain’s Window of Opportunity. 2013. Available online: https://www.unicef-irc.org/article/958-the-first-1000-days-of-life-the-brains-window-of-opportunity.html (accessed on 15 August 2021).
- Lima, M.; Rego, L.; Valente Correa, P.; Trindade, L.; Rodrigues, I.; Nogueira, L. Infant Mortality among Indigenous People in the State of Pará. Rev. Eletr. Enferm. 2020, 22, 1–8. [Google Scholar]
- Teixeira, J.J.d.M.B.; Santos, D.R.d.; Rocha, M.S.F.M.; Silva, S.C.R.d. Aspectos étnicos da mortalidade infantil: Uma contribuição para a vigilância de óbitos na população indígena e não indígena no Pará. Para. Res. Med. J. 2019, 3, e14. [Google Scholar] [CrossRef]
- World Bank Mortality Rate, Infant (per 1000 Live Births)—Brazil | Data. Available online: https://data.worldbank.org/indicator/SP.DYN.IMRT.IN?locations=BR (accessed on 15 August 2021).
- World Health Organization. Children: Improving Survival and Well-Being. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 15 August 2021).
- Alkema, L.; Chao, F.; You, D.; Pedersen, J.; Sawyer, C.C. National, Regional, and Global Sex Ratios of Infant, Child, and under-5 Mortality and Identification of Countries with Outlying Ratios: A Systematic Assessment. Lancet Glob. Health 2014, 2, e521–e530. [Google Scholar] [CrossRef] [Green Version]
- Lansky, S.; Friche, A.A.d.L.; Silva, A.A.M.d.; Campos, D.; Bittencourt, S.D.d.A.; Carvalho, M.L.d.; Frias, P.G.d.; Cavalcante, R.S.; Cunha, A.J.L.A.d. Birth in Brazil Survey: Neonatal Mortality, Pregnancy and Childbirth Quality of Care. Cad. Saúde Pública 2014, 30, S192–S207. [Google Scholar] [CrossRef]
- Souza, P.G.d.; Cardoso, A.M.; Sant’Anna, C.C.; March, M.d.F.B.P. Acute Lower Respiratory Infection in Guarani Indigenous Children, Brazil. Rev. Paul Pediatr. 2018, 36, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, J.B.; Bossolani, G.D.P.; Piva, C.; Dias, G.B.M.; Gomes Ferreira, J.; Rossoni, D.F.; Mota, L.T.; Toledo, M.J.O. Spatial Distribution of Intestinal Parasitic Infections in a Kaingáng Indigenous Village from Southern Brazil. Int. J. Environ. Health Res. 2016, 26, 578–588. [Google Scholar] [CrossRef]
- Itai, Y.; Fujino, T.; Ueno, K.; Motomatsu, Y. An Epidemiological Study of the Incidence of Abnormal Pregnancy in Areas Heavily Contaminated with Methylmercury. Environ. Sci. Int. J. Environ. Physiol. Toxicol. 2004, 11, 83–97. [Google Scholar]
- Benefice, E.; Luna-Monrroy, S.; Lopez-Rodriguez, R. Fishing Activity, Health Characteristics and Mercury Exposure of Amerindian Women Living alongside the Beni River (Amazonian Bolivia). Int. J. Hyg. Environ. Health 2010, 213, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Barreto, M.L.; Teixeira, M.G.; Bastos, F.I.; Ximenes, R.A.; Barata, R.B.; Rodrigues, L.C. Successes and Failures in the Control of Infectious Diseases in Brazil: Social and Environmental Context, Policies, Interventions, and Research Needs. Lancet 2011, 377, 1877–1889. [Google Scholar] [CrossRef]
- Boone, P.; Elbourne, D.; Fazzio, I.; Fernandes, S.; Frost, C.; Jayanty, C.; King, R.; Mann, V.; Piaggio, G.; Santos, A.d.; et al. Effects of Community Health Interventions on Under-5 Mortality in Rural Guinea-Bissau (EPICS): A Cluster-Randomised Controlled Trial. Lancet Glob. Health 2016, 4, e328–e335. [Google Scholar] [CrossRef] [Green Version]
- English, R.; Peer, N.; Honikman, S.; Tugendhaft, A.; Hofman, K.J. “First 1000 Days” Health Interventions in Low- and Middle-Income Countries: Alignment of South African Policies with High-Quality Evidence. Glob. Health Action 2017, 10, 1340396. [Google Scholar] [CrossRef] [Green Version]
- Villar, J.; Merialdi, M.; Gülmezoglu, A.M.; Abalos, E.; Carroli, G.; Kulier, R.; de Onis, M. Nutritional Interventions during Pregnancy for the Prevention or Treatment of Maternal Morbidity and Preterm Delivery: An Overview of Randomized Controlled Trials. J. Nutr. 2003, 133, 1606S–1625S. [Google Scholar] [CrossRef]
- World Health Organization Commitments in Brazil | Global Database on the Implementation of Nutrition Action (GINA). Available online: https://extranet.who.int/nutrition/gina/en/commitments/1394 (accessed on 16 August 2021).
- Saúde Indígena Specialist Doctors Assist Indigenous People of the Alto Rio Negro DSEI by Telemedicine. Available online: http://www.saudeindigena.net.br/coronavirus/en/viewNoticia.php?CodNot=4bafa5aea1 (accessed on 16 August 2021).



{kind=link}
{kind=link}
| Mothers to Infants ID | H-Hg (µg/g) | Age (Years) | Mother’s Hb (g/dL) | Mother’s BMI (kg/m2) | Infant ID | Sex | Age (months) | H-Hg (µg/g) | Hb (g/dL) | Height for Age (Z-Score) | Weight for Age (Z-Score) | Denver II Passed (Y/N)? |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Poxo Muybu | ||||||||||||
| PM-01-03-01 | 6.02 | 16 | 12.1 | 19.6 | PM-01-03-01-01 | M | 9 | 2.25 | 12.2 | −1.43 | −0.22 | Y |
| PM-03-01-02 | 6.08 | 45 | 11.9 | 26.3 | PM-03-01-02-05 | F | 20 | 2.97 | 12.1 | −2.02 | −1.68 | Y |
| PM-05-03-01 | 5.91 | 22 | 14.6 | 24.0 | PM-05-03-01-02 | M | 8 | 2.35 | 10.3 | 0.68 | 1.75 | Y |
| PM-06-01-02 | 7.12 | 31 | 12.5 | 29.2 | PM-06-01-02-03 | M | 21 | 2.22 | 11.1 | −3.28 | −2.71 | Y |
| PM-13-02-02 | 9.20 | 19 | 12.4 | 19.0 | PM-13-02-02-02 | F | 5 | 3.88 | - | −0.41 | 0.38 | Y |
| Sawré Aboy | ||||||||||||
| SA-01-01-02 | 10.1 | 19 | 11.4 | 19.6 | SA-01-01-02-02 | F | 5 | 5.36 | - | −0.62 | −0.63 | Y |
| SA-04-01-02 | 12.0 | 17 | 12.6 | 19.9 | SA-04-01-02-01 | F | 19 | 7.85 | 11.3 | −2.03 | −0.87 | Y |
| SA-06-01-02 | 13.8 | 19 | 14.4 | 24.4 | SA-06-01-02-01 | M | 21 | 6.12 | 11.3 | −1.23 | −0.91 | Y |
| SA-06-01-02-02 | F | 5 | 4.84 | - | 0.57 | −0.41 | Y | |||||
| SA-07-02-02 | 7.25 | 19 | 11.9 | 20.4 | SA-07-02-02-02 | F | 21 | 2.59 | 10.7 | −0.95 | −0.18 | N |
| Sawré Muybu | ||||||||||||
| SM-01-02-02 | 12.1 | 23 | 13.8 | 21.4 | SM-01-02-02-04 | M | 9 | 3.28 | 10.4 | −1.10 | −1.85 | Y |
| SM-04-03-02 | 4.10 | 18 | 13.4 | 26.3 | SM-04-03-02-03 | F | 7 | - | 9.80 | −2.81 | −1.95 | Y |
| SM-12-01-02 | 6.18 | 16 | 11.1 | 25.6 | SM-12-01-02-01 | F | 11 | 19.6 | 10.7 | −1.37 | −0.45 | N |
| SM-14-01-02 | 2.44 | 24 | 13.4 | 25.8 | SM-14-01-02-04 | M | 7 | 5.78 | 9.40 | −0.18 | −0.18 | Y |
| SM-15-01-02 | 4.31 | 16 | 12.8 | 24.2 | SM-15-01-02-02 | F | 9 | 2.44 | 12.0 | 0.15 | 0.91 | N |
| SM-20-01-02 | 3.34 | 29 | 15.3 | 23.6 | SM-20-01-02-05 | F | 5 | 3.98 | −1.16 | −1.23 | Y |
| Methylmercury Levels | ||
|---|---|---|
| <6.0 μg/g | ≥6.0 μg/g | |
| [MeHg]-Mean (μg/g) | 4.1 (n = 20) | 9.9 (n = 33) |
| Age Group (years) | ||
| 12–18 (n) | 9 | 12 |
| 19–30 (n) | 9 | 13 |
| 30–49 (n) | 2 | 8 |
| Sociodemographic Characteristics | ||
| Salary Mean (US$) | 281 | 217 |
| Education Level (median schooling years) | 6 | 6 |
| Household (n) | 11 | 8 |
| Agriculture (n) | 3 | 11 |
| Student, Teacher (n) | 5 | 6 |
| Partner working as extractivist (n) | 0 | 5 |
| Dietary Characteristics | ||
| Frequently Fruit Intake (n) | 20 | 33 |
| Weekly fish consumption (Median) | 3 | 3 |
| Nuts consumed in the wet season (n): | ||
| Daily | 10 | 19 |
| Weekly | 7 | 5 |
| Monthly | 1 | 8 |
| Health Outcomes and Obstetrician History | ||
| Hb Median (g/dL) | 13.4 | 13.2 |
| BMI (kg/m2) | 23.2 | 22.8 |
| Depressed mood (n) | 8 | 8 |
| Live Births (n) | 53 | 97 |
| Miscarriages (n) | 1 | 5 |
| Infant deaths (n) | 5 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kempton, J.W.; Périssé, A.R.S.; Hofer, C.B.; de Vasconcellos, A.C.S.; de Sousa Viana, P.V.; de Oliveira Lima, M.; de Jesus, I.M.; de Souza Hacon, S.; Basta, P.C. An Assessment of Health Outcomes and Methylmercury Exposure in Munduruku Indigenous Women of Childbearing Age and Their Children under 2 Years Old. Int. J. Environ. Res. Public Health 2021, 18, 10091. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910091
Kempton JW, Périssé ARS, Hofer CB, de Vasconcellos ACS, de Sousa Viana PV, de Oliveira Lima M, de Jesus IM, de Souza Hacon S, Basta PC. An Assessment of Health Outcomes and Methylmercury Exposure in Munduruku Indigenous Women of Childbearing Age and Their Children under 2 Years Old. International Journal of Environmental Research and Public Health. 2021; 18(19):10091. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910091
Chicago/Turabian StyleKempton, Joeseph William, André Reynaldo Santos Périssé, Cristina Barroso Hofer, Ana Claudia Santiago de Vasconcellos, Paulo Victor de Sousa Viana, Marcelo de Oliveira Lima, Iracina Maura de Jesus, Sandra de Souza Hacon, and Paulo Cesar Basta. 2021. "An Assessment of Health Outcomes and Methylmercury Exposure in Munduruku Indigenous Women of Childbearing Age and Their Children under 2 Years Old" International Journal of Environmental Research and Public Health 18, no. 19: 10091. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910091