
Enhancing Public Participation in Public Health Offerings: Patient Preferences for Facilities in the Western Cape Province Using a Discrete Choice Experiment

 ,
,
Abstract
:1. Introduction
2. Methods
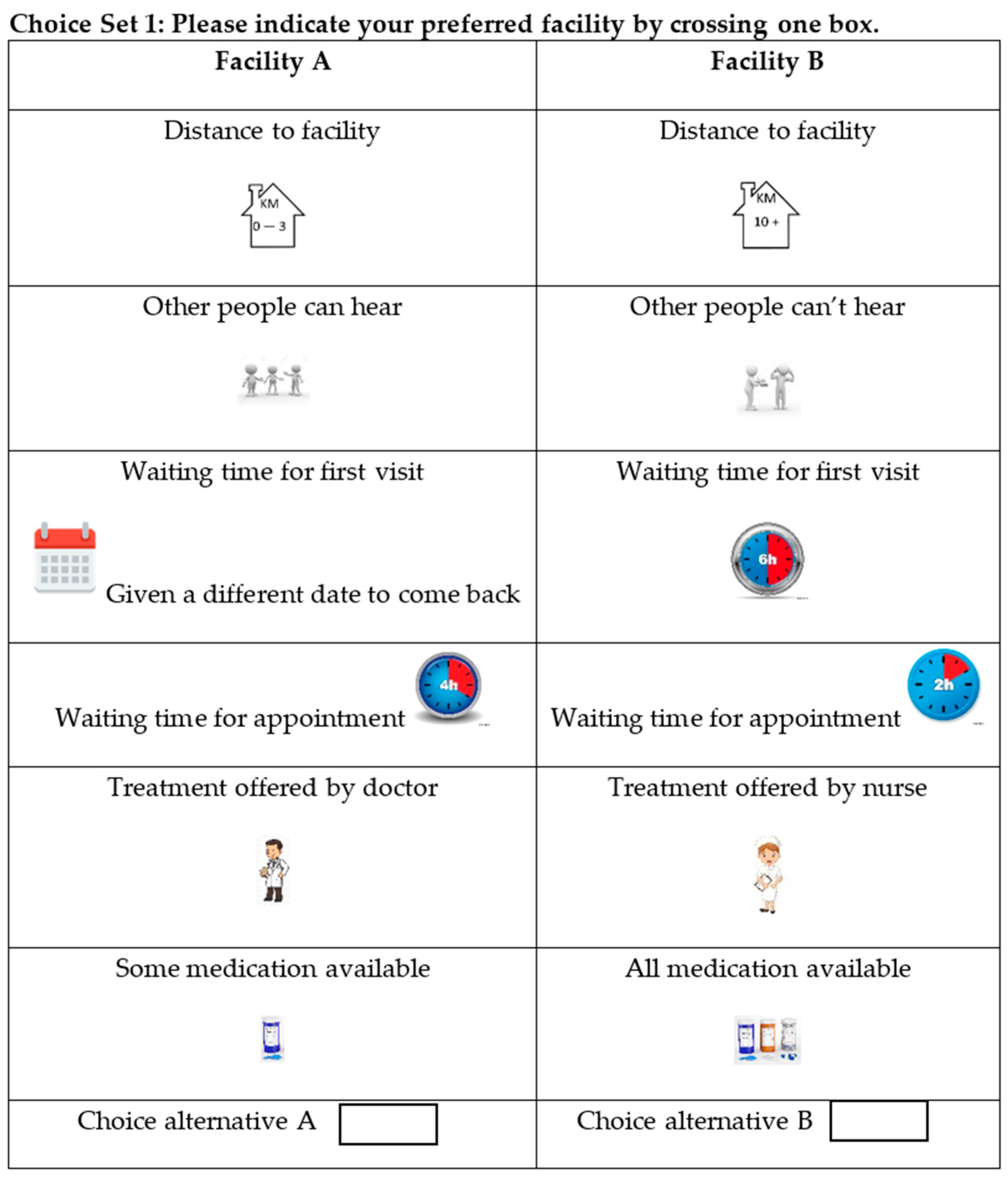
2.1. Discrete Choice Experiments
2.2. Study Design and Sampling
Selection of Attributes and Attribute Levels
2.3. Questionnaire Design and Sample Size
2.4. Setting and Participants
3. Analysis
4. Ethical Considerations
5. Results
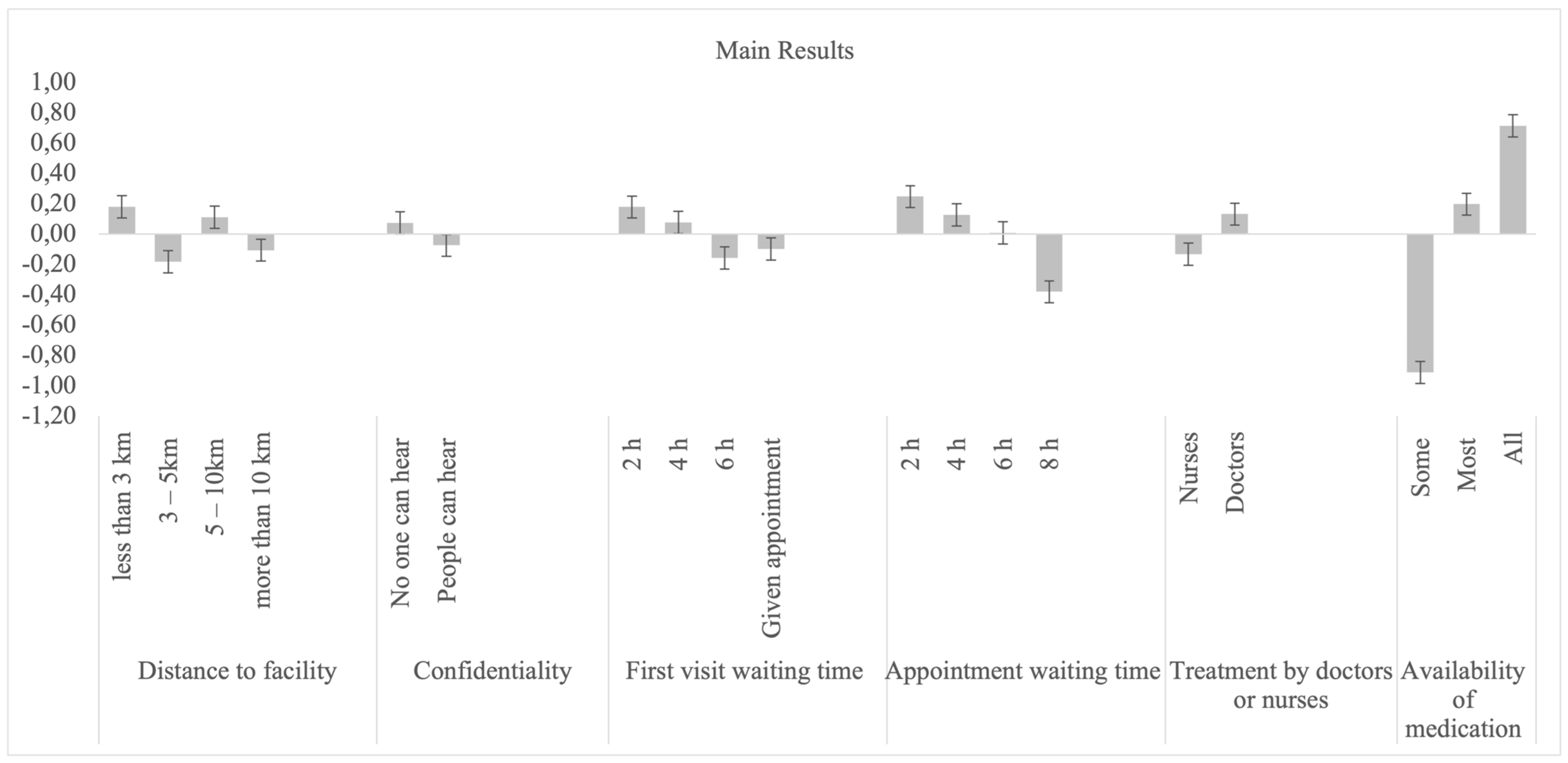
6. Patient Preferences
7. Sub-Group Analysis
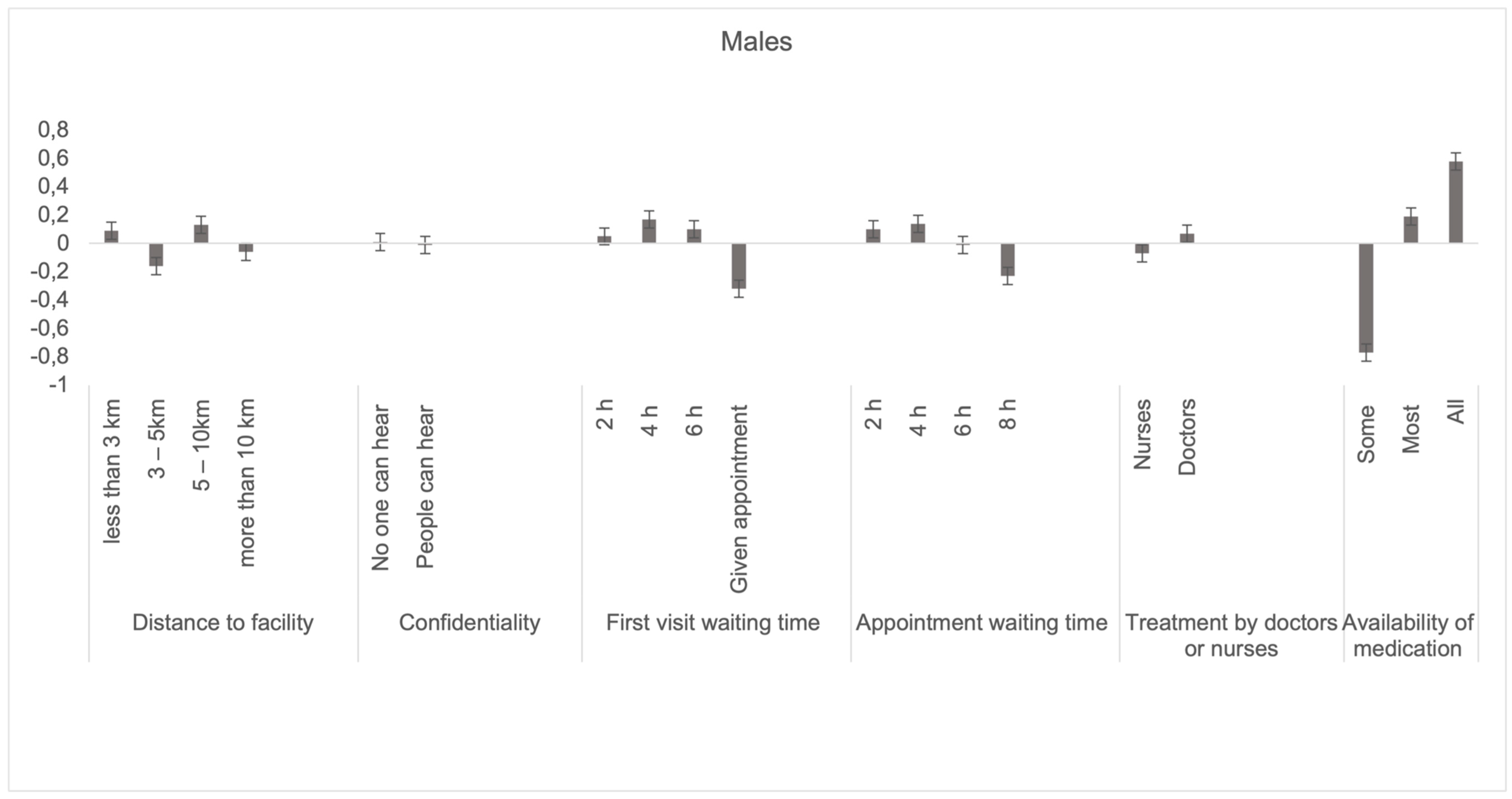
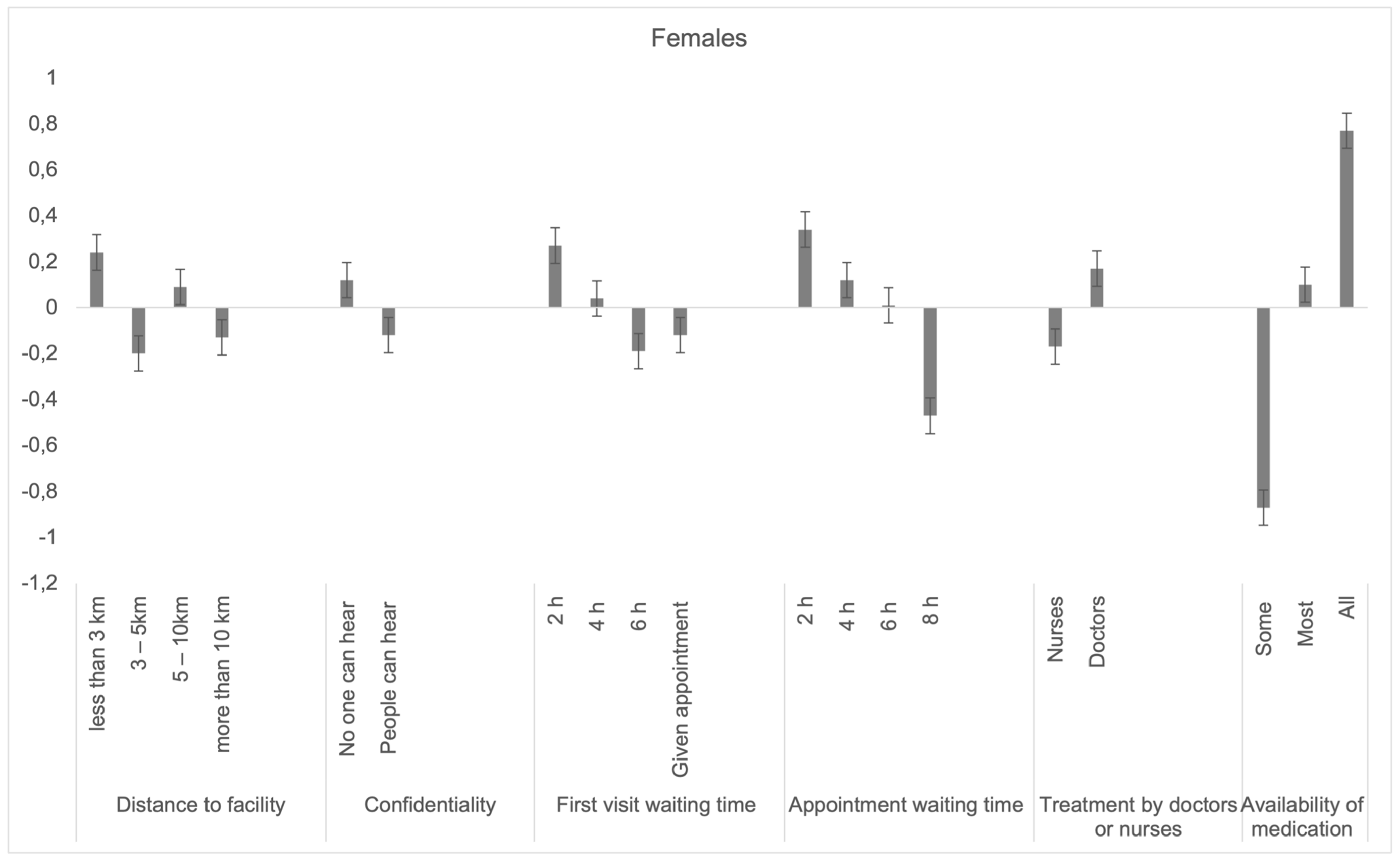
7.1. Males vs. Females
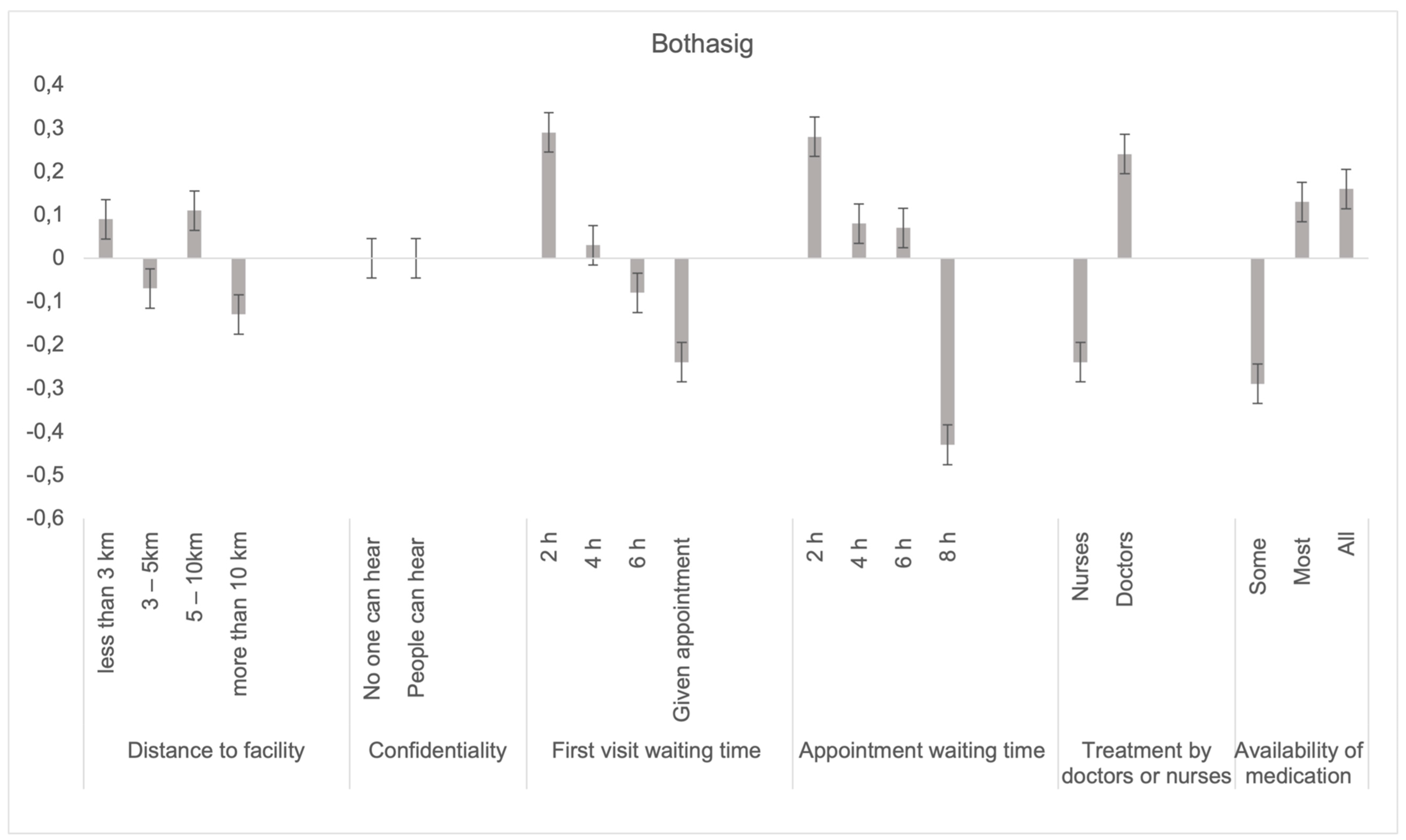
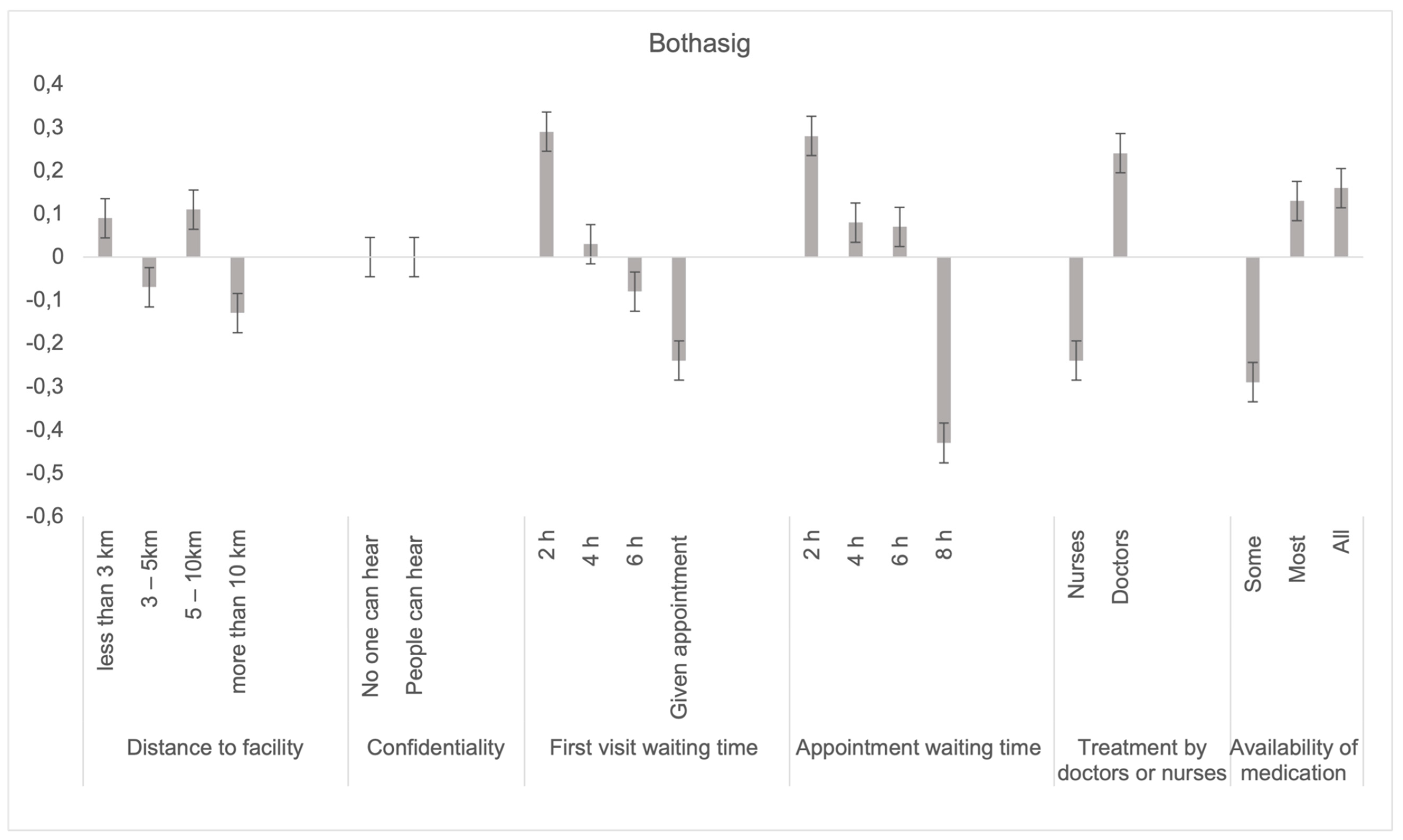
7.2. Facilities: Goodwood vs. Bothasig
8. Discussion
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 466) | Facility | Gender | Age | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Bothasig CDC (n = 230) | Goodwood CDC (n = 236) | p-Value | Women (n = 282) | Men (n = 179) | p-Value | 18–34 (n = 192) | 35+ (n = 274) | p-Value | ||
| Sex (%) | / | / | / | |||||||
| 179 (38.4) | 81 (35.2) | 98 (41.5) | 0.024 | / | / | 62 (32.3) | 117 (42.7) | 0.003 | |
| 282 (60.5) | 149 (64.8) | 133 (56.4) | 125 (65.1) | 157 (57.3) | |||||
| Age group (%) | ||||||||||
| 192 (41.2) | 114 (49.6) | 78 (33.1) | <0.001 | 125 (44.3) | 62 (34.6) | 0.003 | / | / | / |
| 274 (58.8) | 116 (50.4) | 158 (66.9) | 157 (55.7) | 117 (65.4) | / | / | |||
| Marital status (%) | ||||||||||
| 164 (35.2) | 82 (35.7) | 82 (34.7) | 0.931 | 99 (35.1) | 65 (36.3) | <0.001 | 111 (57.8) | 53 (19.3) | <0.001 |
| 214 (45.9) | 106 (46.1) | 108 (45.8) | 123 (43.6) | 91 (50.8) | 64 (33.3) | 150 (54.7) | |||
| 28 (6.0) | 13 (5.7) | 15 (6.4) | 24 (8.5) | 4 (2.2) | 2 (1.0) | 26 (9.5) | |||
| 46 (9.9) | 22 (9.6) | 24 (10.2) | 32 (11.3) | 14 (7.8) | 5 (2.6) | 41 (15.0) | |||
| 6 (1.3) | 4 (1.7) | 2 (0.8) | 3 (1.1) | 3 (1.7) | 3 (1.6) | 3 (1.1) | |||
| Education (%) | ||||||||||
| 32 (6.9) | 12 (5.2) | 20 (8.5) | 0.022 | 21 (7.4) | 11 (6.1) | <0.001 | 3 (1.6) | 29 (10.6) | <0.001 |
| 296 (63.5) | 137 (59.6) | 159 (67.4) | 191 (67.7) | 105 (58.7) | 120 (62.5) | 176 (64.2) | |||
| 80 (17.2) | 52 (22.6) | 28 (11.9) | 39 (13.8) | 41 (22.9) | 40 (20.8) | 40 (14.6) | |||
| 43 (9.2) | 24 (10.4) | 19 (8.1) | 26 (9.2) | 17 (9.5) | 20 (10.4) | 23 (8.4) | |||
| 8 (1.7) | 3 (1.3) | 5 (2.1) | 3 (1.1) | 5 (2.8) | 3 (1.6) | 5 (1.8) | |||
| Employment (%) | ||||||||||
| 34 (7.3) | 17 (7.4) | 17 (7.2) | 0.034 | 24 (8.5) | 10 (5.6) | <0.001 | 33 (17.2) | 1 (0.4) | <0.001 |
| 205 (44.0) | 86 (37.4) | 119 (50.4) | 136 (48.2) | 69 (38.5) | 52 (27.1) | 153 (55.8) | |||
| 53 (11.4) | 31 (13.5) | 22 (9.3) | 21 (7.4) | 32 (17.9) | 16 (8.3) | 37 (13.5) | |||
| 165 (35.4) | 93 (40.4) | 72 (30.5) | 98 (34.8) | 67 (37.4) | 85 (44.3) | 80 (29.2) | |||
Appendix B
| Access-Related Variables | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | All (n = 466) | Facility | Gender | Age | ||||||
| Bothasig CDC (n = 230) | Goodwood CDC (n = 236) | p-Value | Women (n = 282) | Men (n = 179) | p-Value | 18–34 (n = 192) | 35+ (n = 274) | p-Value | ||
| Facility visit | ||||||||||
| 54 (11.6) | 37 (16.1) | 17 (7.2) | <0.001 | 26 (9.2) | 28 (15.6) | 0.161 | 31 (16.1) | 23 (8.4) | <0.001 |
| 120 (25.8) | 77 (33.5) | 43 (18.2) | 75 (26.6) | 45 (25.1) | 68 (35.4) | 52 (19.0) | |||
| 74 (15.9) | 48 (20.9) | 26 (11.0) | 43 (15.2) | 31 (17.3) | 29 (15.1) | 45 (16.4) | |||
| 208 (44.6) | 65 (28.3) | 143 (60.6) | 134 (47.5) | 74 (41.3) | 58 (30.2) | 150 (54.7) | |||
| Chronic | ||||||||||
| 203 (43.6) | 89 (38.7) | 114 (48.3) | 0.097 | 120 (42.6) | 83 (46.4) | 0.073 | 44 (22.9) | 159 (58.0) | <0.001 |
| 236 (50.6) | 127 (55.2) | 109 (46.2) | 151 (53.5) | 85 (47.5) | 135 (70.3) | 101 (36.9) | |||
| 10 (2.1) | 4 (1.7) | 6 (2.5) | 3 (1.1) | 7 (3.9) | 1 (0.5) | 9 (3.3) | |||
| Transport | ||||||||||
| 186 (39.9) | 58 (25.2) | 128 (54.2) | <0.001 | 105 (37.2) | 81 (45.3) | 0.283 | 74 (38.5) | 112 (40.9) | 0.249 |
| 72 (15.5) | 31 (13.5) | 41 (17.4) | 52 (18.4) | 20 (11.2) | 37 (19.3) | 35 (12.8) | |||
| 12 (2.6) | 7 (3.0) | 5 (2.1) | 8 (2.8) | 4 (2.2) | 5 (2.6) | 7 (2.6) | |||
| 16 (3.4) | 12 (5.2) | 4 (1.7) | 10 (3.5) | 6 (3.4) | 7 (3.6) | 9 (3.3) | |||
| 170 (36.5) | 119 (51.7) | 51 (21.6) | 104 (36.9) | 66 (36.9) | 61 (31.8) | 109 (39.7) | |||
| 1 (0.2) | 1 (0.4) | 0 (0.00) | 1 (0.4) | 0 (0.00) | 1 (0.5) | 0 (0.00) | |||
| Travel time | ||||||||||
| 246 (52.8) | 128 (55.7) | 118 (50.0) | 0.208 | 154 (54.6) | 92 (51.4) | 0.645 | 101 (52.6) | 145 (52.9) | 0.905 |
| 140 (30.0) | 66 (28.7) | 74 (31.4) | 85 (30.1) | 55 (30.7) | 55 (28.6) | 85 (31.0) | |||
| 51 (10.9) | 19 (8.3) | 32 (13.6) | 30 (10.6) | 21 (11.7) | 19 (9.9) | 32 (11.7) | |||
| 11 (2.4) | 7 (3.0) | 4 (1.7) | 8 (2.8) | 3 (1.7) | 4 (2.1) | 7 (2.6) | |||
Appendix C


Appendix D


References
- Yu, W.; Li, M.; Ye, F.; Xue, C.; Zhang, L. Patient preference and choice of healthcare providers in Shanghai, China: A cross-sectional study. BMJ Open 2017, 7, e016418. [Google Scholar] [CrossRef] [Green Version]
- Cheng, B.; Li, X.; Lu, Y.; Tan, Y. Agent-based Modeling and Simulation Research into Residents Healthcare Choice. Syst. Eng. 2009, 27, 96–101. [Google Scholar]
- Mahlathi, P.; Dlamini, J. Minimum data sets for human resources for health and the surgical workforce in South Africa’s health system: A rapid analysis of stock and migration. Afr. Inst. Heal. Leadersh. Dev. 2015. Available online: https://www.who.int/workforcealliance/031616south_africa_case_studiesweb.pdf (accessed on 12 November 2021).
- World Health Organization The World Health Report 2000–Health Systems: Improving Performance; World Health Organization: Geneva, Switzerland, 2000; Volume 78.
- Honda, A.; Ryan, M.; Van Niekerk, R.; McIntyre, D. Improving the public health sector in South Africa: Eliciting public preferences using a discrete choice experiment. Health Policy Plan. 2015, 30, 600–611. [Google Scholar] [CrossRef] [Green Version]
- Dear South Africa Call for Public Comment on NHI Bill. Available online: https://dearsouthafrica.co.za/national-health-insurance-bill-2019/ (accessed on 12 November 2021).
- Parlimentary Communication Services Media Alert: Committee on Health To Continue Public Hearings on Nhi Bill. Available online: https://www.parliament.gov.za/press-releases/media-alert-committee-health-continue-public-hearings-nhi-bill. (accessed on 12 November 2021).
- Isaacs, J. Critical Assessment of Public Participation in Enhancing Governance in South Africa: A Case Study of Selected Community Health Committees in Cape Town, Mitchell’s Plain. 2016. Available online: https://www.academia.edu/38335759/Critical_Assessment_of_Public_Participation_in_Enhancing_Governance_in_South_Africa_A_Case_Study_of_Selected_Community_Health_Committees_in_Cape_Town_Mitchells (accessed on 12 November 2021).
- House, I.; Street, K. Mid-Year Population Estimates 2017; Statistics South Africa: Pretoria, South Africa, 2017. [Google Scholar]
- Loewenson, R. Public Participation in Health: Making People Matter. IDS Working. Paper 84 1998, IDS Collections 1451. Available online: https://opendocs.ids.ac.uk/opendocs/handle/20.500.12413/3402 (accessed on 12 November 2021).
- Gray, A.; Vawda, Y. Health policy and legislation. S. Afr. Heal. Rev. 2014, 2014, 3–19. [Google Scholar]
- Hifinger, M.; Hiligsmann, M.; Ramiro, S.; Watson, V.; Severens, J.L.; Fautre, B.; Uhlig, T.; Van Vollenhoven, R.; Jacques, P.; Detert, J.; et al. Economic considerations and patients’ preferences affect treatment selection for patients with rheumatoid arthritis: A discrete choice experiment among European rheumatologists. Ann. Rheum. Dis. 2017, 76, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Dirksen, C.D.; Utens, C.M.A.; Joore, M.A.; van Barneveld, T.A.; Boer, B.; Dreesens, D.H.H.; van Laarhoven, H.; Smit, C.; Stiggelbout, A.M.; van der Weijden, T. Integrating evidence on patient preferences in healthcare policy decisions: Protocol of the patient-VIP study. Implement. Sci. 2013, 8, 64–65. [Google Scholar] [CrossRef] [Green Version]
- Say, R.E.; Thomson, R. The importance of patient preferences in treatment decisions—challenges for doctors. BMJ 2003, 327, 542–545. [Google Scholar] [CrossRef]
- Salampessy, B.H.; Veldwijk, J.; Jantine Schuit, A.; van den Brekel-Dijkstra, K.; Neslo, R.E.J.; Ardine de Wit, G.; Lambooij, M.S. The Predictive Value of Discrete Choice Experiments in Public Health: An Exploratory Application. Patient 2015, 8, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Mulhbacher, A.C.; Bethge, S. Patients’ preferences: A Discrete Choice Experiment for treatment of non-small-cell lung cancer. Eur. J. Heal. Econ. 2015, 16, 657–670. [Google Scholar] [CrossRef] [Green Version]
- Brennan, P.F.; Strombom, I. Improving health care by understanding patient preferences: The role of computer technology. J. Am. Med. Informatics Assoc. 1998, 5, 257–262. [Google Scholar] [CrossRef] [Green Version]
- Brittin, J.; Elijah-Barnwell, S.; Nam, Y.; Araz, O.; Friedow, B.; Jameton, A.; Drummond, W.; Huang, T.T.K. Community-engaged public health research to inform hospital campus planning in a low socioeconomic status urban neighborhood. Heal. Environ. Res. Des. J. 2015, 8, 12–24. [Google Scholar] [CrossRef] [Green Version]
- Rifkin, S.B. Examining the links between community participation and health outcomes: A review of the literature. Health Policy Plan. 2014, 29, 98–106. [Google Scholar] [CrossRef]
- Abelson, J.; Montesanti, S.; Li, K.; Gauvin, F.-P.; Martin, E. Effective Strategies for Interactive Public Engagement in the Development of Healthcare Policies and Programs; Canadian Health Services Research Foundation: Ottawa, ON, Canada, 2010. [Google Scholar]
- Coulter, A.; Ellins, J. Effectiveness of strategies for informing, educating, and involving patients. Br. Med. J. 2007, 335, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Contandriopoulos, D. A sociological perspective on public participation in health care. Soc. Sci. Med. 2004, 58, 321–330. [Google Scholar] [CrossRef]
- Conklin, A.; Morris, Z.; Nolte, E. Involving the Public in Healthcare Policy; RAND Corporation: Santa Monica, CA, USA, 2010. [Google Scholar]
- Soekhai, V.; Whichello, C.; Levitan, B.; Veldwijk, J.; Pinto, C.A.; Donkers, B.; Huys, I.; van Overbeeke, E.; Juhaeri, J.; de Bekker-Grob, E.W. Methods for exploring and eliciting patient preferences in the medical product lifecycle: A literature review. Drug Discov. Today 2019, 24, 1324–1331. [Google Scholar] [CrossRef]
- Republic of South Africa National Department of Health. National Department of Health–National Core Standards; The Republic of South Africa: Pretoria, South Africa, 2011.
- Kleij, K.S.; Tangermann, U.; Amelung, V.E.; Krauth, C. Patients’ preferences for primary health care–A systematic literature review of discrete choice experiments. BMC Health Serv. Res. 2017, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Jiang, M.Z.; Fu, Q.; Xiong, J.Y.; Li, X.L.; Jia, E.P.; Peng, Y.Y.; Shen, X. Preferences heterogeneity of health care utilization of community residents in China: A stated preference discrete choice experiment. BMC Health Serv. Res. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Jia, E.; Gu, Y.; Peng, Y.; Li, X.; Shen, X.; Jiang, M.; Xiong, J. Preferences of patients with non-communicable diseases for primary healthcare facilities: A discrete choice experiment in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 3987. [Google Scholar] [CrossRef]
- Zhang, W.; Ung, C.O.L.; Lin, G.; Liu, J.; Li, W.; Hu, H.; Xi, X. Factors contributing to patients’ preferences for primary health care institutions in China: A qualitative study. Front. Public Heal. 2020, 8, 414. [Google Scholar] [CrossRef]
- Zhang, Z.; Qiu, Z. The usage pattern and spatial preference of community facilities by elder people in rural environments. J. Hous. Built Environ. 2020, 35, 661–678. [Google Scholar] [CrossRef]
- Republic of South Africa National Department of Health. National Health Insurance Bill; The Republic of South Africa: Pretoria, South Africa, 2018; pp. 533–549.
- Bridges, J.F.P.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint analysis applications in health–A checklist: A report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Heal. 2011, 14, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Coast, J.; Al-Janabi, H.; Sutton, E.J.; Horrocks, S.A.; Vosper, A.J.; Swancutt, D.R.; Flynn, T.N. Using qualitative methods for attribute development for Discrete Choice Experiments: Issues and recommendations. Health Econ. 2012, 21, 730–741. [Google Scholar] [CrossRef]
- Chiwire, P.; Evers, S.M.; Mahomed, H.; Hiligsmann, M. Identification and Prioritization of Attributes for a Discrete Choice Experiment Using the Nominal Group Technique: Patients’ Choice of Public Health Facilities in Cape Town, South Africa. Value Health Reg. Issues 2021, 27, 90–98. [Google Scholar] [CrossRef]
- Chiwire, P.; Evers, S.M.; Mahomed, H.; Hiligsmann, M. Willingness to pay for primary health care at public facilities in the Western Cape Province, Cape Town, South Africa. J. Med. Econ. 2021, 24, 162–172. [Google Scholar] [CrossRef]
- Lancsar, E.; Louviere, J. Conducting Discrete Choice experiments to inform healthcare decision making: A user’s guide. Pharmacoeconomics 2008, 26, 661–677. [Google Scholar] [CrossRef]
- de Bekker-Grob, E.W.; Donkers, B.; Jonker, M.F.; Stolk, E.A. Sample size requirements for Discrete-Choice Experiments in healthcare: A practical guide. Patient 2015, 8, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, R. Studying Preferences in Health Service Delivery: The Use of Discrete Choice Experiments; Nossal Institute, Health Policy & Health finance Knowledge Hub: Melbourne, Australia, 2011. [Google Scholar]
- Hifinger, M.; Hiligsmann, M.; Ramiro, S.; Severens, H.; Fautrel, B.J.; Watson, V.; Uhlig, T.; van Vollenhoven, R.; Jacques, P.; Detert, J.; et al. OP0281 Rheumatologists Consider Patient Preferences and Costs when Choosing Treatments for Rheumatoid Arthritis (RA) Patients. A Cross-European Discrete Choice Experiment. Ann. Rheum. Dis. 2015, 74, 178.2–179. [Google Scholar] [CrossRef]
- Hiligsmann, M.M.; Bours, S.P.G.; Boonen, A. A Review of Patient Preferences for Osteoporosis Drug Treatment. Curr. Rheumatol. Rep. 2015, 17, 61. [Google Scholar] [CrossRef] [Green Version]
- Hiligsmann, M.; van Durme, C.; Geusens, P.; Dellaert, B.G.C.; Dirksen, C.D.; van der Weijden, T.; Reginster, J.Y.; Boonen, A. Nominal Group Technique to select attributes for Discrete Choice Experiments: An example for drug treatment choice in osteoporosis. Patient Prefer. Adherence 2013, 7, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Escamilla, V.; Calhoun, L.; Winston, J.; Speizer, I.S. The Role of Distance and Quality on Facility Selection for Maternal and Child Health Services in Urban Kenya. J. Urban Heal. 2018, 95, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Schoeps, A.; Gabrysch, S.; Niamba, L.; Sié, A.; Becher, H. The effect of distance to health-care facilities on childhood mortality in rural Burkina Faso. Am. J. Epidemiol. 2011, 173, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Jordan, H.; Roderick, P.; Martin, D.; Barnett, S. Distance, rurality and the need for care: Access to health services in South West England. Int. J. Health Geogr. 2004, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Nesbitt, R.C.; Lohela, T.J.; Soremekun, S.; Vesel, L.; Manu, A.; Okyere, E.; Grundy, C.; Amenga-Etego, S.; Owusu-Agyei, S.; Kirkwood, B.R.; et al. The influence of distance and quality of care on place of delivery in rural Ghana. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kadobera, D.; Sartorius, B.; Masanja, H.; Mathew, A.; Waiswa, P. The effect of distance to formal health facility on childhood mortality in rural Tanzania, 2005–2007. Glob. Health Action 2012, 5, 1–9. [Google Scholar] [CrossRef]
- Caldow, J.; Bond, C.; Ryan, M.; Campbell, N.C.; Miguel, F.S.; Kiger, A.; Lee, A. Treatment of minor illness in primary care: A national survey of patient satisfaction, attitudes and preferences regarding a wider nursing role. Heal. Expect. 2007, 10, 30–45. [Google Scholar] [CrossRef] [Green Version]
- Larson, E.; Vail, D.; Mbaruku, G.M.; Kimweri, A.; Freedman, L.P.; Kruk, M.E. Moving toward patient-centered care in Africa: A discrete choice experiment of preferences for delivery care among 3003 Tanzanian women. PLoS ONE 2015, 10, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, L.B.; Kjær, T.; Kragstrup, J.; Gyrd-Hansen, D. Do general practitioners know patients’ preferences? An empirical study on the agency relationship at an aggregate level using a discrete choice experiment. Value Heal. 2012, 15, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Hwang, B.; Shroufi, A.; Gils, T.; Steele, S.J.; Grimsrud, A.; Boulle, A.; Yawa, A.; Stevenson, S.; Jankelowitz, L.; Versteeg-Mojanaga, M.; et al. Stock-outs of antiretroviral and tuberculosis medicines in South Africa: A national cross-sectional survey. PLoS ONE 2019, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Republic of South Africa National Department of Health. National Policy on Management of Patient Waiting Time in Out Patient Departments; National Department of Health: Pretoria, South Africa, 2015; p. 20.
- Lancsar, E.; Swait, J. Reconceptualising the External Validity of Discrete Choice Experiments. Pharmacoeconomics 2014, 32, 951–965. [Google Scholar] [CrossRef]
- Quaife, M.; Terris-Prestholt, F.; Di Tanna, G.L.; Vickerman, P. How well do discrete choice experiments predict health choices? A systematic review and meta-analysis of external validity. Eur. J. Heal. Econ. 2018, 19, 1053–1066. [Google Scholar] [CrossRef] [Green Version]
- Hunter, J.R.; Asmall, S.; Ravhengani, N.M.; Chandran, T.M.; Tucker, J.; Mokgalagadi, Y. The Ideal Clinic in South Africa: Progress and challenges in implementation. S. Afr. Heal. Rev. 2016, 2017, 111–124. [Google Scholar]


| Attributes | Definition of Attributes | Attribute |
|---|---|---|
| Distance to CDC | How far for patients to travel to the community day center (CDC) in kilometers from their home. | Less than 3 km |
| Between 3–5 km | ||
| Between 5–10 km | ||
| More than 10 km | ||
| Confidentiality during treatment | Consultation is carried out behind closed doors, without other patients and staff hearing. | Other patients and staff cannot hear the consultation |
| Other patients and staff can hear the consultation | ||
| Waiting time for the first visit to the facility (without an appointment) | How long does it take to consult with the doctor or nurse after entering the CDC. If the first visit is for a particular ailment, they will give a diagnosis. | 2 h |
| 4 h | ||
| 6 h | ||
| Different day than the appointment | ||
| Waiting time with an appointment | How long does it take to see the doctor or nurse after entering the CDC with a pre-booked appointment? | 2 h |
| 4 h | ||
| 6 h | ||
| 8 h | ||
| Treatment offered by | Which staff member provides a diagnosis. | Doctor |
| Nurse | ||
| Availability of required medication | The patient receives the medication prescribed at the CDC. | All the required medication is available |
| Most of the required medication is available | ||
| Some of the required medication is available |
| Type of Factors | Variables | All (n = 466) | Facility | ||
|---|---|---|---|---|---|
| Bothasig CDC (n = 230) | Goodwood CDC (n = 236) | p-Value | |||
| Sociodemographic Factors | Sex (%) | ||||
| 179 (38.4) | 81 (35.2) | 98 (41.5) | 0.024 | |
| 282 (60.5) | 149 (64.8) | 133 (56.4) | ||
| Age Group (%) | |||||
| 192 (41.2) | 114 (49.6) | 78 (33.1) | <0.001 | |
| 274 (58.8) | 116 (50.4) | 158 (66.9) | ||
| Marital Status (%) | |||||
| 164 (35.2) | 82 (35.7) | 82 (34.7) | 0.931 | |
| 214 (45.9) | 106 (46.1) | 108 (45.8) | ||
| 28 (6.0) | 13 (5.7) | 15 (6.4) | ||
| 46 (9.9) | 22 (9.6) | 24 (10.2) | ||
| 6 (1.3) | 4 (1.7) | 2 (0.8) | ||
| Education (%) | |||||
| 32 (6.9) | 12 (5.2) | 20 (8.5) | 0.022 | |
| 296 (63.5) | 137 (59.6) | 159 (67.4) | ||
| 80 (17.2) | 52 (22.6) | 28 (11.9) | ||
| 43 (9.2) | 24 (10.4) | 19 (8.1) | ||
| 8 (1.7) | 3 (1.3) | 5 (2.1) | ||
| Employment (%) | |||||
| 34 (7.3) | 17 (7.4) | 17 (7.2) | 0.034 | |
| 205 (44.0) | 86 (37.4) | 119 (50.4) | ||
| 53 (11.4) | 31 (13.5) | 22 (9.3) | ||
| 165 (35.4) | 93 (40.4) | 72 (30.5) | ||
| Access-Related Factors | Facility Visit | ||||
| 54 (11.6) | 37 (16.1) | 17 (7.2) | <0.001 | |
| 120 (25.8) | 77 (33.5) | 43 (18.2) | ||
| 74 (15.9) | 48 (20.9) | 26 (11.0) | ||
| 208 (44.6) | 65 (28.3) | 143 (60.6) | ||
| Chronic | |||||
| 203 (43.6) | 89 (38.7) | 114 (48.3) | 0.097 | |
| 236 (50.6) | 127 (55.2) | 109 (46.2) | ||
| 10 (2.1) | 4 (1.7) | 6 (2.5) | ||
| Transport | |||||
| 186 (39.9) | 58 (25.2) | 128 (54.2) | <0.001 | |
| 72 (15.5) | 31 (13.5) | 41 (17.4) | ||
| 12 (2.6) | 7 (3.0) | 5 (2.1) | ||
| 16 (3.4) | 12 (5.2) | 4 (1.7) | ||
| 170 (36.5) | 119 (51.7) | 51 (21.6) | ||
| 1 (0.2) | 1 (0.4) | 0 (0.00) | ||
| Travel Time | |||||
| 246 (52.8) | 128 (55.7) | 118 (50.0) | 0.208 | |
| 140 (30.0) | 66 (28.7) | 74 (31.4) | ||
| 51 (10.9) | 19 (8.3) | 32 (13.6) | ||
| 11 (2.4) | 7 (3.0) | 4 (1.7) | ||
| Overall Results | Coefficient | Estimated Standard Deviation | Relative Importance |
|---|---|---|---|
| Attribute/Level | |||
| Constant (non-random parameter) | 0.07 ** (0.01 to 0.14) | ||
| Distance | |||
| 0.18 *** (0.67 to 0.29) | 0.23 *** | |
| −0.18 *** (−0.27 to −0.10) | 0.36 *** | |
| 0.11 *** (0.03 to 0.18) | 0.19 ** | |
| −0.11 ** (−0.21 to −0.01) | 6.7% | |
| Confidentiality | |||
| 0.07 *** (0.02 to 0.13) | 0.22 *** | |
| −0.07 (−0.13 to −0.02) | 4.6% | |
| First visit waiting time | |||
| 0.12 *** (0.08 to 0.27) | 0.20 ** | |
| 0.08 * (−0.00 to 0.16) | 0.30 *** | |
| −0.16 (−0.23 to −0.08) | 0.1 | |
| −0.10 (−0.22 to 0.02) | 10.4% | |
| Appointment waiting time | |||
| 0.25 *** (0.14 to 0.35) | 0.23 *** | |
| 0.13 *** (0.05 to 0.20) | 0.19 ** | |
| 0.01 (−0.07 to 0.09) | 0.01 | |
| −0.38 *** (−0.49 to −0.27) | 19.5% | |
| Treatment by doctors or nurses | |||
| −0.13 (−0.23 to −0.04) | ||
| 0.13*** (0.04 to 0.23) | 0.1 | 8.2% |
| Availability of medication | |||
| −0.91 *** (−1.10 to −0.72) | ||
| 0.20 (0.14 to 0.26) | ||
| 0.71 *** (0.55 to 0.88) | 0.97 *** | 50.5% |
| Replications for simulated probs. = 1000 | Log likelihood function −3618.69568 | McFadden pseudo R-squared 0.0528530 | |
| RPL model with panel has 466 groups | Restricted log likelihood −3820.62726 | Estimation based on n = 5512, K = 27 | |
| Fixed number of observations./group = 12 | Chi squared [27] (p = 0.000) 403.86315 | Inf.Cr.AIC = 7291.4 AIC/n = 1.323 | |
| Number of observations.= 5592, skipped 80 observations | Significance level 0.00000 |
| Sub-Group Gender | Male | Female | Interaction Gender | ||||
|---|---|---|---|---|---|---|---|
| Attribute/Level | Coefficient | Estimated Standard Deviation | Relative Importance | Coefficient | Estimated Standard Deviation | Relative Importance | Significance p-Value |
| Constant (non-random parameter) | 0.07 (−0.03 to 0.18) | 0.07 * (−0.01 to 0.16) | 0.15 | ||||
| Distance | |||||||
| 0.09 (−0.10 to 0.28) | 0.41 *** | 0.24 *** (0.10 to 0.39) | 0.15 | 0.18 | ||
| −0.16 ** (−0.29 to −0.02) | 0.35 *** | −0.20 *** (−0.30 to −0.9) | 0.36 *** | 0.67 | ||
| 0.13 ** (0.00 to 0.25) | 0.17 | 0.09 (−0.00 to 0.19) | 0.22 ** | 0.65 | ||
| −0.06 (−0.22 to 0.10) | 11.4% | −0.13 ** (−0.25 to −0.01) | 8% | |||
| Confidentiality | |||||||
| 0.01 (−0.07 to 0.09) | 0.18 *** | 0.12 *** (0.05 to 0.19) | 0.26 *** | 0.06 * | ||
| −0.01 (−0.09 to 0.07) | 0.8% | −0.12 (−0.19 to −0.05) | 6% | |||
| First visit waiting time | |||||||
| 0.05(−0.10 to 0.21) | 0.24 ** | 0.27 *** (0.14 to 0.39) | 0.20 * | 0.03 ** | ||
| 0.17 ** (0.03 to 0.30) | 0.34 *** | 0.04 (−0.06 to 0.14) | 0.25 *** | 0.15 | ||
| 0.10 (−0.22 to 0.02) | 0.11 | 0.19 *** (−0.09 to 0.11) | 0.11 | 0.23 | ||
| −0.32 ** (−0.53 to −0.11) | 14.6% | −0.12 (−0.28 to 0.04) | 12% | |||
| Appointment Waiting time | |||||||
| 0.10 (−0.63 to 0.27) | 0.21 | 0.34 *** (0.20 to 0.47) | 0.21 | 0.04 ** | ||
| 0.14 ** (0.02 to 0.27) | 0.34 *** | 0.12 ** (0.02 to 0.22) | 0.19 | 0.78 | ||
| −0.01 (0.14 to 0.12) | 0.13 | 0.01 (−0.09 to 0.11) | 0.00 | 0.88 | ||
| −0.23 ** (−0.41 to −0.05) | 14.6% | −0.47 *** (−0.61 to −0.33) | 21% | |||
| Treatment by doctors or nurses | |||||||
| −0.07 (−0.23 to 0.08) | −0.17 (−0.30 to −0.05) | |||||
| 0.07 (−0.08 to 0.23) | 0.13 | 5.5% | 0.17 *** (0.05 to 0.30) | 0.12 | 9% | 0.34 |
| Availability of medication | |||||||
| −0.77 (0.47 to 1.07) | −0.87 (0.62 to 1.12) | |||||
| 0.19 *** (0.10 to 0.29) | 0.23 *** | 0.10 *** (0.12 to 0.28) | 0.29 *** | 0.97 | ||
| 0.58 *** (0.32 to 0.84) | 0.98 *** | 53.1% | 0.77 *** (0.12 to 0.28) | 1.00 *** | 43% | 0.28 |
| Sub-Group Facilities | Goodwood | Bothasig | Interaction Facility | ||||
|---|---|---|---|---|---|---|---|
| Attribute/Level | Coefficient | Estimated Standard Deviation | Relative Importance | Coefficient | Estimated Standard Deviation | Relative Importance | Significance p-Value |
| Constant (non-random parameter) | 0.10 * (−0.00 to 0.19) | 0.06 (−0.03 to 0.15) | 0.17 | ||||
| Distance | |||||||
| 0.25 *** (0.82 to 0.42) | 0.17 | 0.09 (−0.07 to 0.25) | 0.32 *** | 0.18 | ||
| −0.29 *** (−0.43 to −0.53) | 0.63 *** | −0.07 (−0.18 to 0.04) | 0.01 | 0.01 *** | ||
| 0.12 ** (0.01 to 0.23) | 0.22 ** | 0.11 ** (0.00 to 0.22) | 0.21 ** | 0.98 | ||
| −0.08 (−0.23 to 0.07) | 11.3% | −0.13 * (−0.27 to 0.01) | 10% | |||
| Confidentiality | |||||||
| 0.16 *** (0.09 to 0.24) | 0.08 | 0.00 (−0.08 to 0.08) | 0.29 *** | 0.02 ** | ||
| −0.16 (−0.24 to −0.09) | 6.7% | 0.00 (−0.08 to 0.08) | - | |||
| First visit waiting time | |||||||
| 0.07 (−0.06 to 0.21) | 0.05 | 0.29 *** (0.15 to 0.44) | 0.35 *** | 0.02 ** | ||
| 0.11 * (−0.01 to 0.22) | 0.17 | 0.03 (−0.09 to 0.15) | 0.35 *** | 0.21 | ||
| −0.26 *** (−0.37 to −0.14) | 0.04 | −0.08 (−0.18 to 0.02) | 0.14 | 0.03 ** | ||
| 0.08 (−0.10 to 0.26) | 7.8% | −0.24 ** (−0.42 to −0.06) | 22% | |||
| Appointment Waiting time | |||||||
| 0.20 *** (0.05 to 0.36) | 0.33 *** | 11.8% | 0.28 *** (0.14 to 0.43) | 0.19 | 0.30 | |
| 0.21 *** (0.09 to 0.33) | 0.35 *** | 0.08 (−0.03 to 0.19) | 0.05 | 0.34 | ||
| −0.05 (−0.16 to 0.07) | 0.02 | 0.07 (−0.04 to 0.18) | 0.01 | 0.25 | ||
| −0.36 *** (−0.53 to −0.19) | −0.43 *** (−0.58 to −0.28) | 29% | ||||
| Treatment by doctors or nurses | |||||||
| −0.01 (−0.16 to 0.13) | −0.24 (−0.38 to −0.10) | |||||
| 0.01 (−0.13 to 0.16) | 0.00 | 0.4% | 0.24 *** (0.10 to 0.38) | 0.25 *** | 20% | 0.02 ** |
| Availability of medication | |||||||
| −1.62 (1.31 to 1.93) | −0.29 ** (0.06 to 0.52) | |||||
| 0.29 *** (0.20 to 0.39) | 0.34 *** | 0.13 *** (0.04 to 0.21) | 0.23 *** | 0.03 ** | ||
| 1.33 *** (1.06 to 1.61) | 1.14 *** | 62.0% | 0.16 (−0.04 to 0.36) | 0.65 *** | 19% | 0.00 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiwire, P.; Beaudart, C.; Evers, S.M.; Mahomed, H.; Hiligsmann, M. Enhancing Public Participation in Public Health Offerings: Patient Preferences for Facilities in the Western Cape Province Using a Discrete Choice Experiment. Int. J. Environ. Res. Public Health 2022, 19, 590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010590
Chiwire P, Beaudart C, Evers SM, Mahomed H, Hiligsmann M. Enhancing Public Participation in Public Health Offerings: Patient Preferences for Facilities in the Western Cape Province Using a Discrete Choice Experiment. International Journal of Environmental Research and Public Health. 2022; 19(1):590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010590
Chicago/Turabian StyleChiwire, Plaxcedes, Charlotte Beaudart, Silvia M. Evers, Hassan Mahomed, and Mickaël Hiligsmann. 2022. "Enhancing Public Participation in Public Health Offerings: Patient Preferences for Facilities in the Western Cape Province Using a Discrete Choice Experiment" International Journal of Environmental Research and Public Health 19, no. 1: 590. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010590