
Exclusive Breastfeeding at Discharge in Regional New South Wales, Australia: The Role of Antenatal Care (2011–2020)

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
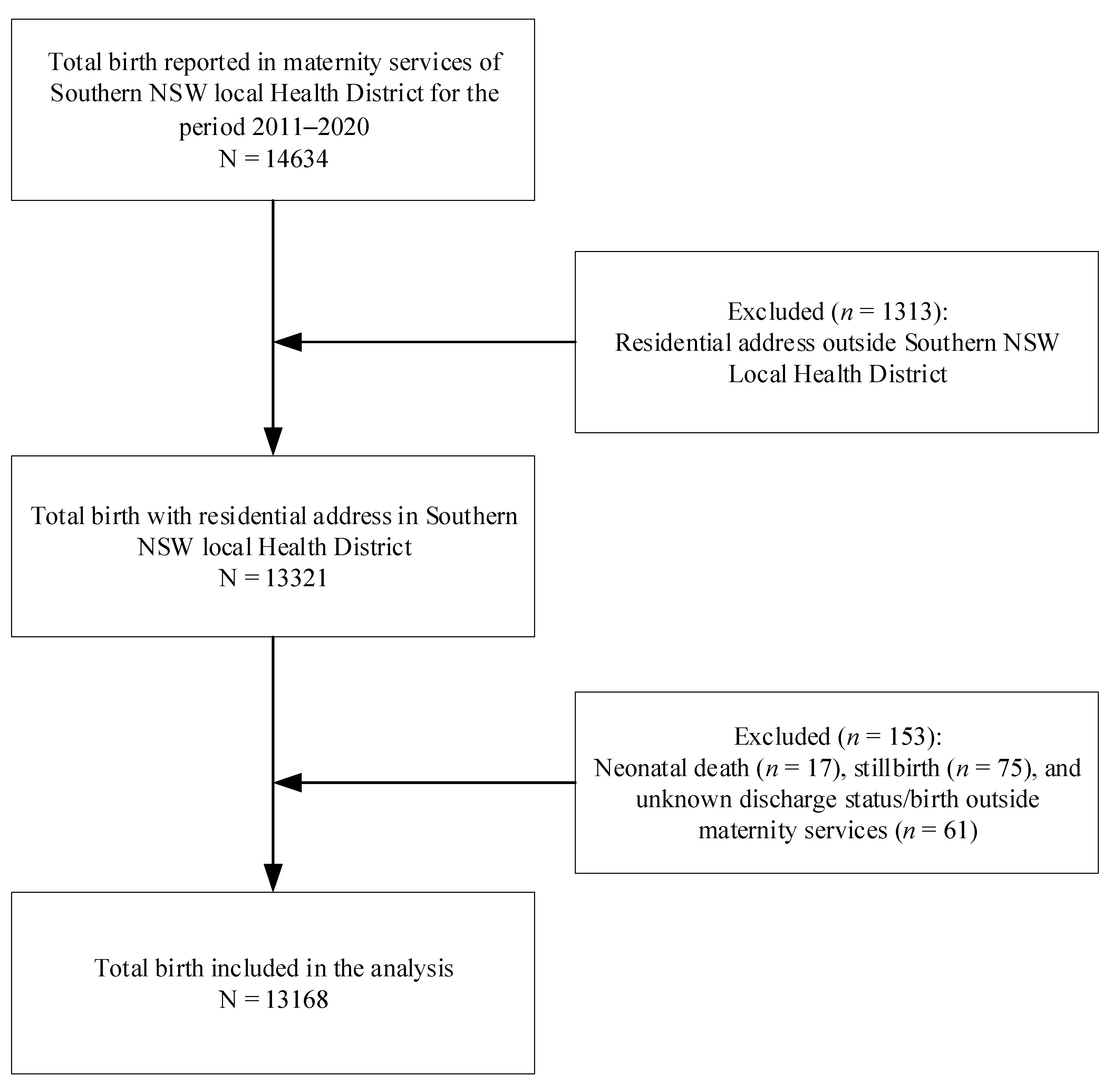
2.1. Data Source and Sample Composition
2.2. Outcome Variable
2.3. Exposure Variables
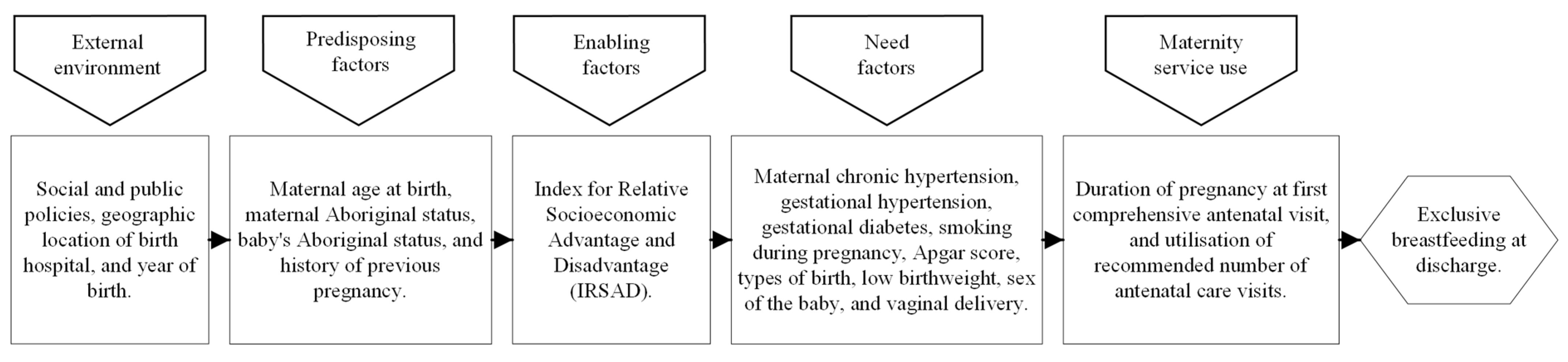
2.4. Covariates
2.5. Statistical Analysis
2.6. Ethical Consideration
3. Results
3.1. Characteristics of Study Sample
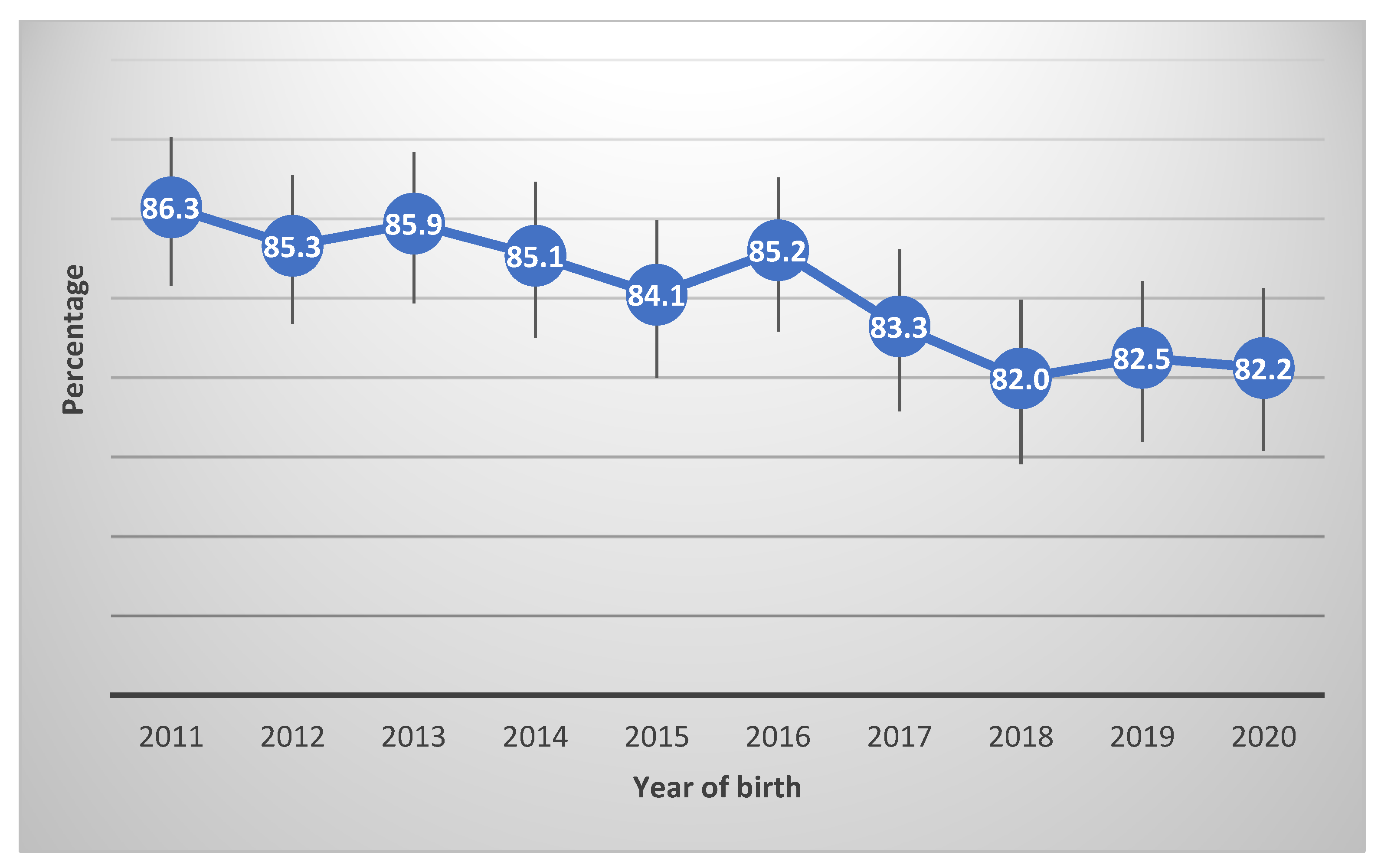
3.2. Exclusive Breastfeeding at Discharge Rate
3.3. Antenatal Care and Exclusive Breastfeeding at Discharge
3.4. Factors Associated with Exclusive Breastfeeding at Discharge
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amir, L.H.; Donath, S.M. Socioeconomic status and rates of breastfeeding in Australia: Evidence from three recent national health surveys. Med. J. Aust. 2008, 189, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics (ABS) Regional Population by Age and Sex. Available online: https://www.abs.gov.au/statistics/people/population/regional-population-age-and-sex/ (accessed on 23 May 2023).
- Indigenous Women’s Maternal Health and Maternal Mortality. Available online: https://www.unwomen.org/en/digital-library/publications/2018/4/indigenous-womens-maternal-health-and-maternal-mortality (accessed on 23 May 2023).
- Australia’s Mothers and Babies. Available online: https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-babies-data-visualisations/contents/summary (accessed on 1 March 2023).
- Pregnancy Care Guidelines. Available online: https://www.health.gov.au/resources/pregnancy-care-guidelines (accessed on 1 March 2023).
- Breastfeeding in NSW—Promotion, Protection and Support. Available online: https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2018_034.pdf (accessed on 1 March 2023).
- Antenatal Care during COVID-19. Available online: https://www.aihw.gov.au/reports/mothers-babies/antenatal-care-during-covid-19/contents/antenatal-care-and-covid-19 (accessed on 12 September 2022).
- Chmielewska, B.; Barratt, I.; Townsend, R.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e759–e772. [Google Scholar] [CrossRef] [PubMed]
- Balogun, O.O.; O’Sullivan, E.J.; McFadden, A.; Ota, E.; Gavine, A.; Garner, C.D.; Renfrew, M.J.; MacGillivray, S. Interventions for promoting the initiation of breastfeeding. Cochrane Database Syst. Rev. 2016, 11, CD001688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shofiya, D.; Sumarmi, S.; Ahmed, F. Nutritional status, family income and early breastfeeding initiation as determinants to successful exclusive breastfeeding. J. Public Health Res. 2020, 9, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Meedya, S.; Fernandez, R.; Fahy, K. Effect of educational and support interventions on long-term breastfeeding rates in primiparous women: A systematic review and meta-analysis. JBI Evid. Synth. 2017, 15, 2307–2332. [Google Scholar] [CrossRef] [PubMed]
- Gallegos, D.; Parkinson, J.; Duane, S.; Domegan, C.; Jansen, E.; Russell-Bennett, R. Understanding breastfeeding behaviours: A cross-sectional analysis of associated factors in Ireland, the United Kingdom and Australia. Int. Breastfeed. J. 2020, 15, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Hadisuyatmana, S.; Has, E.M.; Sebayang, S.K.; Efendi, F.; Astutik, E.; Kuswanto, H.; Arizona, I.K. Women’s empowerment and determinants of early initiation of breastfeeding: A scoping review. J. Pediatr. Nurs. 2021, 56, e77–e92. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.A.; Binns, C.W.; Graham, K.I.; Oddy, W.H. Temporal changes in the determinants of breastfeeding initiation. Birth 2006, 33, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Manohar, N.; Hayen, A.; Bhole, S.; Eastwood, J.; Levy, S.; Scott, J.A. Determinants of breastfeeding initiation among mothers in Sydney, Australia: Findings from a birth cohort study. Int. Breastfeed. J. 2017, 12, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, J.; Cooklin, A.R.; Smith, J. Which mothers wean their babies prematurely from full breastfeeding? An Australian cohort study. Acta Paediatr. 2009, 98, 1274–1277. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, P.R.; Buck, G.; Jackson, J.; Woolley, E.; Bowman, R.; Fox, L.; Gallagher, S.; Sorrell, M.; Dubois, L. Impact of Antenatal Care on Perinatal Outcomes in New South Wales, Australia: A Decade-Long Regional Perspective. Int. J. Environ. Res. Public Health 2023, 20, 977. [Google Scholar] [CrossRef] [PubMed]
- Socio-Economic Indexes for Areas. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/allprimarymainfeatures/8C5F5BB699A0921CCA258259000BA619?opendocument (accessed on 5 September 2022).
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandall, J.; Soltani, H.; Gates, S.; Shennan, A.; Devane, D. Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database Syst. Rev. 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, M.; Dietsch, E. The feasibility of caseload midwifery in rural Australia: A literature review. Women Birth 2013, 26, e1–e4. [Google Scholar] [CrossRef]
- Kashani, A.; Ingberg, J.L.; Hildingsson, I. Caseload midwifery in a rural Australian setting: A qualitative descriptive study. Eur. J. Midwifery 2021, 5, 1–9. [Google Scholar] [CrossRef]
- Williams, K.; Lago, L.; Lainchbury, A.; Eagar, K. Mothers’ views of caseload midwifery and the value of continuity of care at an Australian regional hospital. Midwifery 2010, 26, 615–621. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Factors | Study Sample | Exclusive Breastfeeding at Discharge | |
|---|---|---|---|
| Covariates | N (% ϕ) | n | % (95% CI) |
| Geographic location of birth hospital | |||
| Cooma Health Service | 1479 (11.2) | 1241 | 83.9 (81.9, 85.7) |
| Goulburn Base Hospital | 2904 (22.1) | 2298 | 79.1 (77.6, 80.6) |
| Moruya District Hospital | 2813 (21.4) | 2433 | 86.5 (85.2, 87.7) |
| Queanbeyan Health Service | 3624 (27.5) | 3182 | 87.8 (86.7, 88.8) |
| South East Regional Hospital | 2348 (17.8) | 1931 | 82.2 (80.6, 83.7) |
| Maternal age at birth | |||
| <20 years | 582 (4.4) | 429 | 73.7 (70.0, 77.1) |
| 20–34 years | 10,416 (79.1) | 8831 | 84.8 (84.1, 85.5) |
| 35+ years | 2170 (16.5) | 1825 | 84.1 (82.5, 85.6) |
| Maternal Aboriginal status (N = 13,131) | |||
| Non-Aboriginal | 12,291 (93.3) | 10,419 | 84.8 (84.1, 85.4) |
| Aboriginal | 840 (6.4) | 636 | 75.7 (72.7, 78.5) |
| Baby’s Aboriginal status (N = 12,944) | |||
| Non-Aboriginal | 11,803 (89.6) | 10,002 | 84.7 (84.1, 85.4) |
| Aboriginal | 1141 (8.7) | 890 | 78.0 (75.5, 80.3 |
| History of previous pregnancy (N = 13,152) | |||
| Yes | 8000 (60.8) | 6760 | 84.5 (83.7, 85.3) |
| No | 5152 (39.1) | 4311 | 83.7 (82.6, 84.7) |
| IRSAD quintile (N = 13,154) | |||
| First (most socially advantaged) | 1584 (12.0) | 1401 | 88.4 (86.8, 89.9) |
| Second | 864 (6.6) | 763 | 88.3 (86.0, 90.3) |
| Third | 2512 (19.1) | 2166 | 86.2 (84.8, 87.5) |
| Fourth | 5029 (38.2) | 4239 | 84.3 (83.3, 85.3) |
| Fifth (most socially disadvantaged) | 3165 (24.0) | 2505 | 79.1 (77.7, 80.5) |
| Chronic hypertension | |||
| No | 13,059 (99.2) | 10,997 | 84.2 (83.6, 84.8) |
| Yes | 109 (0.8) | 88 | 80.7 (72.2, 87.1) |
| Gestational hypertension | |||
| No | 12,775 (97.0) | 10,784 | 84.4 (83.8, 85.0) |
| Yes | 393 (3.0) | 301 | 76.6 (72.1, 80.5) |
| Gestational diabetes (N = 13,147) | |||
| No | 12,348 (93.8) | 10,413 | 84.3 (83.7, 85.0) |
| Yes | 799 (6.0) | 654 | 81.9 (79.0, 84.4) |
| Smoking during pregnancy (N = 13,130) | |||
| Smoker during the second half of pregnancy | 1951 (14.8) | 1415 | 72.5 (70.5, 74.5) |
| Smoker in the first half of pregnancy but quit in the second half | 385 (2.9) | 297 | 77.1 (72.7, 81.1) |
| Non-smoker | 10,794 (82.0) | 9342 | 86.5 (85.9, 87.2) |
| Apgar 5 min score (N = 13,068) | |||
| Apgar ≥ 7 | 12,887 (97.9) | 10,889 | 84.5 (83.9, 85.1) |
| Apgar < 7 | 181(1.4) | 111 | 61.3 (54.0, 68.1) |
| Types of birth | |||
| Singleton | 13,066 (99.2) | 11,041 | 84.5 (83.9, 85.1) |
| Twin | 102 (0.8) | 44 | 43.1 (33.9, 52.9) |
| Low birthweight (<2500 g) | |||
| No | 12,788 (97.0) | 10,862 | 84.9 (84.3, 85.5) |
| Yes | 380 (3.0) | 223 | 58.7 (53.7, 63.5) |
| Sex of the baby (N = 13,166) | |||
| Male | 6771 (51.4) | 5665 | 83.7 (82.8, 84.5) |
| Female | 6395 (48.6) | 5419 | 84.7 (83.8, 85.6) |
| Vaginal delivery | |||
| Yes | 9620 (73.1) | 8289 | 86.2 (85.5, 86.8) |
| No | 3548 (26.9) | 2796 | 78.8 (77.4, 80.1) |
| Exposure variables | |||
| Utilisation of recommended number of ANC visits | |||
| Yes | 11,114 (84.4) | 9439 | 84.9 (84.3, 85.6) |
| No | 2054 (15.6) | 1646 | 80.1 (78.4, 81.8) |
| Duration of pregnancy at first comprehensive antenatal visit (N = 13,120) | |||
| First trimester | 6198 (47.1) | 5225 | 84.3 (83.4, 85.2) |
| Second trimester | 5921 (45.0) | 5010 | 84.6 (87.6, 85.5) |
| Third trimester | 1001 (7.6) | 818 | 81.7 (79.2, 84.0) |
| Total | 13,168 (100) | 11,085 | 84.2 (83.5, 84.8) |
| Crude | Adjusted £ | |||
|---|---|---|---|---|
| Exposure Variables | OR | (95% CI) | n | % (95% CI) |
| Utilisation of recommended number of antenatal care visits | ||||
| Yes | Reference | Reference | ||
| No | 0.72 | (0.63, 0.81) ** | 0.85 | (0.75, 0.97) * |
| Duration of pregnancy at first comprehensive antenatal visit | ||||
| First trimester | Reference | Reference | ||
| Second trimester | 1.02 | (0.93, 1.13) | 0.93 | (0.84, 1.04) |
| Third trimester | 0.79 | (0.67, 0.94) * | 0.82 | (0.68, 0.99) * |
| Covariates | Crude | Adjusted £ | ||
|---|---|---|---|---|
| OR | (95% CI) | n | % (95% CI) | |
| Year of birth | ||||
| 2011 | Reference | Reference | ||
| 2012 | 0.92 | (0.74, 1.15) | 0.98 | (0.77, 1.23) |
| 2013 | 0.97 | (0.77, 1.21) | 0.95 | (0.75, 1.21) |
| 2014 | 0.91 | (0.73, 1.13) | 0.91 | (0.72, 1.15) |
| 2015 | 0.84 | (0.68, 1.04) | 0.84 | (0.67, 1.06) |
| 2016 | 0.92 | (0.73, 1.14) | 0.90 | (0.71, 1.14) |
| 2017 | 0.79 | (0.64, 0.98) * | 0.72 | (0.57, 0.90) * |
| 2018 | 0.72 | (0.59, 0.89) * | 0.68 | (0.54, 0.85) * |
| 2019 | 0.75 | (0.61, 0.92) * | 0.71 | (0.56, 0.89) * |
| 2020 | 0.74 | (0.60, 0.91) * | 0.68 | (0.54, 0.85) * |
| Geographic location of birth hospital | ||||
| Cooma Health Service | Reference | Reference | ||
| Goulburn Base Hospital | 0.73 | (0.62, 0.86) ** | 0.82 | (0.64, 1.06) |
| Moruya District Hospital | 1.23 | 1.23 (1.03, 1.46) * | 0.84 | (0.68, 1.04) |
| Queanbeyan Health Service | 1.38 | 1.38 (1.16, 1.64) ** | 1.48 | (1.15, 1.90) * |
| South East Regional Hospital | 0.89 | 0.89 (0.75, 1.06) | 0.93 | (0.71, 1.20) |
| Maternal age at birth | ||||
| 20–34 years | Reference | Reference | ||
| <20 years | 0.50 | (0.42, 0.61) ** | 0.60 | (0.48, 0.75) ** |
| 35+ years | 0.95 | (0.84, 1.08) | 0.93 | (0.81, 1.07) |
| Maternal Aboriginal status | ||||
| Non-Aboriginal | Reference | Reference | ||
| Aboriginal | 0.56 | (0.47, 0.66) ** | 0.72 | (0.60, 0.87) * |
| Baby’s Aboriginal status | ||||
| Non-Aboriginal | Reference | Reference | ||
| Aboriginal | 0.64 | (0.55, 0.74) | 0.78 | (0.66, 0.93) * |
| IRSAD quintile | ||||
| First (most socially advantaged) | Reference | Reference | ||
| Second | 0.99 | (0.76, 1.28) | 1.05 | (0.78, 1.43) |
| Third | 0.82 | (0.68, 0.99) * | 0.92 | (0.75, 1.13) |
| Fourth | 0.70 | (0.59, 0.83) ** | 0.74 | (0.56, 0.98) * |
| Fifth (most socially disadvantaged) | 0.50 | (0.42, 0.59) ** | 0.63 | (0.48, 0.82) * |
| Gestational hypertension | ||||
| No | Reference | Reference | ||
| Yes | 0.60 | (0.48, 0.77) ** | 0.60 | (0.47, 0.77) ** |
| Smoking during pregnancy | ||||
| Smoker at the end of pregnancy | Reference | Reference | ||
| Smoker in the first half of pregnancy but quit in the second half | 1.28 | (0.99, 1.65) | 1.21 | (0.92, 1.58) |
| Non-smoker | 2.44 | (2.18, 2.73) ** | 2.08 | (1.83, 2.37) ** |
| Apgar 5 min score | ||||
| Apgar ≥ 7 | Reference | Reference | ||
| Apgar < 7 | 0.29 | (0.21, 0.39) ** | 0.35 | (0.25, 0.49) ** |
| Types of birth | ||||
| Singletons | Reference | Reference | ||
| Twin | 0.14 | (0.09, 0.21) ** | 0.23 | (0.15, 0.36) ** |
| Low birthweight (<2500 g) | ||||
| No | Reference | Reference | ||
| Yes | 0.25 | (0.20, 0.31) ** | 0.46 | (0.36, 0.59) ** |
| Vaginal delivery | ||||
| Yes | Reference | Reference | ||
| No | 0.60 | (0.54, 0.66) ** | 0.59 | (0.53, 0.66) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woolley, E.; Buck, G.; Jackson, J.; Bowman, R.; Fox, L.; Gallagher, S.; Sorrell, M.; Ghimire, P.R. Exclusive Breastfeeding at Discharge in Regional New South Wales, Australia: The Role of Antenatal Care (2011–2020). Int. J. Environ. Res. Public Health 2023, 20, 6135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20126135
Woolley E, Buck G, Jackson J, Bowman R, Fox L, Gallagher S, Sorrell M, Ghimire PR. Exclusive Breastfeeding at Discharge in Regional New South Wales, Australia: The Role of Antenatal Care (2011–2020). International Journal of Environmental Research and Public Health. 2023; 20(12):6135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20126135
Chicago/Turabian StyleWoolley, Emma, Gretchen Buck, Jackie Jackson, Rebekah Bowman, Louise Fox, Shirlena Gallagher, Malindey Sorrell, and Pramesh Raj Ghimire. 2023. "Exclusive Breastfeeding at Discharge in Regional New South Wales, Australia: The Role of Antenatal Care (2011–2020)" International Journal of Environmental Research and Public Health 20, no. 12: 6135. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20126135