
Volume-Independent Sodium Toxicity in Peritoneal Dialysis: New Insights from Bench to Bed

 ,
,  , and
, and 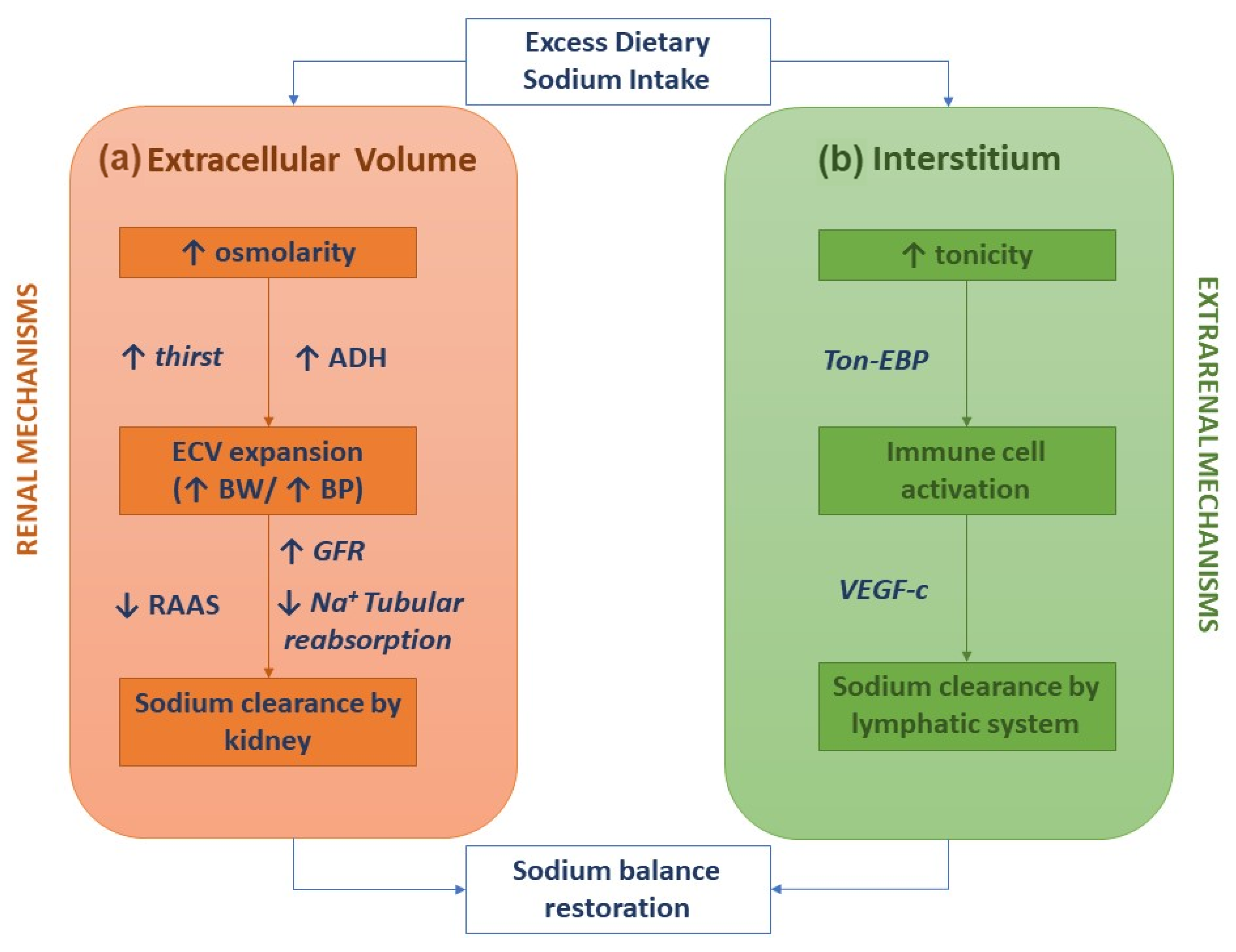{kind=link}
Abstract
:1. Introduction
2. Extrarenal Mechanisms for Sodium Body Balance and Hypertension
3. Volume-Independent Sodium Toxicity in End-Stage Kidney Disease
Sodium Removal by Peritoneal Dialysis
4. Alternative Strategies to Remove Sodium by Peritoneal Dialysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rose, B.D. Regulation of Water and Electrolyte Balance, 4th ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Borrelli, S.; Provenzano, M.; Gagliardi, I.; Michael, A.; Liberti, M.E.; De Nicola, L.; Conte, G.; Garofalo, C.; Andreucci, M. Sodium Intake and Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 4744. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Moissl, U.; Chazot, C.; Mallamaci, F.; Tripepi, G.; Arkossy, O.; Wabel, P.; Stuard, S. Chronic Fluid Overload and Mortality in ESRD. J. Am. Soc. Nephrol. 2017, 28, 2491–2497. [Google Scholar] [CrossRef] [Green Version]
- Titze, J.; Dahlmann, A.; Lerchl, K.; Kopp, C.; Rakova, N.; Schröder, A.; Luft, F.C. Spooky sodium balance. Kidney Int. 2014, 85, 759–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrelli, S.; La Milia, V.; De Nicola, L.; Cabiddu, G.; Russo, R.; Provenzano, M.; Minutolo, R.; Conte, G.; Garofalo, C. Sodium removal by peritoneal dialysis: A systematic review and meta-analysis. J. Nephrol. 2019, 32, 231–239. [Google Scholar] [CrossRef]
- Heer, M.; Baisch, F.; Kropp, J.; Gerzer, R.; Drummer, C. High dietary sodium chloride consumption may not induce body fluid retention in humans. Am. J. Physiol. Renal Physiol. 2000, 278, F585–F595. [Google Scholar] [CrossRef] [Green Version]
- Rakova, N.; Jüttner, K.; Dahlmann, A.; Schröder, A.; Linz, P.; Kopp, C.; Rauh, M.; Goller, U.; Beck, L.; Agureev, A.; et al. Long-term space flight simulation reveals infradian rhythmicity in human Na(+) balance. Cell Metab. 2013, 17, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Mattson, D.L. Immune mechanisms of salt-sensitive hypertension and renal end-organ damage. Nat. Rev. Nephrol. 2019, 15, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Machnik, A.; Neuhofer, W.; Jantsch, J.; Dahlmann, A.; Tammela, T.; Machura, K.; Park, J.K.; Beck, F.X.; Müller, D.N.; Derer, W.; et al. Macrophages regulate salt-dependent volume and blood pressure by a vascular endothelial growth factor-C-dependent buffering mechanism. Nat. Med. 2009, 15, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Machnik, A.; Dahlmann, A.; Kopp, C.; Goss, J.; Wagner, H.; van Rooijen, N.; Eckardt, K.U.; Müller, D.N.; Park, J.K.; Luft, F.C.; et al. Mononuclear phagocyte system depletion blocks interstitial tonicity-responsive enhancer binding protein/vascular endothelial growth factor C expression and induces salt-sensitive hypertension in rats. Hypertension 2010, 55, 755–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiig, H.; Schröder, A.; Neuhofer, W.; Jantsch, J.; Kopp, C.; Karlsen, T.V.; Boschmann, M.; Goss, J.; Bry, M.; Rakova, N.; et al. Immune cells control skin lymphatic electrolyte homeostasis and blood pressure. J. Clin. Investig. 2013, 123, 2803–2815. [Google Scholar] [CrossRef]
- Mattson, D.L.; Dasinger, J.H.; Abais-Battad, J.M. Amplification of Salt-Sensitive Hypertension and Kidney Damage by Immune Mechanisms. Am. J. Hypertens. 2021, 34, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Elijovich, F.; Kleyman, T.R.; Laffer, C.L.; Kirabo, A. Immune Mechanisms of Dietary Salt-Induced Hypertension and Kidney Disease: Harry Goldblatt Award for Early Career Investigators 2020. Hypertension 2021, 78, 252–260. [Google Scholar] [CrossRef]
- Elijovich, F.; Laffer, C.L.; Sahinoz, M.; Pitzer, A.; Ferguson, J.F.; Kirabo, A. The Gut Microbiome, Inflammation, and Salt-Sensitive Hypertension. Curr. Hypertens. Rep. 2020, 22, 79. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.F.; Aden, L.A.; Barbaro, N.R.; Van Beusecum, J.P.; Xiao, L.; Simmons, A.J.; Warden, C.; Pasic, L.; Himmel, L.E.; Washington, M.K.; et al. High dietary salt-induced dendritic cell activation underlies microbial dysbiosis-associated hypertension. JCI Insight 2019, 5, e126241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrelli, S.; De Nicola, L.; Minutolo, R.; Perna, A.; Provenzano, M.; Argentino, G.; Cabiddu, G.; Russo, R.; La Milia, V.; De Stefano, T.; et al. Sodium toxicity in peritoneal dialysis: Mechanisms and “solutions”. J. Nephrol. 2020, 33, 59–68. [Google Scholar] [CrossRef]
- Van Biesen, W.; Verger, C.; Heaf, J.; Vrtovsnik, F.; Britto, Z.M.L.; Do, J.Y.; Prieto-Velasco, M.; Martínez, J.P.; Crepaldi, C.; De Los Ríos, T.; et al. Evolution Over Time of Volume Status and PD-Related Practice Patterns in an Incident Peritoneal Dialysis Cohort. Clin. J. Am. Soc. Nephrol. 2019, 14, 882–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, C.; Verger, C.; Crepaldi, C.; Pham, J.; De Los Ríos, T.; Gauly, A.; Wabel, P.; Van Biesen, W. Baseline hydration status in incident peritoneal dialysis patients: The initiative of patient outcomes in dialysis (IPOD-PD study). Nephrol. Dial. Transplant. 2015, 30, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Paniagua, R.; Ventura, M.D.; Avila-Díaz, M.; Hinojosa-Heredia, H.; Méndez-Durán, A.; Cueto-Manzano, A.; Cisneros, A.; Ramos, A.; Madonia-Juseino, C.; Belio-Caro, F.; et al. NT-proBNP, fluid volume overload and dialysis modality are independent predictors of mortality in ESRD patients. Nephrol. Dial. Transplant. 2010, 25, 551–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Lone, E.L.; Visser, A.; Finney, H.; Fan, S.L. Clinical significance of multi-frequency bioimpedance spectroscopy in peritoneal dialysis patients: Independent predictor of patient survival. Nephrol. Dial. Transplant. 2014, 29, 1430–1437. [Google Scholar] [CrossRef] [Green Version]
- Kopp, C.; Linz, P.; Dahlmann, A.; Hammon, M.; Jantsch, J.; Müller, D.N.; Schmieder, R.E.; Cavallaro, A.; Eckardt, K.U.; Uder, M.; et al. 23Na magnetic resonance imaging-determined tissue sodium in healthy subjects and hypertensive patients. Hypertension 2013, 61, 635–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, M.P.; Raff, U.; Kopp, C.; Scheppach, J.B.; Toncar, S.; Wanner, C.; Schlieper, G.; Saritas, T.; Floege, J.; Schmid, M.; et al. Skin Sodium Concentration Correlates with Left Ventricular Hypertrophy in CKD. J. Am. Soc. Nephrol. 2017, 28, 1867–1876. [Google Scholar] [CrossRef]
- Qirjazi, E.; Salerno, F.R.; Akbari, A.; Hur, L.; Penny, J.; Scholl, T.; McIntyre, C.W. Tissue sodium concentrations in chronic kidney disease and dialysis patients by lower leg sodium-23 magnetic resonance imaging. Nephrol. Dial. Transplant. 2020. [Google Scholar] [CrossRef]
- Sahinoz, M.; Tintara, S.; Deger, S.M.; Alsouqi, A.; Crescenzi, R.L.; Mambungu, C.; Vincz, A.; Mason, O.; Prigmore, H.L.; Guide, A.; et al. Tissue sodium stores in peritoneal dialysis and hemodialysis patients determined by 23-sodium magnetic resonance imaging. Nephrol. Dial. Transplant. 2020, 36, 1307–1317. [Google Scholar] [CrossRef]
- Kopp, C.; Linz, P.; Maier, C.; Wabel, P.; Hammon, M.; Nagel, A.M.; Rosenhauer, D.; Horn, S.; Uder, M.; Luft, F.C.; et al. Elevated tissue sodium deposition in patients with type 2 diabetes on hemodialysis detected by 23Na magnetic resonance imaging. Kidney Int. 2018, 93, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Sakata, F.; Ishii, T.; Tawada, M.; Suzuki, Y.; Kinashi, H.; Katsuno, T.; Takei, Y.; Maruyama, S.; Mizuno, M.; et al. Excessive salt intake increases peritoneal solute transport rate via local tonicity-responsive enhancer binding protein in subtotal nephrectomized mice. Nephrol. Dial. Transplant. 2019, 34, 2031–2042. [Google Scholar] [CrossRef] [PubMed]
- Pletinck, A.; Consoli, C.; Van Landschoot, M.; Steppan, S.; Topley, N.; Passlick-Deetjen, J.; Vanholder, R.; Van Biesen, W. Salt intake induces epithelial-to-mesenchymal transition of the peritoneal membrane in rats. Nephrol. Dial. Transplant. 2010, 25, 1688–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, T.; Sakata, F.; Ishii, T.; Tawada, M.; Suzuki, Y.; Kinashi, H.; Katsuno, T.; Takei, Y.; Maruyama, S.; Mizuno, M.; et al. Sodium chloride promotes tissue inflammation via osmotic stimuli in subtotal-nephrectomized mice. Lab. Investig. 2017, 97, 432–446. [Google Scholar] [CrossRef]
- Dahlmann, A.; Dörfelt, K.; Eicher, F.; Linz, P.; Kopp, C.; Mössinger, I.; Horn, S.; Büschges-Seraphin, B.; Wabel, P.; Hammon, M.; et al. Magnetic resonance-determined sodium removal from tissue stores in hemodialysis patients. Kidney Int. 2015, 87, 434–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemoine, S.; Salerno, F.R.; Akbari, A.; McIntyre, C.W. Influence of Dialysate Sodium Prescription on Skin and Muscle Sodium Concentration. Am. J. Kidney Dis. 2021, 78, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Dahlmann, A.; Linz, P.; Zucker, I.; Haag, V.; Jantsch, J.; Dienemann, T.; Nagel, A.M.; Neubert, P.; Rosenhauer, D.; Rauh, M.; et al. Reduction of Tissue Na+ Accumulation After Renal Transplantation. Kidney Int. Rep. 2021, 6, 2338–2347. [Google Scholar] [CrossRef]
- Wang, T.; Waniewski, J.; Heimbürger, O.; Werynski, A.; Lindholm, B. A quantitative analysis of sodium transport and removal during peritoneal dialysis. Kidney Int. 1997, 52, 1609–1616. [Google Scholar] [CrossRef] [Green Version]
- Leypoldt, J.K.; Charney, D.I.; Cheung, A.K.; Naprestek, C.L.; Akin, B.H.; Shockley, T.R. Ultrafiltration and solute kinetics using low sodium peritoneal dialysate. Kidney Int. 1995, 48, 1959–1966. [Google Scholar] [CrossRef] [Green Version]
- Imholz, A.L.; Koomen, G.C.; Struijk, D.G.; Arisz, L.; Krediet, R.T. Fluid and solute transport in CAPD patients using ultralow sodium dialysate. Kidney Int. 1994, 46, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, M.; Yokoyama, K.; Kubo, H.; Matsumoto, H.; Hasegawa, T.; Shigematsu, T.; Kawaguchi, Y.; Sakai, O. The effect of ultra-low sodium dialysate in CAPD. A kinetic and clinical analysis. Clin. Nephrol. 1996, 45, 188–193. [Google Scholar] [PubMed]
- Davies, S.; Carlsson, O.; Simonsen, O.; Johansson, A.C.; Venturoli, D.; Ledebo, I.; Wieslander, A.; Chan, C.; Rippe, B. The effects of low-sodium peritoneal dialysis fluids on blood pressure, thirst and volume status. Nephrol. Dial. Transplant. 2009, 24, 1609–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkowski, B.; Tam, P.; van der Sande, F.M.; Vychytil, A.; Schwenger, V.; Himmele, R.; Gauly, A. Low-Sodium Versus Standard-Sodium Peritoneal Dialysis Solution in Hypertensive Patients: A Randomized Controlled Trial. Am. J. Kidney Dis. 2016, 67, 753–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkowski, B.; Tam, P.; van der Sande, F.M.; Vychytil, A.; Schwenger, V.; Klein, G.; Himmele, R.; Gauly, A. Residual Renal Function and Effect of Low-Sodium Solution on Blood Pressure in Peritoneal Dialysis Patients. Perit. Dial. Int. 2019, 39, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.; Haraldsson, B.; Vrtovsnik, F.; Schwenger, V.; Fan, S.; Klein, A.; Atiye, S.; Gauly, A. Single-dwell treatment with a low-sodium solution in hypertensive peritoneal dialysis patients. Perit. Dial. Int. 2020, 40, 446–454. [Google Scholar] [CrossRef]
- Blake, P.G. Sodium Levels in Peritoneal Dialysis Solution: How Low Should We Go? Am. J. Kidney Dis. 2016, 67, 719–721. [Google Scholar] [CrossRef] [Green Version]
- Vecchi, L.; Bonomini, M.; Palumbo, R.; Arduini, A.; Borrelli, S. Mild sodium reduction in peritoneal dialysis solution improves hypertension in end stage kidney disease: A case-report study. BMC Nephrol. 2021, 22, 170. [Google Scholar] [CrossRef]
- Freida, P.; Wilkie, M.; Jenkins, S.; Dallas, F.; Issad, B. The contribution of combined crystalloid and colloid osmosis to fluid and sodium management in peritoneal dialysis. Kidney Int. 2008, 73 (Suppl. 108), S102–S111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonomini, M.; Pandolfi, A.; Di Liberato, L.; Di Silvestre, S.; Cnops, Y.; Di Tomo, P.; D’Arezzo, M.; Monaco, M.P.; Giardinelli, A.; Di Pietro, N.; et al. L-carnitine is an osmotic agent suitable for peritoneal dialysis. Kidney Int. 2011, 80, 645–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonomini, M.; Di Liberato, L.; Del Rosso, G.; Stingone, A.; Marinangeli, G.; Consoli, A.; Bertoli, S.; De Vecchi, A.; Bosi, E.; Russo, R.; et al. Effect of an L-carnitine-containing peritoneal dialysate on insulin sensitivity in patients treated with CAPD: A 4-month, prospective, multicenter randomized trial. Am. J. Kidney Dis. 2013, 62, 929–938. [Google Scholar] [CrossRef]
- Piccapane, F.; Bonomini, M.; Castellano, G.; Gerbino, A.; Carmosino, M.; Svelto, M.; Arduini, A.; Procino, G. A Novel Formulation of Glucose-Sparing Peritoneal Dialysis Solutions with l-Carnitine Improves Biocompatibility on Human Mesothelial Cells. Int. J. Mol. Sci. 2020, 22, 123. [Google Scholar] [CrossRef] [PubMed]
- Bonomini, M.; Masola, V.; Procino, G.; Zammit, V.; Divino-Filho, J.C.; Arduini, A.; Gambaro, G. How to Improve the Biocompatibility of Peritoneal Dialysis Solutions (without Jeopardizing the Patient’s Health). Int. J. Mol. Sci. 2021, 22, 7955. [Google Scholar] [CrossRef] [PubMed]
- Rago, C.; Lombardi, T.; Di Fulvio, G.; Di Liberato, L.; Arduini, A.; Divino-Filho, J.C.; Bonomini, M. A New Peritoneal Dialysis Solution Containing L-Carnitine and Xylitol for Patients on Continuous Ambulatory Peritoneal Dialysis: First Clinical Experience. Toxins 2021, 13, 174. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borrelli, S.; De Nicola, L.; De Gregorio, I.; Polese, L.; Pennino, L.; Elefante, C.; Carbone, A.; Rappa, T.; Minutolo, R.; Garofalo, C. Volume-Independent Sodium Toxicity in Peritoneal Dialysis: New Insights from Bench to Bed. Int. J. Mol. Sci. 2021, 22, 12804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222312804
Borrelli S, De Nicola L, De Gregorio I, Polese L, Pennino L, Elefante C, Carbone A, Rappa T, Minutolo R, Garofalo C. Volume-Independent Sodium Toxicity in Peritoneal Dialysis: New Insights from Bench to Bed. International Journal of Molecular Sciences. 2021; 22(23):12804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222312804
Chicago/Turabian StyleBorrelli, Silvio, Luca De Nicola, Ilaria De Gregorio, Lucio Polese, Luigi Pennino, Claudia Elefante, Alessandro Carbone, Tiziana Rappa, Roberto Minutolo, and Carlo Garofalo. 2021. "Volume-Independent Sodium Toxicity in Peritoneal Dialysis: New Insights from Bench to Bed" International Journal of Molecular Sciences 22, no. 23: 12804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222312804