
Extracellular Vesicles and Thrombogenicity in Atrial Fibrillation


1
Internal Medicine Department, State Medical University, Zaporozhye 69035, Ukraine
2
Internal Medicine Department, Medical Academy of Postgraduate Education, Zaporozhye 69096, Ukraine
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2022, 23(3), 1774; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031774
Submission received: 16 January 2022
/
Revised: 30 January 2022
/
Accepted: 2 February 2022
/
Published: 4 February 2022
(This article belongs to the Special Issue Thrombo-Inflammatory Extracellular Vesicles)
Abstract
:Extracellular vesicles (EVs) are defined as a heterogenic group of lipid bilayer vesicular structures with a size in the range of 30–4000 nm that are released by all types of cultured cells. EVs derived from platelets, mononuclears, endothelial cells, and adipose tissue cells significantly increase in several cardiovascular diseases, including in atrial fibrillation (AF). EVs are engaged in cell-to-cell cooperation, endothelium integrity, inflammation, and immune response and are a cargo for several active molecules, such as regulatory peptides, receptors, growth factors, hormones, and lipids. Being transductors of the intercellular communication, EVs regulate angiogenesis, neovascularization, coagulation, and maintain tissue reparation. There is a large amount of evidence regarding the fact that AF is associated with elevated levels of EVs derived from platelets and mononuclears and a decreased number of EVs produced by endothelial cells. Moreover, some invasive procedures that are generally performed for the treatment of AF, i.e., pulmonary vein isolation, were found to be triggers for elevated levels of platelet and mononuclear EVs and, in turn, mediated the transient activation of the coagulation cascade. The review depicts the role of EVs in thrombogenicity in connection with a risk of thromboembolic complications, including ischemic stroke and systemic thromboembolism, in patients with various forms of AF.
1. Introduction
Atrial fibrillation (AF) is the most common form of cardiac arrhythmia amongst older people and patients with cardiovascular (CV) diseases (CVD) and continues to demonstrate steady growth in the general population [1]. The prevalence of AF is increasing at epidemic proportions in both developed and developing countries, regardless of the presence of conventional CV risk factors [2,3]. Indeed, the current prevalence of AF in the European Union is 7.3%, and it will increase to 89% by 2060 [1,3]. Moreover, at least 65% of senior citizens in the European Union will have AF in 2060, and paroxysmal, persistent, and permanent forms of AF are projected to be diagnosed in approximately 5,989,000, approximately 2,833,000, and approximately 5,579,000 of older people, respectively [3]. Electroanatomic and adverse cardiac remodeling resulting in natural CVD evolution and AF persistence is considered to be a substrate for the development of cardiac dysfunction, heart failure (HF) occurrence, and thromboembolic complications, which sufficiently reduce life span duration and quality of life in patients affected by this condition [4]. In addition, AF is independently associated with both high rates of morbidity, and mortality is a common cause of premature disability in CVD patients [5]. Overall, the risk of thromboembolism in these patients is not just associated with AF, but it also varies widely depending on coexisting comorbidities (HF, chronic kidney disease, chronic obstructive pulmonary disease, diabetes mellitus, obesity, and cardiomyopathy), low physical activity, patient age and gender, and methods of cardioversion and anticoagulation [6,7,8]. Despite the numerous benefits of CVD prevention therapy and its wide implementation in routine practice, there remains an unacceptably high risk of potentially devastating complications associated with catheter pulmonary vein isolation (PVI), such as stroke/transient ischemic attack and systemic thromboembolism during persistent AF or the occurrence of its permanent form [9]. The number of one-year recurrent AF episodes has remained high (20%) [10], whereas single-procedural 1-year and 5-year arrhythmia-free survival is 66% and 44%, respectively [11,12]. However, the prevention of thromboembolic complications remains the focus of pragmatic strategy development for AF therapy [13,14].
The extracellular vesicles (EVs) are vesicular structures that are secreted from numerous cells and supply several biologically active molecules (growth factors, active peptides, regulatory proteins, pro-inflammatory cytokines, micro-RNAs (miR)) that are involved in cell-to-cell communication, including in the modulation of tissue repair, inflammation, angiogenesis/neovascularization, immune response, extracellular matrix accumulation, and vascular integrity enhancement [15,16,17]. Moreover, EVs that originate from the activated or apoptotic cells exert variable effects that are dependent on a spectrum of encapsulated cytokines, proteome, lipidome, and miRs and have an epigenetic impact on target cells [16]. There is strong evidence of the fact that EVs that are derived from a large spectrum of circulating blood cells, including platelets, mononuclear cells/leucocytes, endothelial cells, and even adipose tissue cells and antigen-presenting cells, are a cargo for pro-coagulant phospholipids, mainly phosphatidylserine, active molecules, non-coding RNAs, and other components, that regulate coagulation cascade and play a crucial role in the incidence of AF-related thromboembolism [15,16,17]. This review recapitulates recent findings on the role of EVs in thrombogenicity in connection with a risk of thromboembolic complications, including ischemic stroke and systemic thromboembolism, in patients with various forms of AF.
2. Methodology
We searched the MEDLINE, EMBASE, Medline (PubMed), Web of Science, and Cochrane Central bibliographic databases with the keywords [exosome AND atrial fibrillation], [extracellular vesicles AND atrial fibrillation], [extracellular vesicles AND thrombogenicity] and found a total of 12 original articles written in English. We evaluated the quality of each article to ensure that the data were homogenous. We used the following criteria to determine the quality of eligible papers: full-length manuscript with an English abstract and published in a reputable journal, human study, data that were available for assessment, the presence of a control group, a clear and concise description of the methods by which EVs were determined and measured, and a lack of result misinterpretation. In the present study, we focus on original articles addressing EVs and AF.
3. Extracellular Vesicles: Definition, Nomenclature, Biological Function
According to the International Society on Extracellular Vesicles (ISEV), EVs are defined as a heterogenic group of lipid bilayer vesicular structures with a size in the range of 30–4000 nm that are released by all types of cultured cells and are found in abundance in body fluids (blood, lymph, saliva, urine, bile, synovial fluid, cerebrospinal fluid) [18]. EVs consist of three subpopulations: exosomes, microvesicles (MVs), and apoptotic bodies (ABs), that can be distinguished from each other based on their size, immune phenotypes, origin, biogenesis, and mechanism of release and component delivery [19,20,21]. Table 1 contains the main characteristics of EVs. Although a universal definition of EVs subpopulations remain elusive, the ISEV recommends not using other criteria apart from the size of the EVs to classify them because there is overlap among the different phenotypes of these vesicular structures [22]. Biological pathways of generation, shedding, and the release of EVs exert remarkable diversity. For instance, exosomes appear following endocytosis from endosomes, whereas MVs are synthesized after blebbing from the plasma membrane and being released in biological fluid and contain all of the antigens that are widely expressed on the surface of the mother cells [23]. In addition, MVs and exosomes are not only produced by cellular activation, but they are also produced via pro-inflammatory stimulation, shear stress, and the influence of pro-thrombotic and pro-apoptotic substances. ABs occur as the result of the shrinkage and blebbing of apoptotic cells, but there is alternative pathway that relates to lysosome vesicle secretion and secretory autophagy. Therefore, mechanical activation and hemolysis, which are common features in patients with CVD (valve stenosis, prosthetic valves, AF, HF) as well as non-CVD (infections, sepsis, and eclampsia), are strongly associated with apoptotic cell breakdown [24,25,26,27]. In fact, an evaluation of the EVs secretome demonstrated that different sub-populations of EVs had either overlapping protein components or coincidentally similar protein arrangements, and this was a consequence of the type of stimulation that caused the EVs to release and the type of the mother cells [28].
The exact circulation levels of the different EVs subpopulations in healthy individuals and in patients with CVD and non-CVD is unclear due to a lack of strong evidence regarding their concentrations due to high variability in the sensitivity and specificity of the detection methods used or the co-detection of contaminants [29]. However, it is widely agreed upon that the majority of circulating EVs are of a platelet-derived vesicular structure, whereas neutrophil-derived, mononuclear-derived, endothelial cell-derived, and red blood cell-derived vesicles have been found in by far lower concentrations when compared to platelet-derived ones [30].
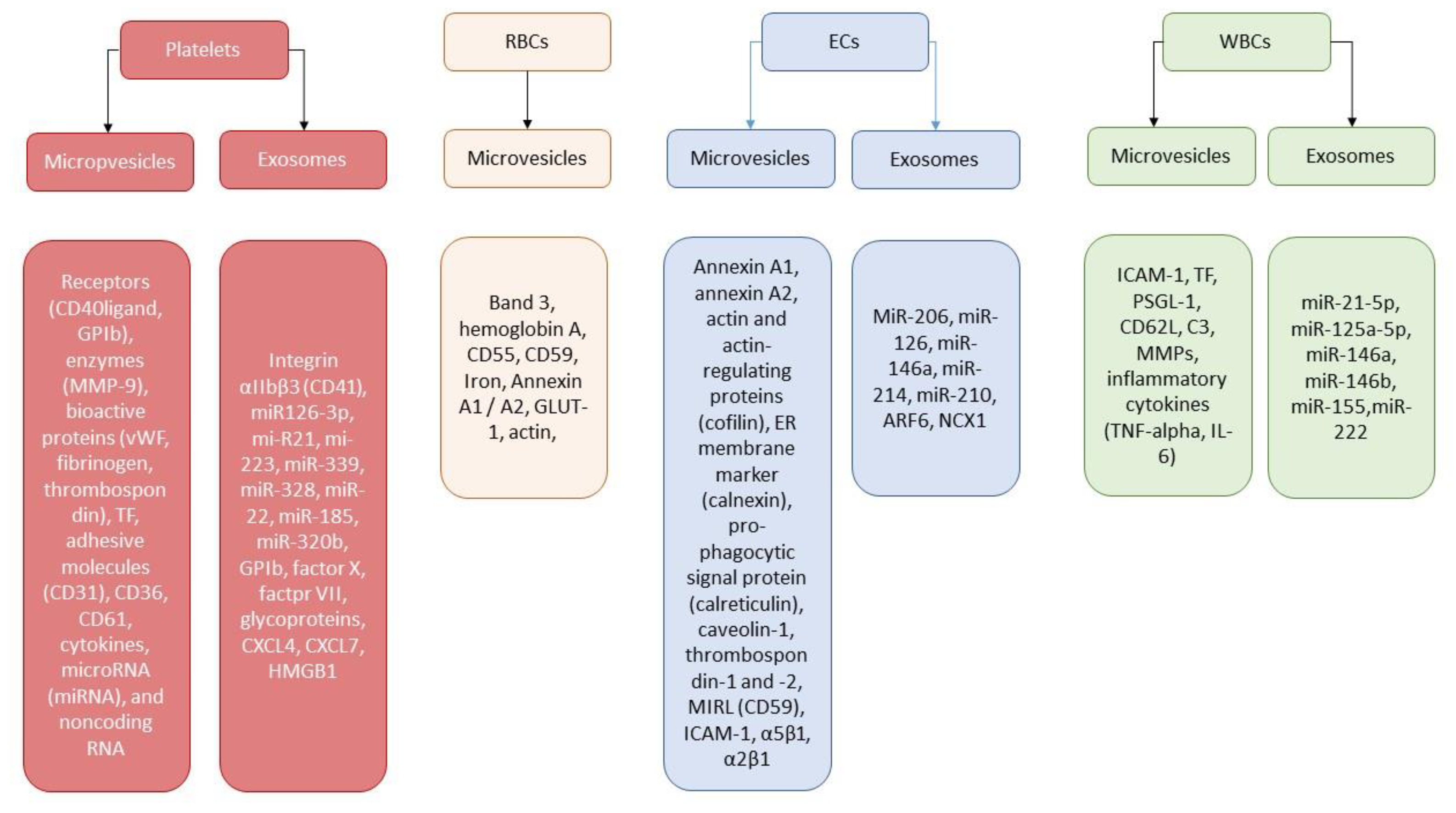
Nowadays, EVs are considered to be powerful mediator of cell-to-cell communication through the delivery of cargo proteins (adenosine diphosphate-ribosylation factor 6, Ras-related protein 22a, vesicle-soluble NSF attachment protein receptor, vesicle-associated membrane protein 3, T-cell internal antigen 1, argonaute-2, lipids, mRNA, miRNA long noncoding RNA, and occasionally genomic DNA) [31]. In addition, EVs directly transfer functional receptors, such as CD41, CD61, CD62, CXCR4, PAR-1, and PPRγ, from parental cells to recipient cells, contributing an axis for the regulation of their proliferation, differentiation, and activation. A large spectrum of miRNAs was observed in the EVs that were isolated from human parental cells. More often than not, the miRNAs that are incorporated into EVs act as negative regulators for several biological processes, including tissue reparation, vascular integrity, angiogenesis, neovascularization, immune response, and inflammation. Indeed, miR126-3p is responsible for the suppression of the expression of different inflammatory genes in the macrophages/mononuclears and thereby mediates cytokine-induced thrombogenicity and NETosis [32]. Platelet-derived EVs enriched in miR 21, miR-223, and miR-339 seem to be a modulator of expression of the platelet-derived growth factor receptor-beta in smooth muscle cells, playing a crucial role in plaque development and vascular remodeling [33]. Figure 1 illustrates the role of EVs’ secretome depending on the origin of the vesicles.
4. Extracellular Vesicles and Thrombogenicity/Thrombosis
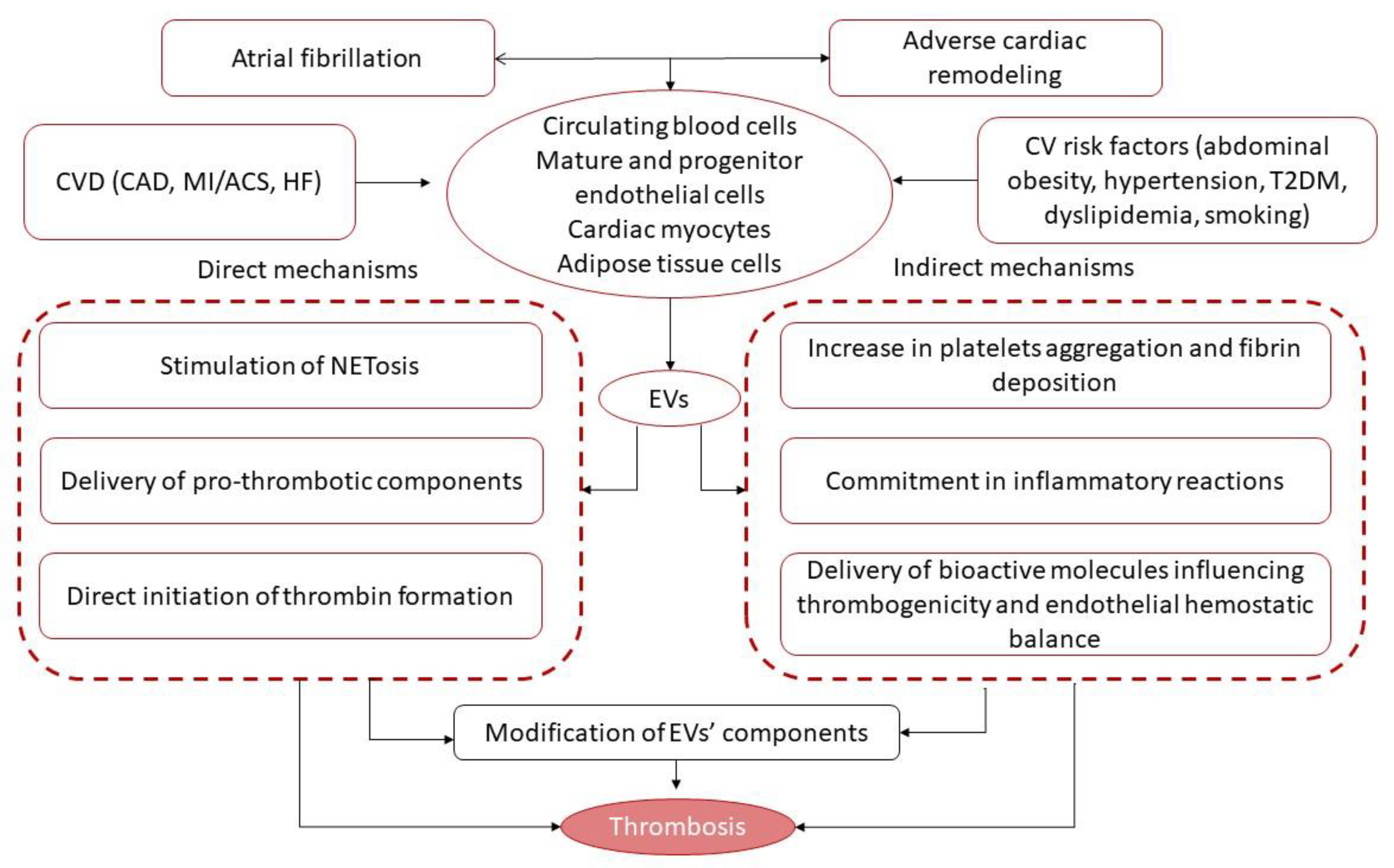
It has been suggested that cell-derived EVs that are enriched in lipids (phosphatidylserine, arachidonic acids), secretory phospholipase A2, factors of coagulation (factor X, factor VII, tissue factor), chromatin, and DNAs/RNAs might have 50- to 100-fold higher specific pro-coagulant activity than activated platelets [30,34]. The mechanisms by which these EVs exert their pro-coagulative abilities are considered to be quite complex (Figure 2).
First, secreted EVs may facilitate the formation of neutrophil extracellular traps (NETs), which may contribute to thrombus development and attenuate the counteracting effect of endogenous fibrinolytic systems [35,36]. Second, the presence of polyphosphate (polyP) in cell-derived EVs may promote thrombosis through a tissue factor-independent route, whereas these effects were initially described in cancer-associated thrombosis [37] and then extrapolated to others. Yet, the pro-coagulant activity to EVs that originated from mature endothelial cells was found to be up-regulated by the induction of the expression of adhesion proteins and several encapsulated pro-inflammatory cytokines, mainly IL-8 and tumor necrosis factor-alpha (TNF-alpha), on mother cells [38]. These mechanisms are rigorously regulated by the protease-activated receptor (PAR) 2 signaling pathway, which, in turn, mediates the rapid generation of pro-thrombotic components, such as inactive tissue factor/factor VII and integrin α5 β1 into the EVs secreted by endothelial cells [39]. Finally, the internationalization of the pro-thrombotic complex consists of tissue factor–factor VIIa–factor Xa by endothelial cells and regulates tissue factor availability for release on pro-coagulant EVs [40,41]. Third, the P2Y1 and P2Y12 receptors, which play a pivotal role in platelet activation and aggregation, seem to be transported by EVs as membrane-associated structures [42]. The next thrombogenicity-stimulating pathway is direct thrombin activation by EVs enriched by chemokines (CXCL4, CXCL7) and the cytoplasmic high-mobility group box 1 protein [43]. In addition, platelet-derived and endothelial cell-derived MVs and exosomes can stimulate coagulation independently after the mechanical stimulation of the parental cells or due to hemolysis [44].
Therefore, EVs can potentiate thrombosis through several indirect mechanisms, such as through an increase in platelet aggregation and fibrin deposition following the transfer of arachidonic acid [45], the down-regulation of endothelial cyclooxygenase (COX)-2 expression and prostacyclin synthesis via thromboxane A2-related mechanisms [46], and increased endothelial cell surface thrombogenicity and altered endothelial hemostatic balance [47]. It has been found that platelet-derived MVs are able to modulate the expression of (COX)-2 and prostacyclin production in both circulating monocytes and in progenitor/mature endothelial cells through the direct activation of the PKC/p42/p44 MAPK/p38 kinase and c-Jun N-terminal kinase/Elk-1pathways [48]. Indeed, these pathways contribute to vascular homeostasis through the regulation of plasmin generation on the endothelial cell layer and is a crucial player in ensuring thrombogenicity and blood clotting control [49]. The EVs that are mainly derived from endothelial cells participate in transfer growth factors (fibroblast growth factor, transforming growth factor-beta), active proteins (including annexin A2 ligand and CD40 ligand+), and receptors, resulting in TNF-alpha and IL-6 co-stimulation, and, in turn, lead to plasmin generation and the expression of both the urokinase-type plasminogen activator (uPA) and its receptor (uPAR) on the surface of endothelial cells [50]. All of these trigger an increase in their ability to bind exogenous uPA on uPAR and to subsequently maintain plasmin formation. Moreover, this was found to be a signal messenger for endothelial cell-derived EVs to induce plasmin generation and, in turn, affect tube formation in endothelial progenitor cells, thereby ensuring their proliferative and proteolytic activities [49]. Previous studies have shown that S100A10 is a member of the S100 family of Ca2+-binding proteins and was found to be abundantly distributed in progenitor and mature endothelial cells and protected from altered vascular integrity and hypercoagulation [51,52]. Indeed, this resulted in the loss of S100A10 from the endothelial cells, which exerted significant plasmin generation suppression [51,52,53]. It is possible that the EVs originating from activated endothelial cells are able to be a cargo for the kringle-2 domain of tPA, which plays a crucial role in S100A10-dependent plasmin generation [54]. Thus, decreased number and lowered functional activity of endothelial cell-derived EVs are considered to be a powerful factors for increased thrombogenicity.
These mechanisms based on both the synthesis and transfer of coagulation factors by EVs, but these can also be activated via the pro-inflammatory cytokine cascade, the proteasome-dependent mechanism, and apoptosis [55]. In fact, It is prudently suggested that these mechanisms overlap with each other. For instance, pro-inflammatory cytokine IL-33 and cholesterol were found to be powerful inductors for differential tissue factor expression and stimulators for monocyte subsets as well as for the release of pro-coagulant EVs into circulation from mother cells [55,56]. Consequently, inflammatory cytokines along with other factors generated during blood coagulation, such as platelet-derived lipid mediators (lysophosphatidate, phosphatidic acid and sphingosine 1-phosphate), may contribute to the formation of a pro-thrombotic state in CVD patients as well as potentiate neovascularization and angiogenesis [57]. Considerable attention has focused on the ability of pro-coagulant lipid components, mainly phospholipids derived through EVs, to be agonists for G-protein-coupled endothelial differentiation gene receptors, which seem to be important for the morphogenesis of capillary-like structures, promoting angiogenesis and supporting blood clotting [57]. On the other hand, numerous EVs enriched in phospholipids have been derived from activated platelets, resulting in blood coagulation and were eventually noticed to be key modulators of the chemo-attractive and proteolytic activity of the endothelial cells [58,59] that linked CV factors, comorbidities, endothelial integrity, and thrombogenicity [60].
Another pathophysiologic mechanism that would explain the link between AF and thrombogenicity is the indirect influence of the EVs on thromboembolic complications through adverse cardiac remodeling. Indeed, there is a wide range of resoundingly clear scientific proof of the fact that EVs enriched in cardiac protective microRNAs, such as miR-30d, miR-17-3p, miR-155, miR-222, and miR-378, are primary secreted by cardiac myocytes following acute-phase ischemia, hypoxia, inflammation, and biochemical stress and may ameliorate apoptosis through the activation of MAP4K4 (mitogen-associate protein kinase 4), the down-regulation of tumor protein p53-inducible nuclear protein 1, and the suppression of cardiac fibroblast proliferation and activation by directly targeting integrin α5 [61,62,63]. On the contrary, the chronic phases of these conditions were strongly associated with lower miR-30d expression in the myocardium and also decreased the amount of circulating EVs enriched in miR-30d, miR-17-3p, and miR-222, something that that is considered to be related to adverse cardiac remodeling in animal models and humans [62,63,64]. All of these are consequently linked to the over-expression of the genes that are implicated in fibrosis and inflammation and might play a role in the occurrence of non-valvular AF [65]. In addition, lowered levels of circulating endothelial cell-derived EVs, mainly the MVs that are able to regulate myocardial reparation and vascular integrity through supplying active molecules, regulatory peptides, miRNAs, and growth factors, were found to be predictors of adverse cardiac remodeling and AF [66,67]. In addition, the EVs derived from adipose tissues, including epicardial fat, as well as those originating from apoptotic mononuclear cells, were found to have encapsulated certain inflammatory cytokines, such as TNF-alpha, IL-1α, IL-1β, and RANTES, and they were also determined to have a cytotoxic impact on the myocardium, promoting left ventricular hypertrophy and arhythmogenesis [68,69]. Thus, the EVs originating from cardiac myocytes and circulating blood, mainly endothelial cells and mononuclear cells, may indirectly influence the development of AF through the mediation of cardiac hypertrophy, fibrosis, and oxidative stress/inflammation and aggravating atrial remodeling.
5. Atrial Fibrillation and Signature of EVs
Atrial fibrillation seems to be a powerful trigger for a pro-thrombotic state, which is associated with shedding EVs from many activated and apoptotic cell types in response to blood turbulence, inflammation, hemolysis, and adverse cardiac remodeling as well as an effect on coexisting CV risk factors and diseases, including HF, stroke, and atherosclerosis [70,71,72,73,74]. The changes in the EV signature in patients with different forms of AF are reported in Table 2.
5.1. Signature of EVs in Non-Valvular AF
Shaihov-Teper, O. et al. (2021) [69] investigated the signature of epicardial adipose tissue-derived EVs in patients with AF and found a significant difference between AF patients and individuals without AF in terms of the compounds of pro-inflammatory and pro-fibrotic cytokines and pro-fibrotic miRNAs encapsulated in the EVs. The authors concluded that the EVs from AF patients had more a profound pro-inflammatory, pro-fibrotic, and pro-arrhythmic epicardial adipose tissue-derived-EVs signature than patients without AF. [69]. Siwaponanan, P. et al. (2019) [75] reported that patients with non-valvular AF had sufficiently higher levels of total circulating MVs, platelet-derived MVs, and endothelial cell-derived MPs compared to healthy volunteers, even after adjusting for potential co-factors. The authors also noticed that the levels of circulating MVs enriched in pro-coagulant lipids (phosphatidylserine) did not significantly differ between the AF patients and healthy volunteers. On the contrary, there is a large amount of evidence regarding the fact that circulating pro-coagulant MVs were found in abundance in patients with persistent and/or permanent AF who were not receiving anticoagulant therapy compared to age-matched control subjects [76,77,78]. It is interesting to note that a number of platelet-derived MVs and endothelial cell-derived MVs were not distinguished in patients with non-valvular AF and control subjects with CV risk factors, but the total amount of EVs was significantly higher in the AF patients than it was in in healthy volunteers without known CV risk factors [76,77,78]. However, the presence of AF was found to be a solid predictor of the annexin V(+) MVs level, which seems to be a marker for hypercoagulation and a risk of both atrial thrombosis and systemic thromboembolism. Therefore, there is strong evidence for the fact that the amount of platelet-derived MVs was positively correlated with the thrombus diameter in non-valvular AF patients [79]. In another study, Wang, H. et al. (2020) [80] established that the levels of platelet-derived MVs in high-risk stroke patient according to the CHADS2 score were significantly higher compared to low to moderate risk AF patients. Finally, the data of the patients who were included in the Pulmonary Embolism Response Team (PERT) registry revealed that EVs may be a promising predictive indicator for acute pulmonary thromboembolism episodes in non-valvular patients with AF [88], but the clinical significance of the findings need elucidation in large-scale clinical trials.
5.2. Changes in EVs Profile during Anticoagulation Therapy in AF Patients
Lenart-Migdalska, A. et al. (2021) [81] investigated the impact of rivaroxaban on the circulating levels of both platelet-derived MVs (CD42b) and endothelial cell-derived MVs (CD144) amongst patients with non-valvular paroxysmal, persistent, or permanent AF (CHA2DS2-VASc score ≥ 2).
The authors found that the chronic administration of rivaroxaban was associated with an increase in the circulating number of both MVs phenotypes and that the peak plasma concentration of rivaroxaban was well correlated to the amount of MVs. In confirmation of these findings, Lenart-Migdalska, A. et al. (2020) [81] reported that dabigatran administration was associated with sufficient increases in the circulating levels of platelet-derived MVs (CD42b) in AF patients, whereas the amount of endothelial cell-derived (CD144) MVs was not elevated. The results of the West Birmingham Atrial Fibrillation Project yielded that the AF patient group had increased levels of apoptotic MVs compared to the disease control group and that warfarin and apixaban were similar in terms of their effect of reducing the pro-thrombotic index [82]. In fact, these findings clarify a possible pro-thrombotic role of MVs in oral anticoagulants, such as rivaroxaban, apixaban, and dabigatran, and that requires further investigation in large-scale clinical studies. The study by Duarte, R. et al. (2021) [83] revealed that patients with non-valvular AF undergoing warfarin or rivaroxaban treatment had higher levels of platelet-derived MVs; however, there was no difference in the levels of endothelial cell-derived MVs between the groups compared to the age- and sex-matched controls. These data may be important to stratify AF patients who are at risk of thromboembolic complications during anticoagulation therapy.
5.3. EV Signature in Patients with Valvular AF
There are limited data describing the changes that take place in the EV signature in valvular AF. Azzam H. and Zagloul M (2009) [84] reported that the levels of circulating platelet-derived MVs, labeled as CD41(+) particles, were significantly elevated in patients with rheumatic mitral stenosis and any form of AF compared to healthy volunteers. In addition, the authors noticed a significant correlation between the severity of mitral stenosis and circulating levels of platelet-derived MVs.
5.4. The Levels and Immune Phenotypes of EVs in AF Patients Treated with Catheter Ablation
However, it remained unclear whether patients with AF had an increased thrombotic status depending on the right and left atrium volume after pulmonary vein isolation. Jesel, L. et al. (2014) [85] no found atrial-specific differences in terms of the total levels of circulating pro-coagulant MVs, leukocyte-derived-MVs, or platelet-derived MVs. However, the authors noticed that the total amount of endothelial cell-derived MVs along with tissue factor activity and collagen-induced platelet aggregation were slightly increased in the right atrium and not in the left atrium. These findings are confusing to thoroughly explain the role of circulating pro-coagulant MVs in cardiac thrombus formation in non-valvular AF after pulmonary vein isolation. In addition, MVs-associated tissue factor activity was found to be reduced, whereas the fibrinolytic activity of the MVs in patients with acute episodes of AF treated with catheter ablation was improved [86]. On the contrary, Zhang, X. Z. et al. (2018) [87] reported that the hypercoagulable state after radiofrequency catheter ablation was significantly increased and exhibited a positive correlation with the total number of platelet-derived CD62P MVs. Moreover, it was revealed that the levels of platelet-derived MVs (CD62P) seven days after radiofrequency catheter ablation were significantly higher compared with those patients who were examined immediately after the procedure.
6. EVs in Routine Practice: Potential Benefits and Pitfalls
The findings support an emerging paradigm that involves EVs in thrombotic complications in patients with different forms of AF. Despite the fact that thrombogenicity can be directly modulated by platelet-derived EVs, resulting in altered hemodynamics, hemolysis, and blood turbulence as well as AF occurrence, an impaired circulating EV profile was found to be a promising biomarker for adverse cardiac remodeling, including left ventricular hypertrophy and fibrosis as well as a higher risk of AF [67]. Moreover, serum-derived EVs have been thoroughly identified as carrying potential biological markers, such as microRNAs, for the diagnosis and treatment of AF, especially with oral anticoagulants, but their clinical significance requires further investigations to clearly understand the reproducibility, sensitivity, and specificity of the targets [89]. Although specific markers and the methodology for determining various subsets of EVs have also been thoroughly described [22], there are no clear recommendations for a routine laboratory practice to measure EVs. In addition, there is no consent between investigations as to how to interpret and compare the results and whether a determination of an altered signature of EVs is better than single subset of ones to predict CV events in AF patients with and without HF. Indeed, some comorbidities that were found to have been frequently associated with AF, such as type 2 diabetes mellitus, abdominal obesity, and HF, exhibited an altered EVs profile along with impaired EVs proteinomics and lipidomics. Whether the secretome of different cells, including EVs, exerts a unique perspective for the diagnosis of a pro-thrombotic state in AF patients, regardless of comorbidities, remains uncertain. Another unresolved issue is the economic burden that occurs when a new biomarker is implemented into clinical practice. Unfortunately, there is no strong evidence to support that fact that the EVs signature is a superior conventional biomarker to predict thromboembolic complications, such as cardiac thrombosis, stroke, and systemic thromboembolism. All of these need to be investigated in large-scale clinical studies in the future.
7. Conclusions
Circulating EVs that are enriched in pro-coagulant components appear to be powerful triggers of cardiac thrombus formation and systemic thromboembolism. The altered signature of circulating EVs that are mainly derived from apoptotic cells and activated platelets and endothelial cells was found to be a promising predictor of potential thromboembolic complications, although the impact of different anticoagulants on the dynamic of these biomarkers is uncertain and requires clear elucidation in large clinical trials. The wide implementation of catheter ablation may require more advanced methods for the re-evaluation of potential thromboembolic risk, and in this context, EVs monitoring seems to be remarkably effective, but this approach needs validation in further investigations.
Author Contributions
Conceptualization, A.E.B. and A.A.B.; methodology, A.E.B.; validation, A.E.B. and A.A.B.; formal analysis, A.E.B.; investigation, A.E.B. and A.A.B.; resources, A.E.B. and A.A.B.; data curation, A.A.B.; writing—original draft preparation, A.E.B. and A.A.B.; writing—review and editing, A.E.B. and A.A.B.; visualization, A.A.B.; supervision, A.E.B.; project administration, A.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AF | atrial fibrillation |
| Alix | ALG2 interacting protein X |
| CV | cardiovascular |
| CVD | cardiovascular disease |
| EVs | extracellular vesicles |
| MAP4K4 | mitogen-associate protein kinase 4 |
| MVBs | multivesicular bodies |
| MVs | microvesicles |
| HF | heart failure |
| HMGB1 | cytoplasmic high-mobility group box 1 protein |
| PE | pulmonary embolism |
| PPARγ | peroxisome proliferator-activated receptor γ |
| PVI | pulmonary vein isolation |
| RANTES | Regulated upon Activation, Normal T Cell-Expressed and Presumably Secreted. |
| SNAREs | soluble N-ethylmaleimide-sensitive factor attachment protein receptors |
| TSG101 | tumor susceptibility gene 101 |
| TNF | tumor necrosis factor |
References
- Di Carlo, A.; Bellino, L.; Consoli, D.; Mori, F.; Zaninelli, A.; Baldereschi, M.; Cattarinussi, A.; D’Alfonso, M.G.; Gradia, C.; Sgherzi, B.; et al. Prevalence of atrial fibrillation in the Italian elderly population and projections from 2020 to 2060 for Italy and the European Union: The FAI Project. EP Eur. 2019, 21, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Tedrow, U.B.; Conen, D.; Ridker, P.M.; Cook, N.R.; Koplan, B.A.; Manson, J.E.; Buring, J.E.; Albert, C.M. The long- and short-term impact of elevated body mass index on the risk of new atrial fibrillation the WHS (women’s health study). J. Am. Coll. Cardiol. 2010, 55, 2319–2327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloosterman, M.; Crijns, H.; Van Gelder, I.C. Rising prevalence of atrial fibrillation in the elderly population: New challenges of geriatric cardiology. EP Eur. 2019, 21, 1451–1453. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Hua, C.; Jiang, C.; He, L.; Jia, Z.X.; Lyu, W.H.; Tang, R.B.; Sang, C.H.; Long, D.Y.; Dong, J.Z.; Ma, C.S.; et al. Causes of death and influencing factors of atrial fibrillation patients undergoing anticoagulation therapy. Zhonghua Xin Xue Guan Bing Za Zhi 2021, 49, 353–359. [Google Scholar] [CrossRef]
- Rankin, A.J.; Rankin, S.H. Cardioverting acute atrial fibrillation and the risk of thromboembolism: Not all patients are created equal. Clin. Med. 2017, 17, 419–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proietti, M.; Laroche, C.; Drozd, M.; Vijgen, J.; Cozma, D.C.; Drozdz, J.; Maggioni, A.P.; Boriani, G.; Lip, G.Y.H.; EORP-AF Investigators. Impact of chronic obstructive pulmonary disease on prognosis in atrial fibrillation: A report from the EURObservational Research Programme Pilot Survey on Atrial Fibrillation (EORP-AF) General Registry. Am. Heart J. 2016, 181, 83–91. [Google Scholar] [CrossRef]
- Boriani, G.; Laroche, C.; Diemberger, I.; Fantecchi, E.; Popescu, M.I.; Rasmussen, L.H.; Dan, G.-A.; Kalarus, Z.; Tavazzi, L.; Maggioni, A.P.; et al. ‘Real-world’ management and outcomes of patients with paroxysmal vs. non-paroxysmal atrial fibrillation in Europe: The EURObservational Research Programme-Atrial Fibrillation (EORP-AF) General Pilot Registry. EP Eur. 2016, 18, 648–657. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Laroche, C.; Boriani, G.; Cimaglia, P.; Dan, G.-A.; Santini, M.; Kalarus, Z.; Rasmussen, L.H.; Popescu, M.I.; Tica, O.; et al. Sex-related differences in presentation, treatment, and outcome of patients with atrial fibrillation in Europe: A report from the Euro Observational Research Programme Pilot survey on Atrial Fibrillation. EP Eur. 2015, 17, 24–31. [Google Scholar] [CrossRef]
- Sivasambu, B.; Balouch, M.A.; Zghaib, T.; Bajwa, R.J.; Chrispin, J.; Berger, R.D.; Ashikaga, H.; Nazarian, S.; Marine, J.E.; Calkins, H.; et al. Increased rates of atrial fibrillation recurrence following pulmonary vein isolation in overweight and obese patients. J. Cardiovasc. Electrophysiol. 2018, 29, 239–245. [Google Scholar] [CrossRef]
- Scherr, D.; Khairy, P.; Miyazaki, S.; Aurillac-Lavignolle, V.; Pascale, P.; Wilton, S.B.; Ramoul, K.; Komatsu, Y.; Roten, L.; Jadidi, A.; et al. Five-year outcome of catheter ablation of persistent atrial fibrillation using termination of atrial fibrillation as a procedural endpoint. Circulation. Arrhythmia Electrophysiol. 2015, 8, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saguner, A.M.; Maurer, T.; Wissner, E.; Santoro, F.; Lemes, C.; Mathew, S.; Sohns, C.; Heeger, C.H.; Reißmann, B.; Riedl, J.; et al. Catheter ablation of atrial fibrillation in very young adults: A 5-year follow-up study. EP Eur. 2018, 20, 58–64. [Google Scholar] [CrossRef]
- Jame, S.; Barnes, G. Stroke and thromboembolism prevention in atrial fibrillation. Heart 2020, 106, 10–17. [Google Scholar] [CrossRef]
- O’Neill, L.; Wielandts, J.Y.; Gillis, K.; Hilfiker, G.; Le Polain De Waroux, J.-B.; Tavernier, R.; Duytschaever, M.; Knecht, S. Catheter Ablation in Persistent AF, the Evolution towards a More Pragmatic Strategy. J. Clin. Med. 2021, 10, 4060. [Google Scholar] [CrossRef]
- Blanch-Ruiz, M.A.; Ortega-Luna, R.; Martínez-Cuesta, M.Á.; Álvarez, Á. The Neutrophil Secretome as a Crucial Link between Inflammation and Thrombosis. Int. J. Mol. Sci. 2021, 22, 4170. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.; Zulli, A.; Kerrigan, S.; Petrovic, D.; Kruzliak, P. Predictive role of circulating endothelial-derived microparticles in cardiovascular diseases. Clin. Biochem. 2015, 48, 562–568. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, R.; Hirata, R.; Hirata, M.H.; Aikawa, E. Circulating Extracellular Vesicles as Biomarkers and Drug Delivery Vehicles in Cardiovascular Diseases. Biomolecules 2021, 11, 388. [Google Scholar] [CrossRef]
- Théry, C.; Witwer, K.W. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): A position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef] [Green Version]
- Van der Pol, E.; Böing, A.N.; Gool, E.L.; Nieuwland, R. Recent developments in the nomenclature, presence, isolation, detection and clinical impact of extracellular vesicles. J. Thromb. Haemost. JTH 2016, 14, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Nederveen, J.P.; Warnier, G.; Di Carlo, A.; Nilsson, M.I.; Tarnopolsky, M.A. Extracellular Vesicles and Exosomes: Insights from Exercise Science. Front. Physiol. 2021, 11, 604274. [Google Scholar] [CrossRef] [PubMed]
- Askeland, A.; Borup, A.; Østergaard, O.; Olsen, J.V.; Lund, S.M.; Christiansen, G.; Kristensen, S.R.; Heegaard, N.; Pedersen, S. Mass-Spectrometry Based Proteome Comparison of Extracellular Vesicle Isolation Methods: Comparison of ME-kit, Size-Exclusion Chromatography, and High-Speed Centrifugation. Biomedicines 2020, 8, 246. [Google Scholar] [CrossRef]
- Witwer, K.W.; Goberdhan, D.C.; O’Driscoll, L.; Théry, C.; Welsh, J.A.; Blenkiron, C.; Buzás, E.I.; Di Vizio, D.; Erdbrügger, U.; Falcón-Pérez, J.M.; et al. Updating MISEV: Evolving the minimal requirements for studies of extracellular vesicles. J. Extracell. Vesicles 2021, 10, e12182. [Google Scholar] [CrossRef] [PubMed]
- Femminò, S.; Penna, C.; Margarita, S.; Comità, S.; Brizzi, M.F.; Pagliaro, P. Extracellular vesicles and cardiovascular system: Biomarkers and Cardioprotective Effectors. Vasc. Pharmacol. 2020, 135, 106790. [Google Scholar] [CrossRef]
- Puhm, F.; Boilard, E.; Machlus, K.R. Platelet Extracellular Vesicles: Beyond the Blood. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Abels, E.R.; Breakefield, X.O. Introduction to Extracellular Vesicles: Biogenesis, RNA Cargo Selection, Content, Release, and Uptake. Cell. Mol. Neurobiol. 2016, 36, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Puhm, F.; Flamand, L.; Boilard, E. Platelet extracellular vesicles in COVID-19: Potential markers and makers. J. Leukoc. Biol. 2022, 111, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.E. Microparticles in Chronic Heart Failure. Adv. Clin. Chem. 2017, 81, 1–41. [Google Scholar] [CrossRef] [PubMed]
- Bebelman, M.P.; Smit, M.J.; Pegtel, D.M.; Baglio, S.R. Biogenesis and function of extracellular vesicles in cancer. Pharmacol. Ther. 2018, 188, 1–11. [Google Scholar] [CrossRef]
- Arraud, N.; Linares, R.; Tan, S.; Gounou, C.; Pasquet, J.M.; Mornet, S.; Brisson, A.R. Extracellular vesicles from blood plasma: Determination of their morphology, size, phenotype and concentration. J. Thromb. Haemost. 2014, 12, 614–627. [Google Scholar] [CrossRef]
- Sinauridze, E.I.; Kireev, D.A.; Popenko, N.Y.; Pichugin, A.V.; Panteleev, M.A.; Krymskaya, O.V.; Ataullakhanov, F.I. Platelet microparticle membranes have 50- to 100-fold higher specific procoagulant activity than activated platelets. Thromb. Haemost. 2007, 97, 425–434. [Google Scholar]
- Simons, M.; Raposo, G. Exosomes—Vesicular carriers for intercellular communication. Curr. Opin. Cell Biol. 2009, 21, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Laffont, B.; Corduan, A.; Rousseau, M.; Duchez, A.C.; Lee, C.H.; Boilard, E.; Provost, P. Platelet microparticles reprogram macrophage gene expression and function. Thromb. Haemost. 2016, 115, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Silverman-Gavrila, R.; Silverman-Gavrila, L.; Bendeck, M.P. Cell division fidelity is altered during the vascular response to injury: Its novel role in atherosclerosis progression. Am. J. Pathol. 2013, 182, 628–639. [Google Scholar] [CrossRef]
- Fourcade, O.; Simon, M.F.; Viode, C.; Rugani, N.; Leballe, F.; Ragab, A.; Fournie, B.; Sarda, L.; Chap, H. Secretory phospholipase A2 generates the novel lipid mediator lysophosphatidic acid in membrane microvesicles shed from activated cells. Cell 1995, 80, 919–927. [Google Scholar] [CrossRef] [Green Version]
- Almeida, V.H.; Rondon, A.; Gomes, T.; Monteiro, R.Q. Novel Aspects of Extracellular Vesicles as Mediators of Cancer-Associated Thrombosis. Cells 2019, 8, 716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berezin, A. Neutrophil extracellular traps: The core player in vascular complications of diabetes mellitus. Diabetes Metab. Syndr. 2019, 13, 3017–3023. [Google Scholar] [CrossRef]
- Gasecka, A.; Böing, A.N.; Filipiak, K.J.; Nieuwland, R. Platelet extracellular vesicles as biomarkers for arterial thrombosis. Platelets 2017, 28, 228–234. [Google Scholar] [CrossRef]
- Rothmeier, A.S.; Versteeg, H.H.; Ruf, W. Factor VIIa-induced interaction with integrin controls the release of tissue factor on extracellular vesicles from endothelial cells. J. Thromb. Haemost. 2019, 17, 627–634. [Google Scholar] [CrossRef]
- Rothmeier, A.S.; Liu, E.; Chakrabarty, S.; Disse, J.; Mueller, B.M.; Østergaard, H.; Ruf, W. Identification of the integrin-binding site on coagulation factor VIIa required for proangiogenic PAR2 signaling. Blood 2018, 131, 674–685. [Google Scholar] [CrossRef] [PubMed]
- Zifkos, K.; Dubois, C.; Schäfer, K. Extracellular Vesicles and Thrombosis: Update on the Clinical and Experimental Evidence. Int. J. Mol. Sci. 2021, 22, 9317. [Google Scholar] [CrossRef]
- Rosas, M.; Slatter, D.A.; Obaji, S.G.; Webber, J.P.; Alvarez-Jarreta, J.; Thomas, C.P.; Aldrovandi, M.; Tyrrell, V.J.; Jenkins, P.V.; O’Donnell, V.B.; et al. The procoagulant activity of tissue factor expressed on fibroblasts is increased by tissue factor-negative extracellular vesicles. PLoS ONE 2020, 15, e0240189. [Google Scholar] [CrossRef] [PubMed]
- Gąsecka, A.; Rogula, S.; Eyileten, C.; Postuła, M.; Jaguszewski, M.J.; Kochman, J.; Mazurek, T.; Nieuwland, R.; Filipiak, K.J. Role of P2Y Receptors in Platelet Extracellular Vesicle Release. Int. J. Mol. Sci. 2020, 21, 6065. [Google Scholar] [CrossRef] [PubMed]
- Zarà, M.; Guidetti, G.F.; Camera, M.; Canobbio, I.; Amadio, P.; Torti, M.; Tremoli, E.; Barbieri, S.S. Biology and Role of Extracellular Vesicles (EVs) in the Pathogenesis of Thrombosis. Int. J. Mol. Sci. 2019, 20, 2840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suades, R.; Padro, T.; Vilahur, G.; Badimon, L. Circulating and platelet-derived microparticles in human blood enhance thrombosis on atherosclerotic plaques. Thromb. Haemost. 2012, 108, 1208–1219. [Google Scholar] [CrossRef] [PubMed]
- Barry, O.P.; Pratico, D.; Lawson, J.A.; FitzGerald, G.A. Transcellular activation of platelets and endothelial cells by bioactive lipids in platelet microparticles. J. Clin. Investig. 1997, 99, 2118–2127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caughey, G.E.; Cleland, L.G.; Gamble, J.R.; James, M.J. Up-regulation of endothelial cyclooxygenase-2 and prostanoid synthesis by platelets. Role of thromboxane A2. J. Biol. Chem. 2001, 276, 37839–37845. [Google Scholar] [CrossRef] [PubMed]
- Aharon, A.; Tamari, T.; Brenner, B. Monocyte-derived microparticles and exosomes induce procoagulant and apoptotic effects on endothelial cells. Thromb. Haemost. 2008, 100, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Barry, O.P.; Kazanietz, M.G.; Praticò, D.; FitzGerald, G.A. Arachidonic acid in platelet microparticles up-regulates cyclooxygenase-2-dependent prostaglandin formation via a protein kinase C/mitogen-activated protein kinase-dependent pathway. J. Biol. Chem. 1999, 274, 7545–7556. [Google Scholar] [CrossRef] [Green Version]
- Lacroix, R.; Sabatier, F.; Mialhe, A.; Basire, A.; Pannell, R.; Borghi, H.; Robert, S.; Lamy, E.; Plawinski, L.; Camoin-Jau, L.; et al. Activation of plasminogen into plasmin at the surface of endothelial microparticles: A mechanism that modulates angiogenic properties of endothelial progenitor cells in vitro. Blood 2007, 110, 2432–2439. [Google Scholar] [CrossRef]
- Plesner, T.; Behrendt, N.; Ploug, M. Structure, function and expression on blood and bone marrow cells of the urokinase-type plasminogen activator receptor, uPAR. Stem cells 1997, 15, 398–408. [Google Scholar] [CrossRef]
- Kwon, M.; MacLeod, T.J.; Zhang, Y.; Waisman, D.M. S100A10, annexin A2, and annexin a2 heterotetramer as candidate plasminogen receptors. Front. Biosci. 2005, 10, 300–325. [Google Scholar] [CrossRef] [Green Version]
- He, K.L.; Deora, A.B.; Xiong, H.; Ling, Q.; Weksler, B.B.; Niesvizky, R.; Hajjar, K.A. Endothelial cell annexin A2 regulates polyubiquitination and degradation of its binding partner S100A10/p11. J. Biol. Chem. 2008, 283, 19192–19200. [Google Scholar] [CrossRef] [Green Version]
- Miller, V.A.; Madureira, P.A.; Kamaludin, A.A.; Komar, J.; Sharma, V.; Sahni, G.; Thelwell, C.; Longstaff, C.; Waisman, D.M. Mechanism of plasmin generation by S100A10. Thromb. Haemost. 2017, 117, 1058–1071. [Google Scholar] [CrossRef]
- Bharadwaj, A.; Kempster, E.; Waisman, D.M. The Annexin A2/S100A10 Complex: The Mutualistic Symbiosis of Two Distinct Proteins. Biomolecules 2021, 11, 1849. [Google Scholar] [CrossRef] [PubMed]
- Stojkovic, S.; Thulin, Å.; Hell, L.; Thaler, B.; Rauscher, S.; Baumgartner, J.; Gröger, M.; Ay, C.; Demyanets, S.; Neumayer, C.; et al. IL-33 stimulates the release of procoagulant microvesicles from human monocytes and differentially increases tissue factor in human monocyte subsets. Thromb. Haemost. 2017, 117, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.L.; Reilly, M.P.; Casasanto, P.; McKenzie, S.E.; Williams, K.J. Cholesterol enrichment of human monocyte/macrophages induces surface exposure of phosphatidylserine and the release of biologically-active tissue factor-positive microvesicles. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Harvey, K.; Siddiqui, R.A.; Sliva, D.; Garcia, J.G.; English, D. Serum factors involved in human microvascular endothelial cell morphogenesis. J. Lab. Clin. Med. 2002, 140, 188–198. [Google Scholar] [CrossRef] [PubMed]
- English, D.; Welch, Z.; Kovala, A.T.; Harvey, K.; Volpert, O.V.; Brindley, D.N.; Garcia, J.G. Sphingosine 1-phosphate released from platelets during clotting accounts for the potent endothelial cell chemotactic activity of blood serum and provides a novel link between hemostasis and angiogenesis. FASEB J. 2000, 14, 2255–2265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limaye, V. The role of sphingosine kinase and sphingosine-1-phosphate in the regulation of endothelial cell biology. Endothelium 2008, 15, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.E. Impaired Immune Phenotype of Endothelial Cell-derived Micro Particles: The Missing Link between Diabetes-related States and Risk of Cardiovascular Complications? J. Data Min. Genom. Proteom. 2016, 7, 195–197. [Google Scholar] [CrossRef]
- Li, J.; Salvador, A.M.; Li, G.; Valkov, N.; Ziegler, O.; Yeri, A.; Yang Xiao, C.; Meechoovet, B.; Alsop, E.; Rodosthenous, R.S.; et al. Mir-30d Regulates Cardiac Remodeling by Intracellular and Paracrine Signaling. Circ. Res. 2021, 128, e1–e23. [Google Scholar] [CrossRef]
- He, W.; Huang, H.; Xie, Q.; Wang, Z.; Fan, Y.; Kong, B.; Huang, D.; Xiao, Y. MiR-155 Knockout in Fibroblasts Improves Cardiac Remodeling by Targeting Tumor Protein p53-Inducible Nuclear Protein 1. J. Cardiovasc. Pharmacol. Ther. 2016, 21, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Liu, H.; Gao, W.; Zhang, L.; Ye, Y.; Yuan, L.; Ding, Z.; Wu, J.; Kang, L.; Zhang, X.; et al. MicroRNA-378 suppresses myocardial fibrosis through a paracrine mechanism at the early stage of cardiac hypertrophy following mechanical stress. Theranostics 2018, 8, 2565–2582. [Google Scholar] [CrossRef] [PubMed]
- Schüttler, D.; Clauss, S.; Weckbach, L.T.; Brunner, S. Molecular Mechanisms of Cardiac Remodeling and Regeneration in Physical Exercise. Cells 2019, 8, 1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maries, L.; Marian, C.; Sosdean, R.; Goanta, F.; Sirbu, I.O.; Anghel, A. MicroRNAs—The Heart of Post-Myocardial Infarction Remodeling. Diagnostics 2021, 11, 1675. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Wang, J.; Tan, W.; Jiang, Y.; Wang, S.; Li, Q.; Yu, X.; Tan, J.; Liu, S.; Zhang, P.; et al. Extracellular vesicles from human embryonic stem cell-derived cardiovascular progenitor cells promote cardiac infarct healing through reducing cardiomyocyte death and promoting angiogenesis. Cell Death Dis. 2020, 11, 354. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.E.; Berezin, A.A. Extracellular Endothelial Cell-Derived Vesicles: Emerging Role in Cardiac and Vascular Remodeling in Heart Failure. Front. Cardiovasc. Med. 2020, 7, 47. [Google Scholar] [CrossRef]
- Bang, C.; Batkai, S.; Dangwal, S.; Gupta, S.K.; Foinquinos, A.; Holzmann, A.; Just, A.; Remke, J.; Zimmer, K.; Zeug, A.; et al. Cardiac fibroblast-derived microRNA passenger strand-enriched exosomes mediate cardiomyocyte hypertrophy. J. Clin. Investig. 2014, 124, 2136–2146. [Google Scholar] [CrossRef]
- Shaihov-Teper, O.; Ram, E.; Ballan, N.; Brzezinski, R.Y.; Naftali-Shani, N.; Masoud, R.; Ziv, T.; Lewis, N.; Schary, Y.; Levin-Kotler, L.P.; et al. Extracellular Vesicles from Epicardial Fat Facilitate Atrial Fibrillation. Circulation 2021, 143, 2475–2493. [Google Scholar] [CrossRef]
- Nomura, S.; Shimizu, M. Clinical significance of procoagulant microparticles. J. Intensive Care 2015, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Berezin, A.E.; Kremzer, A.; Berezina, T.; Martovitskaya, Y. The signature of circulating microparticles in heart failure patients with metabolic syndrome. J. Circ. Biomark. 2016, 5, 1849454416663659. [Google Scholar] [CrossRef]
- Lee, S.-T.; Chu, K.; Jung, K.-H.; Kim, J.-M.; Moon, H.-J.; Bahn, J.-J.; Im, W.-S.; Sunwoo, J.; Moon, J.; Kim, M.; et al. Circulating CD62E+ microparticles and cardiovascular outcomes. PLoS ONE 2012, 7, e35713. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xiao, Y.; Lin, Z.; Xiao, X.; He, C.; Bihl, J.C.; Zhao, B.; Ma, X.; Chen, Y. The Role of Circulating Platelets Microparticles and Platelet Parameters in Acute Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2015, 24, 2313–2320. [Google Scholar] [CrossRef] [Green Version]
- Jesel, L.; Abbas, M.; Toti, F.; Cohen, A.; Arentz, T.; Morel, O. Microparticles in atrial fibrillation: A link between cell activation or apoptosis, tissue remodelling and thrombogenicity. Int. J. Cardiol. 2013, 168, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Siwaponanan, P.; Keawvichit, R.; Udompunturak, S.; Hunnangkul, S.; Reesukumal, K.; Sukapirom, K.; Pattanapanyasat, K.; Krittayaphong, R. Altered profile of circulating microparticles in nonvalvular atrial fibrillation. Clin. Cardiol. 2019, 42, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Ederhy, S.; Di Angelantonio, E.; Mallat, Z.; Hugel, B.; Janower, S.; Meuleman, C.; Boccara, F.; Freyssinet, J.M.; Tedgui, A.; Cohen, A. Levels of circulating procoagulant microparticles in nonvalvular atrial fibrillation. Am. J. Cardiol. 2007, 100, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, A.; Chung, I.; Blann, A.D.; Lip, G.Y.H. Elevated platelet microparticle levels in nonvalvular atrial fibrillation: Relationship to p-selectin and antithrombotic therapy. Chest 2007, 131, 809–815. [Google Scholar] [CrossRef]
- Lenart-Migdalska, A.; Drabik, L.; Kaźnica-Wiatr, M.; Tomkiewicz-Pająk, L.; Podolec, P.; Olszowska, M. Increased Levels of Platelets and Endothelial-Derived Microparticles in Patients with Non-Valvular Atrial Fibrillation During Rivaroxaban Therapy. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211019465. [Google Scholar] [CrossRef]
- Wang, L.; Bi, Y.; Yu, M.; Li, T.; Tong, D.; Yang, X.; Zhang, C.; Guo, L.; Wang, C.; Kou, Y.; et al. Phosphatidylserine-exposing blood cells and microparticles induce procoagulant activity in non-valvular atrial fibrillation. Int. J. Cardiol. 2018, 258, 138–143. [Google Scholar] [CrossRef]
- Wang, H.; Song, N.P.; Li, J.P.; Wang, Z.H.; Ti, Y.; Li, Y.H.; Zhang, W.; Zhong, M. The microvesicle/CD36 complex triggers a prothrombotic phenotype in patients with non-valvular atrial fibrillation. J. Cell. Mol. Med. 2020, 24, 7331–7340. [Google Scholar] [CrossRef]
- Lenart-Migdalska, A.; Drabik, L.; Kaźnica-Wiatr, M.; Tomkiewicz-Pająk, L.; Podolec, P.; Olszowska, M. Flow Cytometric Assessment of Endothelial and Platelet Microparticles in Patients with Atrial Fibrillation Treated with Dabigatran. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620972467. [Google Scholar] [CrossRef] [PubMed]
- Voukalis, C.; Lip, G.Y.H.; Shantsila, E. Effects of antithrombotic drugs on the pro-thrombotic state in patients with atrial fibrillation: The west Birmingham atrial fibrillation project. Thromb. Res. 2021, 200, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Duarte, R.; Rios, D.; Figueiredo, E.L.; Caiaffa, J.; Silveira, F.R.; Lanna, R.; Alves, L.; Martins, G.L.; Reis, H.J.; Reis, E.A.; et al. Thrombin Generation and other hemostatic parameters in patients with atrial fibrillation in use of warfarin or rivaroxaban. J. Thromb. Thrombolysis 2021, 51, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Azzam, H.; Zagloul, M. Elevated platelet microparticle levels in valvular atrial fibrillation. Hematology 2009, 14, 357–360. [Google Scholar] [CrossRef]
- Jesel, L.; Arentz, T.; Herrera-Siklody, C.; Trenk, D.; Zobairi, F.; Abbas, M.; Weber, R.; Minners, J.; Toti, F.; Morel, O. Do atrial differences in endothelial damage, leukocyte and platelet activation, or tissue factor activity contribute to chamber-specific thrombogenic status in patients with atrial fibrillation? J. Cardiovasc. Electrophysiol. 2014, 25, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Pourtau, L.; Sellal, J.M.; Lacroix, R.; Poncelet, P.; Bernus, O.; Clofent-Sanchez, G.; Hocini, M.; Haïssaguerre, M.; Dignat-George, F.; Sacher, F.; et al. Platelet function and microparticle levels in atrial fibrillation: Changes during the acute episode. Int. J. Cardiol. 2017, 243, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.Z.; Liu, A.G.; Guo, M.L.; Guan, J.; Cai, S.L.; Du, Q.; Zhou, C.Y. Relationship of platelet microparticle CD62P and activated GP IIb/IIIa with hypercoagulable state after atrial fibrillation radiofrequency catheter ablation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 3919–3924. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Darki, A.; Hoppensteadt, D.; Darwish, I.; Syed, M.; Brailovsky, Y.; Fareed, J. Biomarkers of Thrombo-Inflammatory Responses in Pulmonary Embolism Patients with Pre-Existing Versus New-Onset Atrial Fibrillation. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211014964. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, X.; Li, H.; Li, Y.; Cheng, D.; Tang, Y.; Sang, H. Serum extracellular vesicles containing MIAT induces atrial fibrosis, inflammation and oxidative stress to promote atrial remodeling and atrial fibrillation via blockade of miR-485-5p-mediated CXCL10 inhibition. Clin. Transl. Med. 2021, 11, e482. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Secretome of EVs originated from different cells. Abbreviations: ARF6, ADP ribosylation factor 6; ECs, endothelial cells; RBCs, red blood cells; ER, endoplasmic reticulum; ICAM-1, intracellular adhesion molecule 1; CD62L, l-selectin; MIRL, membrane inhibitor of reactive lysis; MMPs, metalloproteinases; TNF-alpha, tumor necrosis factor-alpha; TF, tissue factor; vWF; Von Willebrand factor; CXCL, C-X-C motif ligand; HMGB1, high mobility group box 1; PSGL-1, P-selectin glycoprotein ligand-1; WBCs, white blood cells.
Figure 1.
Secretome of EVs originated from different cells. Abbreviations: ARF6, ADP ribosylation factor 6; ECs, endothelial cells; RBCs, red blood cells; ER, endoplasmic reticulum; ICAM-1, intracellular adhesion molecule 1; CD62L, l-selectin; MIRL, membrane inhibitor of reactive lysis; MMPs, metalloproteinases; TNF-alpha, tumor necrosis factor-alpha; TF, tissue factor; vWF; Von Willebrand factor; CXCL, C-X-C motif ligand; HMGB1, high mobility group box 1; PSGL-1, P-selectin glycoprotein ligand-1; WBCs, white blood cells.

Figure 2.
Pathogenetic pathways underlying EV-related thrombosis formation and increase in thrombogenicity. Abbreviations: CAD, coronary artery disease; ACS, acute coronary syndrome; EVs, extracellular vesicles; NETosis, neutrophil extracellular traps; AF, atrial fibrillation; CVD, cardiovascular diseases; CV, cardiovascular; HF, heart failure; T2DM, type 2 diabetes mellitus.
Figure 2.
Pathogenetic pathways underlying EV-related thrombosis formation and increase in thrombogenicity. Abbreviations: CAD, coronary artery disease; ACS, acute coronary syndrome; EVs, extracellular vesicles; NETosis, neutrophil extracellular traps; AF, atrial fibrillation; CVD, cardiovascular diseases; CV, cardiovascular; HF, heart failure; T2DM, type 2 diabetes mellitus.


{kind=link}
{kind=link}
Table 1.
Characteristics of EVs.
| Characteristics | Exosomes | Microvesicles | Apoptotic Bodies |
|---|---|---|---|
| Diameter, nm | 30–150 | 100–1000 | 500–4000 |
| Sedimentation, g | 100,000 | 20,000 | 16,000 |
| Pathway for biogenesis | Endocytosis from endosomes and exocytosis of late endosomes/MVBs | Blebbing from plasma membranes | Shrinkage and blebbing of apoptotic cells |
| Unconventional secretion pathway | Cellular activation | Early apoptosis | Lysosome vesicle secretion and secretory autophagy |
| Delivery contents | Alix, chaperones, Rab proteins, Rab GTPases, SNAREs, lipid rafts, proteins (flotillin), myokines, inflammatory cytokines, growth factors, miRs. | Arachidonic acid, cytokines, chemokine RANTES/CCL5, P-selectin, lipids, signaling proteins, miRNA, and microRNA, membrane-anchored receptors (PPARγ) and adhesion molecules | Organelles and/or nuclear content including chromatin, DNA, miRNAs, microRNAs, histones, oncogenes. |
| Membrane-specific antigens | Tetraspanins (CD9, CD81, CD63), TSG101, | Integrins, selectins, membrane proteins of parental cells | Annexin-V(+) |
Abbreviations: Alix, ALG2 interacting protein X; TSG101, tumor susceptibility gene 101; SNAREs, soluble N-ethylmaleimide-sensitive factor attachment protein receptors; PPARγ, peroxisome proliferator-activated receptor γ; MVBs, multivesicular bodies; RANTES, Regulated upon Activation, Normal T Cell-Expressed and Presumably Secreted; miRs, micro-RNAs; (+), positive.
Table 2.
The signature of EVs in patients with non-valvular AF.
| Type of AF | Study Design | n | Comparator(s) | Anticoagulation Therapy | Results | Reference |
|---|---|---|---|---|---|---|
| Paroxysmal, persistent, or permanent, non-valvular AF | Cohort study | 32 AF patients | 30 patients without AF | Non-treated | EVs received from AF patients had distinctive pro-inflammatory, pro-fibrotic, and pro-arrhythmic signature of epicardial adipose tissue-derived-EVs | [69] |
| Paroxysmal, persistent, or permanent, non-valvular | Cohort study | 66 AF patients | 33 healthy volunteers | Non-treated | ↑ total circulating MVs, platelet-derived MVs, endothelial-derived MVs. No difference in lipid enriched MVs between AF patients and healthy volunteers | [75] |
| Permanent and/or persistent, non-valvular | case–control study | 45 AF patients, 90 control individuals | 45 with CV risk factors and 45 without | Non-treated | ↑ Annexin V-positive MV levels | [76] |
| Paroxysmal, persistent, or permanent, non-valvular | Case-control study | 70 AF patients | 46 disease control subjects and 33 healthy control subjects | Non-treated | ↑ number of platelet-derived MVs, but no difference between AF patients and disease control subjects | [77] |
| Paroxysmal, persistent, or permanent, non-valvular | Cohort study | 37 AF patients (11 and 23 patients treated with 15 mg and 20 mg of rivaroxaban) | 11 patients (15 mg of rivaroxaban) | Rivaroxaban 15–20 mg daily | ↑ CD144(+) and CD42b(+) MV levels | [78] |
| Paroxysmal, persistent, or permanent, non-valvular | Cohort study | 78 AF patients | 36 controls | 18 AF patients with thrombi versus 60 AF patients without ones | The amount of platelet-derived MVs was positively correlated with thrombus diameter | [79] |
| Paroxysmal, persistent, or permanent, valvular | Cohort study | 210 AF patients | ‘low to moderate risk’ compared to ‘high risk’ for stroke according to the CHADS2 score | AVK/OAK | ↑ levels of platelet-derived MVs in high-risk patients compared with low to moderate risk patients | [80] |
| Paroxysmal, persistent, or permanent, valvular | Cohort study | 39 AF patients with CHA2DS2-VASc score ≥ 2 | 11 patients with dabigatran of 110 mg bid versus 28 patients with dabigatran of 150 mg bid | Dabigatran for 3 months or more | ↑circulating levels of platelet-derived MVs (CD42b) without changes in endothelial cell-derived (CD144) MVs | [81] |
| Paroxysmal, persistent, or permanent, valvular | Cohort study | 120 AF patients naïve to oral anticoagulants | 62 AF patients treated with antiplatelets | AVK/OAK/antiplatelets | Warfarin and apixaban demonstrated comparable positive effects on the levels of apoptotic MVs | [82] |
| Paroxysmal, persistent, or permanent, non-valvular | Cohort study | 60 AF patients | Age and sex matched controls | Warfarin or rivaroxaban | No difference in levels of endothelial cell-derived MVs between the groups. Patients taking rivaroxaban and warfarin had significantly higher platelet-derived EVs levels compared to control group. | [83] |
| Paroxysmal, persistent, or permanent, valvular | Case control study | 20 AF patients | 10 healthy volunteers who were in sinus rhythm | Non-treated | ↑ CD41(+) platelet-derived MVs | [84] |
| Paroxysmal/persistent, non-valvular | Case control study | 22 AF patients undergoing pulmonary vein isolation | 16 paroxysmal AF versus 6 persistent AF | AVK | No atrial-specific differences in the levels of several subsets of MVs in the left atrium volume, but not in the right atrial | [85] |
| Paroxysmal/persistent, non-valvular | Case control study | 37 AF patients referred for AF catheter ablation | paroxysmal (n = 21) and persistent (n = 16) AF patients referred for AF catheter ablation | AVK | ↓ pro-coagulant and ↑ fibrinolytic activity of MVs after catheter ablation | [86] |
| Paroxysmal/persistent, non-valvular | Case control study | 60 AF patients after radiofrequency catheter ablation | 20 healthy volunteers | AVK/OAK | ↑ levels of platelet-derived MVs (CD62P) in seven days after radiofrequency catheter ablation compared with immediate after the procedure | [87] |
Abbreviations: EVs, extracellular vesicles; AF, atrial fibrillation; CV, cardiovascular; ↑, increase; ↓, decrease; MVs, microvesicles; n, number of eligible patients; AVK, antagonists of vitamin K; OAK, oral anticoagulants.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Berezin, A.E.; Berezin, A.A. Extracellular Vesicles and Thrombogenicity in Atrial Fibrillation. Int. J. Mol. Sci. 2022, 23, 1774. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031774
AMA Style
Berezin AE, Berezin AA. Extracellular Vesicles and Thrombogenicity in Atrial Fibrillation. International Journal of Molecular Sciences. 2022; 23(3):1774. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031774
Chicago/Turabian StyleBerezin, Alexander E., and Alexander A. Berezin. 2022. "Extracellular Vesicles and Thrombogenicity in Atrial Fibrillation" International Journal of Molecular Sciences 23, no. 3: 1774. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms23031774
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.