
Effect of High-Intensity Interval Training on Physical Health in Coronary Artery Disease Patients: A Meta-Analysis of Randomized Controlled Trials



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Selection Criteria and Outcome Measure
2.3. Data Extraction
2.4. Risk of Bias and Quality Assessment
2.5. Statistical Analyses
3. Results
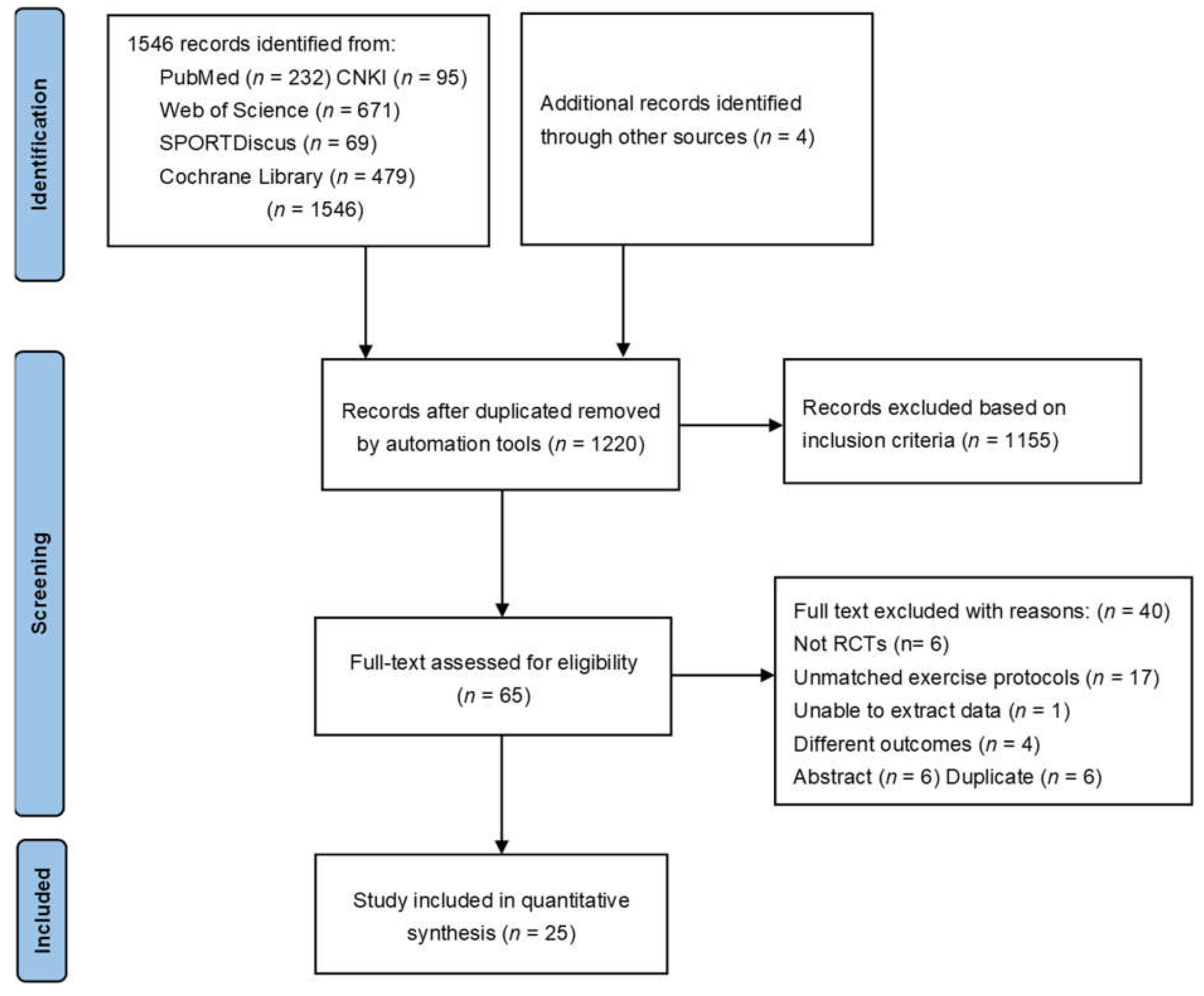
3.1. Study Identification and Selection
3.2. Characteristics of the Studies
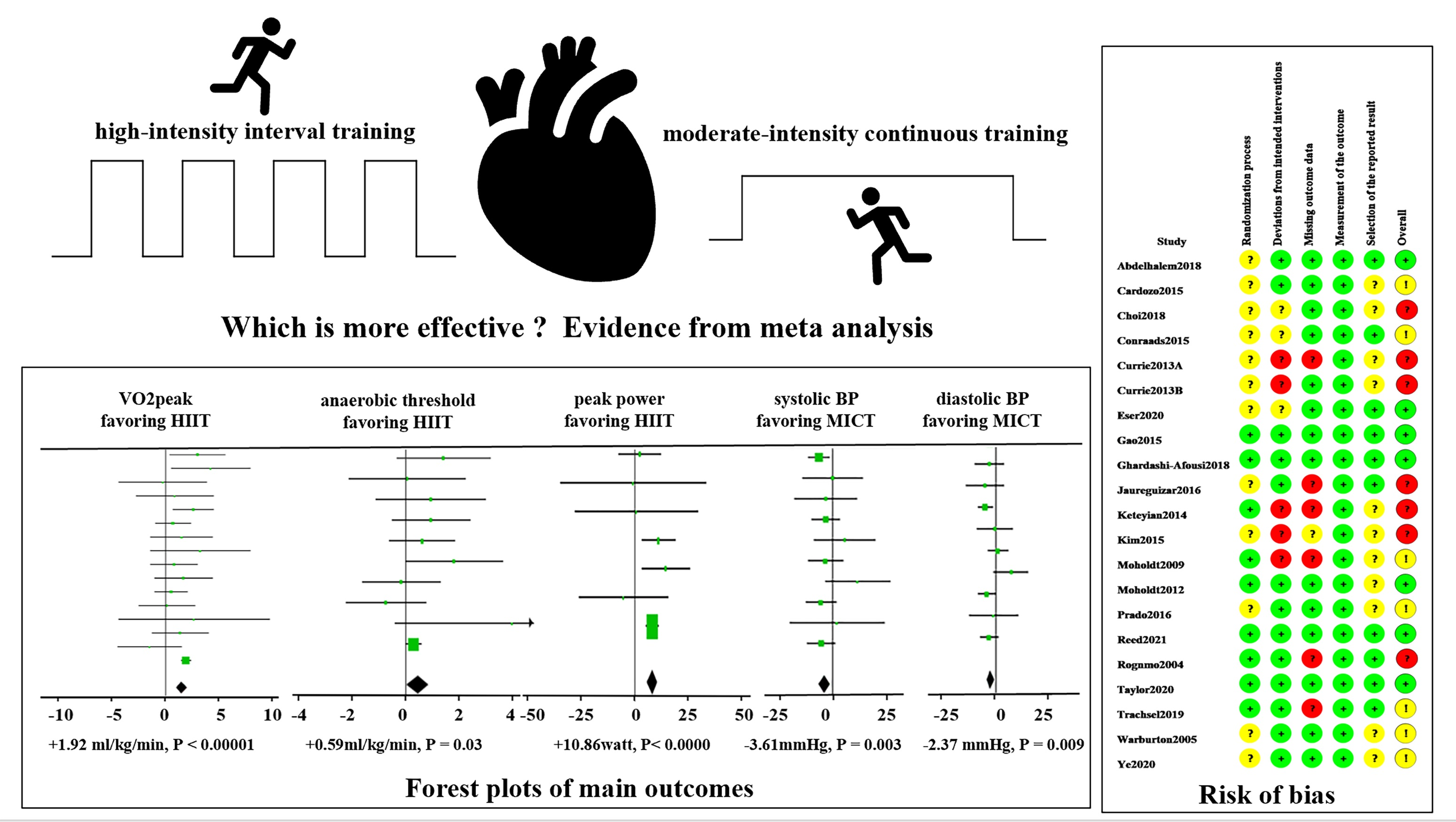
3.3. Risk of Bias and Quality Assessment
3.4. Effect of HIIT and MICT on VO2peak in CAD Patients
3.5. Effect of HIIT and MICT on Other Cardiorespiratory Parameters in CAD Patients
3.6. Effect of HIIT and MICT on CVD Risk Factors in CAD Patients
3.7. Effect of HIIT and MICT on Left Ventricular Function in CAD Patients
3.8. Effect of HIIT and MICT on QoL in CAD Patients
4. Discussion
5. Study Strength and Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Shengshou, H. Report on Cardiovascular Health and Diseases Burden in China: An Updated Summary of 2020. Chin. Circ. J. 2021, 36, 521–545. [Google Scholar]
- Laukkanen, J.A.; Kurl, S.; Salonen, R.; Rauramaa, R.; Salonen, J.T. The predictive value of cardiorespiratory fitness for cardiovascular events in men with various risk profiles: A prospective population-based cohort study. Eur. Heart J. 2004, 25, 1428–1437. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise Capacity and Mortality among Men Referred for Exercise Testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H. Effects of Endurance Training on Blood Pressure, Blood Pressure–Regulating Mechanisms, and Cardiovascular Risk Factors. Hypertension 2005, 46, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Oldridge, N. Exercise-based cardiac rehabilitation in patients with coronary heart disease: Meta-analysis outcomes revisited. Future Cardiol. 2012, 8, 729–751. [Google Scholar] [CrossRef]
- Shepherd, C.W.; While, A.E. Cardiac rehabilitation and quality of life: A systematic review. Int. J. Nurs. Stud. 2012, 49, 755–771. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Balady, G.J.; Chaitman, B.; Driscoll, D.; Foster, C.; Froelicher, E.; Gordon, N.; Pate, R.; Rippe, J.; Bazzarre, T. Recommendations for cardiovascular screening, staffing, and emergency policies at health/fitness facilities. Circulation 1998, 97, 2283–2293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Forman, D.E.; Lavie, C.J.; Guazzi, M. Should high-intensity-aerobic interval training become the clinical standard in heart failure? Heart Fail. Rev. 2013, 18, 95–105. [Google Scholar] [CrossRef]
- Vanhees, L.; Rauch, B.; Piepoli, M.; van Buuren, F.; Takken, T.; Börjesson, M.; Bjarnason-Wehrens, B.; Doherty, P.; Dugmore, D.; Halle, M.; et al. Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular disease (Part III). Eur. J. Prev. Cardiol. 2012, 19, 1333–1356. [Google Scholar] [CrossRef]
- Thum, J.S.; Parsons, G.; Whittle, T.; Astorino, T.A. High-Intensity Interval Training Elicits Higher Enjoyment than Moderate Intensity Continuous Exercise. PLoS ONE 2017, 12, e0166299. [Google Scholar] [CrossRef] [Green Version]
- Vella, C.A.; Taylor, K.; Drummer, D. High-intensity interval and moderate-intensity continuous training elicit similar enjoyment and adherence levels in overweight and obese adults. Eur. J. Sport Sci. 2017, 17, 1203–1211. [Google Scholar] [CrossRef]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-Intensity Interval Training in Cardiac Rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Quindry, J.C.; Franklin, B.A.; Chapman, M.; Humphrey, R.; Mathis, S. Benefits and Risks of High-Intensity Interval Training in Patients with Coronary Artery Disease. Am. J. Cardiol. 2019, 123, 1370–1377. [Google Scholar] [CrossRef]
- Elliott, A.D.; Rajopadhyaya, K.; Bentley, D.J.; Beltrame, J.F.; Aromataris, E.C. Interval Training Versus Continuous Exercise in Patients with Coronary Artery Disease: A Meta-Analysis. Heart Lung Circ. 2015, 24, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Liou, K.; Ho, S.; Fildes, J.; Ooi, S.-Y. High Intensity Interval versus Moderate Intensity Continuous Training in Patients with Coronary Artery Disease: A Meta-analysis of Physiological and Clinical Parameters. Heart Lung Circ. 2016, 25, 166–174. [Google Scholar] [CrossRef]
- Pattyn, N.; Coeckelberghs, E.; Buys, R.; Cornelissen, V.A.; Vanhees, L. Aerobic Interval Training vs. Moderate Continuous Training in Coronary Artery Disease Patients: A Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 687–700. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Yan, X.; Cai, X.; Li, J. Effects of High-Intensity Interval Training on Aerobic Capacity in Cardiac Patients: A Systematic Review with Meta-Analysis. BioMed Res. Int. 2017, 2017, 1–16. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Hannan, A.L.; Hing, W.; Simas, V.; Climstein, M.; Coombes, J.S.; Jayasinghe, R.; Byrnes, J.; Furness, J. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: A systematic review and meta-analysis. Open Access J. Sports Med. 2018, 9, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Rognmo, Ø.; Hetland, E.; Helgerud, J.; Hoff, J.; Slørdahl, S.A. High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 216–222. [Google Scholar] [CrossRef]
- Amundsen, B.H.; Rognmo, Ø.; Hatlen-Rebhan, G.; Slørdahl, S.A. High-intensity aerobic exercise improves diastolic function in coronary artery disease. Scand. Cardiovasc. J. 2008, 42, 110–117. [Google Scholar] [CrossRef]
- A Rocco, E.A.; Prado, D.M.; Silva, A.G.; Lazzari, J.M.A.; Bortz, P.C.; Rocco, D.F.M.; Rosa, C.G.; Furlan, V. Effect of continuous and interval exercise training on the PETCO2 response during a graded exercise test in patients with coronary artery disease. Clinics (Sao Paulo) 2012, 67, 623–627. [Google Scholar] [CrossRef]
- Conraads, V.M.; Pattyn, N.; De Maeyer, C.; Beckers, P.J.; Coeckelberghs, E.; Cornelissen, V.A.; Denollet, J.; Frederix, G.; Goetschalckx, K.; Hoymans, V.Y.; et al. Aerobic interval training and continuous training equally improve aerobic exercise capacity in patients with coronary artery disease: The SAINTEX-CAD study. Int. J. Cardiol. 2015, 179, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Jaureguizar, K.V.; Vicente-Campos, D.; Bautista, L.R.; de la Peña, C.H.; Gómez, M.J.; Rueda, M.J.; Fernández, M.I. Effect of High-Intensity Interval Versus Continuous Exercise Training on Functional Capacity and Quality of Life in Patients With Coronary Artery Disease: A Randomized Clinical Trial. J. Cardiopulm. Rehabil. Prev. 2016, 36, 96–105. [Google Scholar] [CrossRef]
- Prado, D.M.; Rocco, E.A.; Silva, A.G.; Rocco, D.F.; Pacheco, M.T.; Silva, P.F.; Furlan, V. Effects of continuous vs interval exercise training on oxygen uptake efficiency slope in patients with coronary artery disease. Braz. J. Med. Biol. Res. 2016, 49, e4890. [Google Scholar] [CrossRef] [Green Version]
- Pattyn, N.; Beckers, P.; Cornelissen, V.A.; Coeckelberghs, E.; De Maeyer, C.; Frederix, G.; Goetschalckx, K.; Possemiers, N.; Schepers, D.; Van Craenenbroeck, E.M.; et al. The effect of aerobic interval training and continuous training on exercise capacity and its determinants. Acta Cardiol. 2017, 72, 328–340. [Google Scholar] [CrossRef]
- Van De Heyning, C.M.; De Maeyer, C.; Pattyn, N.; Beckers, P.J.; Cornelissen, V.A.; Goetschalckx, K.; Possemiers, N.; Van Craenenbroeck, E.M.; Voigt, J.-U.; Vanhees, L.; et al. Impact of aerobic interval training and continuous training on left ventricular geometry and function: A SAINTEX-CAD substudy. Int. J. Cardiol. 2018, 257, 193–198. [Google Scholar] [CrossRef]
- Villelabeitia-Jaureguizar, K.; Vicente-Campos, D.; Senen, A.B.; Jiménez, V.V.H.; Bautista, L.L.R.; Garrido-Lestache, M.E.B.; Chicharro, J.L. Mechanical efficiency of high versus moderate intensity aerobic exercise in coronary heart disease patients: A randomized clinical trial. Cardiol. J. 2019, 26, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Eser, P.; Jaeger, E.; Marcin, T.; Herzig, D.; Trachsel, L.; Wilhelm, M. Acute and chronic effects of high-intensity interval and moderate-intensity continuous exercise on heart rate and its variability after recent myocardial infarction: A randomized controlled trial. Ann. Phys. Rehabil. Med. 2020, 101444. [Google Scholar] [CrossRef]
- Moholdt, T.T.; Amundsen, B.H.; Rustad, L.A.; Wahba, A.; Løvø, K.T.; Gullikstad, L.R.; Bye, A.; Skogvoll, E.; Wisløff, U.; Slørdahl, S.A. Aerobic interval training versus continuous moderate exercise after coronary artery bypass surgery: A randomized study of cardiovascular effects and quality of life. Am. Heart J. 2009, 158, 1031–1037. [Google Scholar] [CrossRef]
- Moholdt, T.; Aamot, I.L.; Granøien, I.; Gjerde, L.; Myklebust, G.; Walderhaug, L.; Brattbakk, L.; Hole, T.; Graven, T.; Stølen, T.O.; et al. Aerobic interval training increases peak oxygen uptake more than usual care exercise training in myocardial infarction patients: A randomized controlled study. Clin. Rehabil. 2011, 26, 33–44. [Google Scholar] [CrossRef]
- Cardozo, G.G.; Oliveira, R.B.; Farinatti, P. Effects of High Intensity Interval versus Moderate Continuous Training on Markers of Ventilatory and Cardiac Efficiency in Coronary Heart Disease Patients. Sci. World J. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Currie, K.D.; Dubberley, J.B.; Mckelvie, R.S.; MacDonald, M.J. Low-Volume, High-Intensity Interval Training in Patients with CAD. Med. Sci. Sports Exerc. 2013, 45, 1436–1442. [Google Scholar] [CrossRef] [Green Version]
- Currie, K.D.; Rosen, L.M.; Millar, P.J.; McKelvie, R.S.; MacDonald, M.J. Heart rate recovery and heart rate variability are unchanged in patients with coronary artery disease following 12 weeks of high-intensity interval and moderate-intensity endurance exercise training. Appl. Physiol. Nutr. Metab. 2013, 38, 644–650. [Google Scholar] [CrossRef]
- Keteyian, S.J.; Hibner, B.A.; Bronsteen, K.; Kerrigan, D.; Aldred, H.A.; Reasons, L.M.; Saval, M.A.; Brawner, C.A.; Schairer, J.R.; Thompson, T.M.; et al. Greater Improvement in Cardiorespiratory Fitness Using Higher-Intensity Interval Training in the Standard Cardiac Rehabilitation Setting. J. Cardiopulm. Rehabil. Prev. 2014, 34, 98–105. [Google Scholar] [CrossRef]
- Trachsel, L.-D.; Nigam, A.; Fortier, A.; Lalongé, J.; Juneau, M.; Gayda, M. Moderate-intensity continuous exercise is superior to high-intensity interval training in the proportion of VO2peak responders after ACS. Rev. Esp. Cardiol. (Engl. Ed.) 2019, 73, 725–733. [Google Scholar] [CrossRef]
- Warburton, D.E.; McKenzie, D.C.; Haykowsky, M.J.; Taylor, A.; Shoemaker, P.; Ignaszewski, A.P.; Chan, S.Y. Effectiveness of High-Intensity Interval Training for the Rehabilitation of Patients With Coronary Artery Disease. Am. J. Cardiol. 2005, 95, 1080–1084. [Google Scholar] [CrossRef]
- Reed, J.L.; Terada, T.; Cotie, L.M.; Tulloch, H.E.; Leenen, F.H.; Mistura, M.; Hans, H.; Wang, H.-W.; Vidal-Almela, S.; Reid, R.D.; et al. The effects of high-intensity interval training, Nordic walking and moderate-to-vigorous intensity continuous training on functional capacity, depression and quality of life in patients with coronary artery disease enrolled in cardiac rehabilitation: A randomized controlled trial (CRX study). Prog. Cardiovasc. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Choi, H.-Y.; Han, H.-J.; Choi, J.-W.; Jung, H.-Y.; Joa, K.-L. Superior Effects of High-Intensity Interval Training Compared to Conventional Therapy on Cardiovascular and Psychological Aspects in Myocardial Infarction. Ann. Rehabil. Med. 2018, 42, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Choi, H.E.; Lim, M.H. Effect of High Interval Training in Acute Myocardial Infarction Patients with Drug-Eluting Stent. Am. J. Phys. Med. Rehabil. 2015, 94, 879–886. [Google Scholar] [CrossRef]
- Gao, Z.; Ji, P.; Xia, Y.; Wang, L. Effects of different intensity aerobic exercise on cardiac function and exercise endurance in patients after percutaneous coronary intervention. Chin. J. Rehabil. Med. 2015, 30, 344–348. [Google Scholar]
- Ye, R.; Sun, L.; Zhang, Q.; Wang, K. Influence of aerobic exercise intensity on cardiac function and exercise tolenrance in patients with stroke complicated coronaty heart disease. Chin. J. Cardiovasc. Rehabil. Med. 2020, 29, 536–540. [Google Scholar]
- Ghardashi-Afousi, A.; Holisaz, M.T.; Shirvani, H.; Pishgoo, B. The effects of low-volume high-intensity interval versus moderate intensity continuous training on heart rate variability, and hemodynamic and echocardiography indices in men after coronary artery bypass grafting: A randomized clinical trial study. ARYA Atheroscler. 2018, 14, 260–271. [Google Scholar] [CrossRef]
- Taylor, J.L.; Holland, D.J.; Keating, S.E.; Leveritt, M.D.; Gomersall, S.R.; Rowlands, A.V.; Bailey, T.G.; Coombes, J.S. Short-term and Long-term Feasibility, Safety, and Efficacy of High-Intensity Interval Training in Cardiac Rehabilitation. JAMA Cardiol. 2020, 5, 1382. [Google Scholar] [CrossRef]
- Abdelhalem, A.; Shabana, A.; Onsy, A.; Gaafar, A. High intensity interval training exercise as a novel protocol for cardiac rehabilitation program in ischemic Egyptian patients with mild left ventricular dysfunction. Egypt. Heart J. 2018, 70, 287–294. [Google Scholar] [CrossRef]
- Keteyian, S.J.; Brawner, C.A.; Savage, P.D.; Ehrman, J.K.; Schairer, J.; Divine, G.; Aldred, H.; Ophaug, K.; Ades, P.A. Peak aerobic capacity predicts prognosis in patients with coronary heart disease. Am. Heart J. 2008, 156, 292–300. [Google Scholar] [CrossRef]
- Rankin, A.J.; MacIntyre, P.; Hillis, W.S.; Rankin, A.C. Walk or run? Is high-intensity exercise more effective than moderate-intensity exercise at reducing cardiovascular risk? Scott. Med. J. 2012, 57, 99–102. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: Cardiopulmonary emphasis. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Durães, A.R.; Dos Reis, H.F.C.; Neves, V.R.; Martinez, B.P.; Carvalho, V.O. High-intensity interval training versus moderate-intensity continuous training on exercise capacity and quality of life in patients with coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 1696–1707. [Google Scholar] [CrossRef]
- Pattyn, N.; Beulque, R.; Cornelissen, V. Aerobic Interval vs. Continuous Training in Patients with Coronary Artery Disease or Heart Failure: An Updated Systematic Review and Meta-Analysis with a Focus on Secondary Outcomes. Sports Med. 2018, 48, 1189–1205. [Google Scholar] [CrossRef]
- Qin, Y.; Bundhun, P.K.; Yuan, Z.-L.; Chen, M.-H. The effect of high-intensity interval training on exercise capacity in post-myocardial infarction patients: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2021. [Google Scholar] [CrossRef]
- Gerlach, S.; Mermier, C.; Kravitz, L.; Degnan, J.; Dalleck, L.; Zuhl, M. Comparison of Treadmill and Cycle Ergometer Exercise During Cardiac Rehabilitation: A Meta-analysis. Arch. Phys. Med. Rehabilitation 2020, 101, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.; Quan, M.; Zhuang, J. Effect of High-Intensity Interval Training versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Children and Adolescents: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vromen, T.; Kraal, J.; Kuiper, J.; Spee, R.; Peek, N.; Kemps, H. The influence of training characteristics on the effect of aerobic exercise training in patients with chronic heart failure: A meta-regression analysis. Int. J. Cardiol. 2016, 208, 120–127. [Google Scholar] [CrossRef]
- Gevaert, A.; Adams, V.; Bahls, M.; Bowen, T.S.; Cornelissen, V.; Dörr, M.; Hansen, D.; Mc Kemps, H.; Leeson, P.; Van Craenenbroeck, E.M.; et al. Towards a personalised approach in exercise-based cardiovascular rehabilitation: How can translational research help? A ‘call to action’ from the Section on Secondary Prevention and Cardiac Rehabilitation of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2020, 27, 1369–1385. [Google Scholar] [CrossRef]
- Araujo, B.; Leite, J.C.; Fuzari, H.; Pereira, D.S.R.; Remigio, M.I.; Dornelas, D.A.A.; Lima, C.S.; Cunha, B.D. Influence of High-Intensity Interval Training Versus Continuous Training on Functional Capacity in Individuals with Heart Failure: A Systematic Review and Meta-Analysis. J. Cardiopulm. Rehabil. Prev. 2019, 39, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Chen, P.; Zhu, J. The Effects of Interval Training and Continuous Training on Cardiopulmonary Fitness and Exercise Tolerance of Patients with Heart Failure—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6761. [Google Scholar] [CrossRef]
- Hansen, D.; Abreu, A.; Ambrosetti, M.; Cornelissen, V.; Gevaert, A.; Kemps, H.; Laukkanen, J.A.; Pedretti, R.; Simonenko, M.; Wilhelm, M.; et al. Exercise intensity assessment and prescription in cardiovascular rehabilitation and beyond: Why and how: A position statement from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021. [Google Scholar] [CrossRef]
- Sarullo, F.M.; Fazio, G.; Brusca, I.; Fasullo, S.; Paterna, S.; Licata, P.; Novo, G.; Novo, S.; Di Pasquale, P. Cardiopulmonary Exercise Testing in Patients with Chronic Heart Failure: Prognostic Comparison from Peak VO2 and VE/VCO2 Slope. Open Cardiovasc. Med. J. 2010, 4, 127–134. [Google Scholar] [CrossRef]
- Ferrari, R.; Fox, K. Heart rate reduction in coronary artery disease and heart failure. Nat. Rev. Cardiol. 2016, 13, 493–501. [Google Scholar] [CrossRef]
- Aune, D.; Sen, A.; Ó’Hartaigh, B.; Janszky, I.; Romundstad, P.R.; Tonstad, S.; Vatten, L.J. Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality—A systematic review and dose–response meta-analysis of prospective studies. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 504–517. [Google Scholar] [CrossRef]
- Iellamo, F.; Manzi, V.; Caminiti, G.; Vitale, C.; Castagna, C.; Massaro, M.; Franchini, A.; Rosano, G.; Volterrani, M. Matched dose interval and continuous exercise training induce similar cardiorespiratory and metabolic adaptations in patients with heart failure. Int. J. Cardiol. 2013, 167, 2561–2565. [Google Scholar] [CrossRef] [PubMed]
- Wisloff, U.; Stoylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, O.; Haram, P.M.; Tjonna, A.E.; Helgerud, J.; Slordahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Palermi, S.; Iacono, O.; Sirico, F.; Modestino, M.; Ruosi, C.; Spera, R.; De Luca, M. The complex relationship between physical activity and diabetes: An overview. J. Basic Clin. Physiol. Pharmacol. 2021. [Google Scholar] [CrossRef]
- Mendes, R.; Sousa, N.; Themudo-Barata, J.L.; Reis, V.M. High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Middle-Aged and Older Patients with Type 2 Diabetes: A Randomized Controlled Crossover Trial of the Acute Effects of Treadmill Walking on Glycemic Control. Int. J. Environ. Res. Public Health 2019, 16, 4163. [Google Scholar] [CrossRef] [Green Version]
- Winding, K.M.; Munch, G.W.; Iepsen, U.W.; van Hall, G.; Pedersen, B.K.; Mortensen, S.P. The effect on glycaemic control of low-volume high-intensity interval training versus endurance training in individuals with type 2 diabetes. Diabetes Obes. Metab. 2018, 20, 1131–1139. [Google Scholar] [CrossRef] [Green Version]
- De Nardi, A.T.; Tolves, T.; Lenzi, T.L.; Signori, L.U.; da Silva, A.M.V. High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2018, 137, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Balady, G.J.; Williams, M.A.; Ades, P.A.; Bittner, V.; Comoss, P.; Foody, J.A.; Franklin, B.; Sanderson, B.; Southard, D. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. J. Cardiopulm. Rehabil. Prev. 2007, 27, 121–129. [Google Scholar] [PubMed]
- Palermi, S.; Bragazzi, N.L.; Cular, D.; Ardigò, L.P.; Padulo, J. How chest press-based exercises can alleviate the burden of cardiovascular diseases. Hum. Mov. 2021, 22, 4. [Google Scholar] [CrossRef]
- Currie, K.D.; Bailey, K.J.; Jung, M.E.; McKelvie, R.S.; MacDonald, M.J. Effects of resistance training combined with moderate-intensity endurance or low-volume high-intensity interval exercise on cardiovascular risk factors in patients with coronary artery disease. J. Sci. Med. Sport 2015, 18, 637–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]


 : filled studies).
: filled studies).
: filled studies).
: filled studies).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Disease | Subjects (N, DR) | Ages (M ± SD) | Outcomes |
|---|---|---|---|---|
| Abdelhalem 2018, Egypt | CAD | HIIT (18M/2F) MICT (16M/4F), ND | HIIT(54.65 ± 7.63) MICT (51.95 ± 8.07) | LVEF, TC, LDL-C, HDL-C, TG |
| Amundsen 2008, Norway Rognmo 2004, Norway | CAD | HIIT (6M/2F, 27%) MICT(8M/1F,10%) | HIIT (63 ± 11) MICT (61 ± 7) | LVEDD |
| VO2peak, SBP, DBP, RER, HRrest, HRpeak | ||||
| Cardozo 2015, Brazil | CAD | HIIT (15M/5F) MICT (16M/8F), ND | HIIT (56 ± 12) MICT (62 ± 12) | VO2peak, AT, peak O2 pulse, VE/VCO2, OUES, RER, HRpeak |
| Choi 2018, South Korea | MI | HIIT (21M/2F, 4%) MICT (18M/3F, 5%) | HIIT(53 ± 6.84) MICT (57.31 ± 12.62) | VO2peak |
| Conraads 2015, Belgium Pattyn 2017, Belgium Van De Heyning 2018, Belgium | CAD | HIIT (81M/4F, 15%) MICT (80M/9F, 11%) | HIIT(57 ± 8.8) MICT(59.9 ± 9.2) | SBP, DBP, QoL, FBG, TC, LDL-C, HDL-C, TG, HRpeak, Peak power, HRrest, RER, peak O2 pulse, VO2peak, AT, HRR1min, |
| OUES, VE/VCO2 LVEDD, LVEDV, LVESD, LVESV | ||||
| Currie 2013A, Canada | CAD | HIIT (7M) MICT (7M), Total 39% | HIIT (63 ± 11) MICT (64 ± 6) | VO2peak, AT, peak power, SBP, DBP HRpeak, HRrest, RER |
| Currie 2013B, Canada | CAD | HIIT (10M/1F) MICT(10M/1F), Total 27% | HIIT (62 ± 11) MICT (68 ± 8) | VO2peak, AT, peak power, SBP, DBP HRpeak, HRrest, RER |
| Eser 2020, Switzerland | MI | HIIT (34, 8%) MICT (35, 3%), NR | HIIT (53 ± 12.59) MICT (59 ± 7.41) | SBP, DBP, HRpeak, HRR1min |
| Gao 2015, China | PCI | HIIT (18M/4F) MICT (16M/5F),ND | HIIT (59.4 ± 7.9) MICT (61.2 ± 8) | VO2peak, AT, peak power, LVEF |
| Ghardashi-Afousi 2018, Iran | CABG | HIIT (14M, 22%) MICT (14M, 22%) | HIIT (53.9 ± 3.44) MICT (54.1 ± 4.02) | SBP, DBP, HRpeak, HRrest, LVEF, LVEDD, LVEDV, LVESD, LVESV |
| Jaureguizar 2016, Spain | IHD | HIIT (28M/8F, 8%) MICT (33M/3F, 13%) | HIIT(58 ± 11) MICT (58 ± 11) | SBP, DBP, HRrest, HRR, QoF |
| Jaureguiza 2019, Spain | HIIT (50M/7F) MICT (42M/11F), NR | HIIT (57.6 ± 9.8) MICT (58.3 ± 9.5) | VO2peak, AT, peak power, HRpeak, RER | |
| Keteyian 2014, US | CAD | HIIT (11M/5F, 29%) MICT (12M/1F, 28%) | HIIT(60 ± 7) MICT (58 ± 9) | VO2peak, AT, SBP, DBP, HRrest, HRpeak, HRR1min, RER, VE/VCO2, peak O2 pulse |
| Kim 2015, South Korea | AMI | HIIT(12M/2F, 13%) MICT(10M/4F, 13%) | HIIT(57 ± 11.58) MICT(60.2 ± 13.64) | VO2peak, HRpeak, HRrest, HRR1min, RER, LDL, HDL, TG |
| Moholdt 2009, Norway | CABG | HIIT(24M/4F, 15%) MICT(24M/7F, 11%) | HIIT(60.2 ± 6.9) MICT(62 ± 7.6) | VO2peak, RER, HRR1min, HRrest, QoL, HDL-C, LDL-C, TG, LVEDV, LVESV, LVEF, FBG |
| Moholdt 2012, Norway | MI | HIIT(25M/5F, 18%) MICT(49M/10F, 14%) | HIIT(56.76 ± 10.4) MICT(57.7 ± 69.3) | VO2peak, HRpeak, HRrest, RER, HDL-C, TG, FBG |
| Reed 2021, Canada | CAD | HIIT(36M/7F, 12%) MICT(38M/6F, 18%) | HIIT(61 ± 7) MICT(60 ± 7) | SBP, DBP, QoL |
| Prado 2016, Brazil | CAD | HIIT(14M/3F) MICT(14M/4F), NR | HIIT(56.5 ± 2.7) MICT(61.3 ± 2.2) | VO2peak, AT, RER, HRpeak, OUES, VE/VCO2 |
| Taylor 2020, Australia | CAD | HIIT(39M/7F, 4%) MICT(39M/8F, 9%) | HIIT(65 ± 7) MICT(65 ± 8) | VO2peak, HRpeak, HRrest, RER, peak O2 pulse, OUES, LDL-C, HDL-C, TG, TC, SBP, DBP, QoL, FBG |
| Trachsel 2019, Canada | ACS | HIIT(15M/8F, 38%) MICT(15M/3F, 5%) | HIIT(63.6 ± 9) MICT(59.2 ± 9.7) | VO2peak, OUES, VE/VCO2, peak O2 pulse, peak power, RER, HRpeak, HRR |
| Warburton 2005, Canada | CAD | HIIT(7M) MICT(7M), NR | HIIT(55 ± 7) MICT(57 ± 8) | HRpeak, peak O2 pulse, VE/VCO2, AT |
| Ye 2020, China | Stroke + CAD | HIIT(43M/17F) MICT(40M/20F), ND | HIIT(58.9 ± 5.294) MICT(59 ± 4.643) | VO2peak, AT, peak power, LVEF |
| Outcomes | N | Std.Err | t | p > |t| | 95%CI | Interval |
|---|---|---|---|---|---|---|
| VO2peak | 16 | 0.367 | −1.20 | 0.252 | −1.225 | 0.348 |
| AT | 9 | 0.441 | 1.41 | 0.197 | −0.396 | 1.640 |
| VE/VCO2 | 6 | 0.792 | 0.27 | 0.802 | −1.986 | 2.411 |
| OUES | 5 | 1.526 | 0.19 | 0.864 | −4.572 | 5.141 |
| peak O2 pulse | 6 | 1.113 | 0.08 | 0.943 | −3.006 | 3.176 |
| LVEF | 5 | 1.253 | 2.95 | 0.060 | −0.295 | 7.677 |
| peak power | 7 | 0.524 | −0.92 | 0.400 | −1.831 | 0.865 |
| RER | 13 | 0.458 | −1.26 | 0.233 | −1.586 | 0.430 |
| HRpeak | 15 | 0.461 | 0.07 | 0.946 | −0.964 | 1.028 |
| HRrest | 11 | 0.630 | 0.59 | 0.567 | −1.051 | 1.799 |
| HRR1min | 7 | 2.285 | −0.06 | 0.956 | −6.008 | 5.741 |
| SBP | 10 | 0.465 | 3.67 | 0.006 | 0.635 | 2.779 |
| DBP | 10 | 0.876 | 1.19 | 0.268 | −0.977 | 3.061 |
| HDL-C | 6 | 1.465 | 1.64 | 0.177 | −1.669 | 6.467 |
| LDL-C | 5 | 1.360 | −1.15 | 0.333 | −5.893 | 2.763 |
| TG | 6 | 0.935 | −0.89 | 0.423 | −3.431 | 1.764 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, L.; Zhang, X.; Chen, K.; Ren, X.; Chen, S.; He, Q. Effect of High-Intensity Interval Training on Physical Health in Coronary Artery Disease Patients: A Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Dev. Dis. 2021, 8, 158. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8110158
Du L, Zhang X, Chen K, Ren X, Chen S, He Q. Effect of High-Intensity Interval Training on Physical Health in Coronary Artery Disease Patients: A Meta-Analysis of Randomized Controlled Trials. Journal of Cardiovascular Development and Disease. 2021; 8(11):158. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8110158
Chicago/Turabian StyleDu, Litao, Xianliang Zhang, Ke Chen, Xiaoyu Ren, Si Chen, and Qiang He. 2021. "Effect of High-Intensity Interval Training on Physical Health in Coronary Artery Disease Patients: A Meta-Analysis of Randomized Controlled Trials" Journal of Cardiovascular Development and Disease 8, no. 11: 158. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8110158