
Covid-19 Symptomatic Patients with Oral Lesions: Clinical and Histopathological Study on 123 Cases of the University Hospital Policlinic of Bari with a Purpose of a New Classification


 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- The presence of SARS-CoV-2 confirmed by reverse transcription polymerase chain reaction (RT-PCR) after nasal and oropharyngeal swabs;
- (2)
- Adult patients hospitalized at the University Hospital Policlinic of Bari from October 2020 to December 2020.
- Probably pre-existing conditions: all the para-physiological lesions endemic in the general population;
- SARS-CoV-2-related lesions. The authors considered lesions as virus-related when they appeared together with general symptoms or within one week after the onset of general symptoms and always before the beginning of therapies;
- Treatment-related lesions: lesions that appeared after the start of the Covid-19 specific therapies;
- Lesions mainly related to poor oral hygiene.
3. Results
3.1. Patients Data
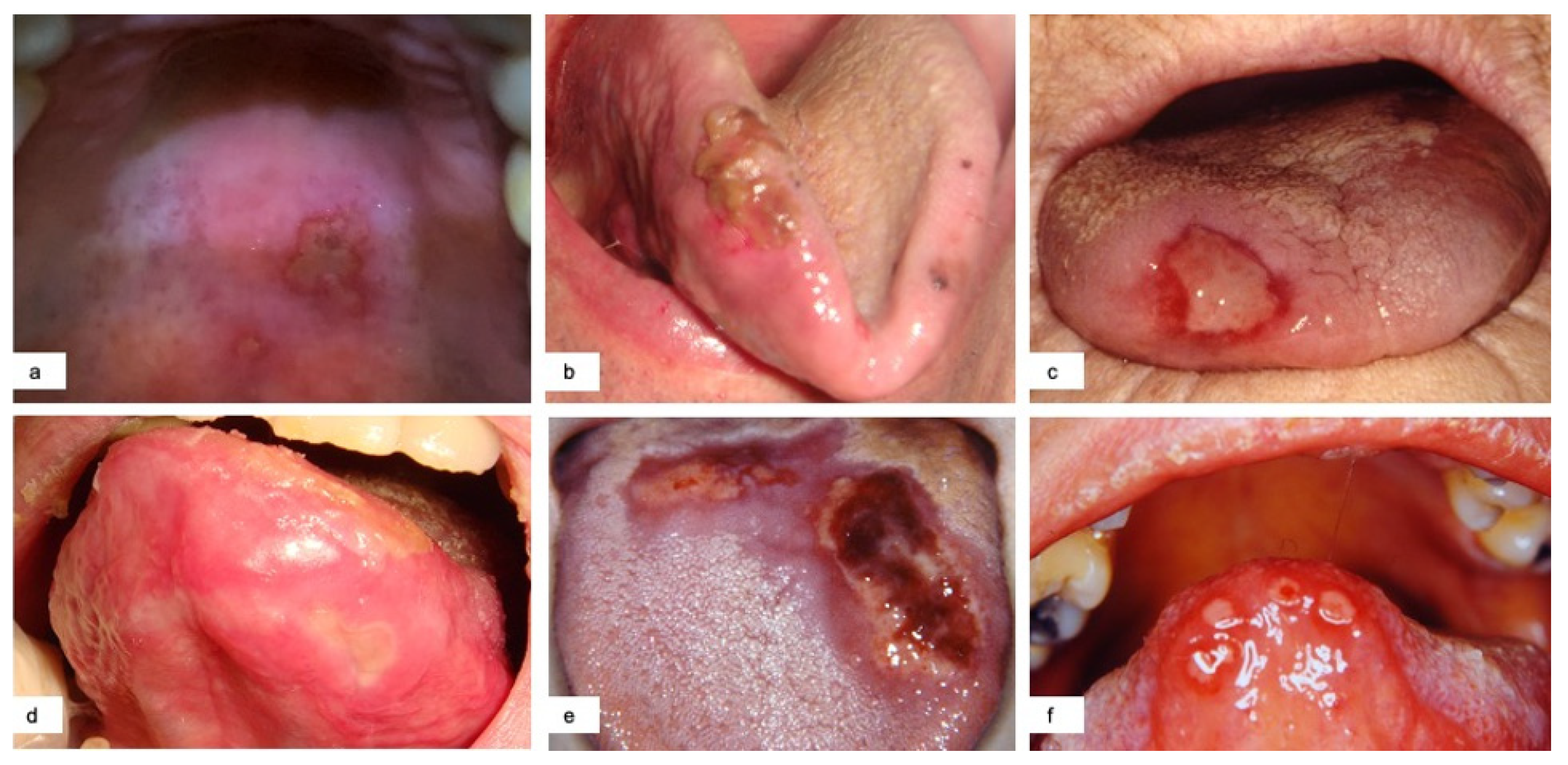
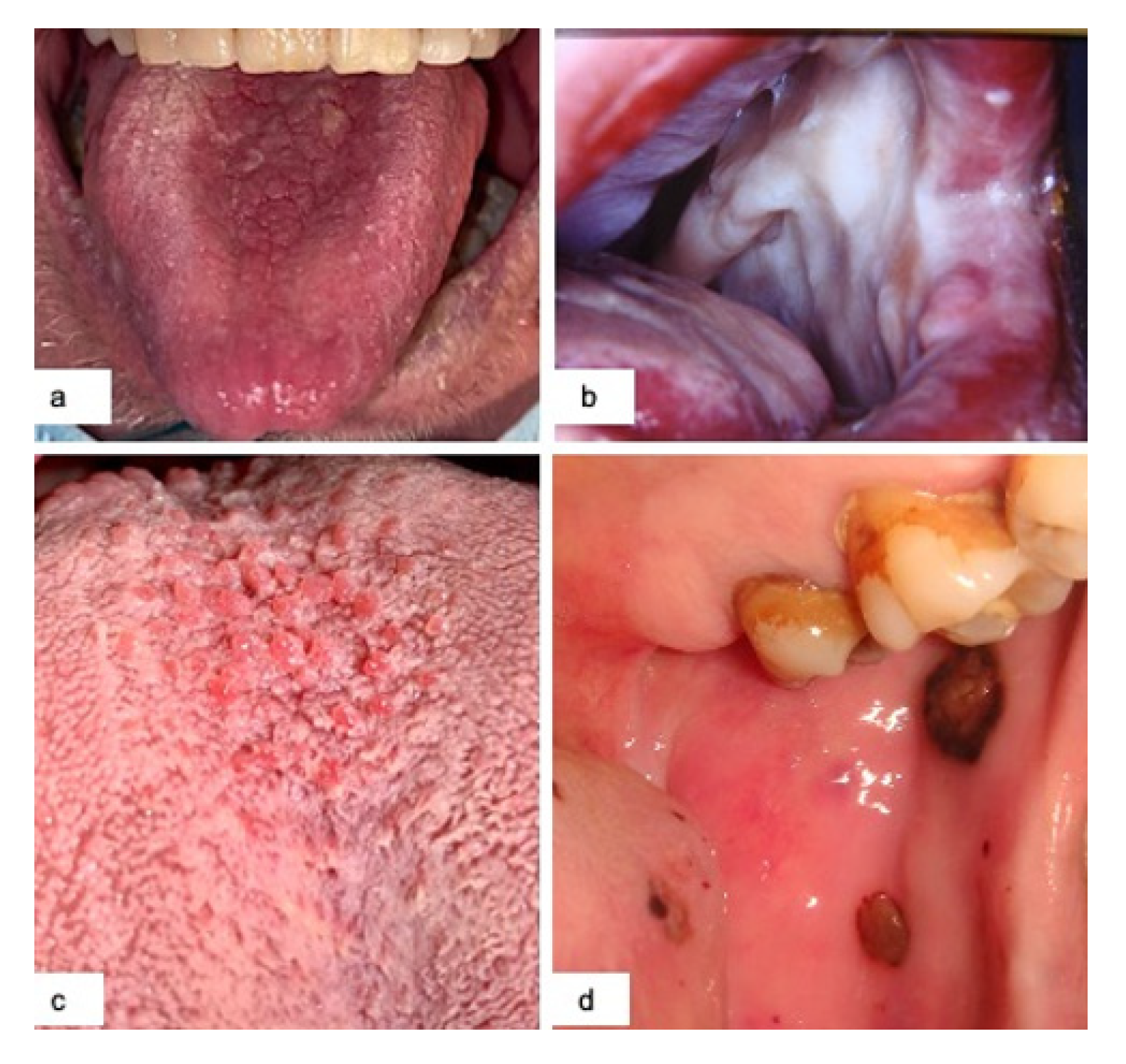
3.2. Oral Manifestations
3.3. Taste Disorders
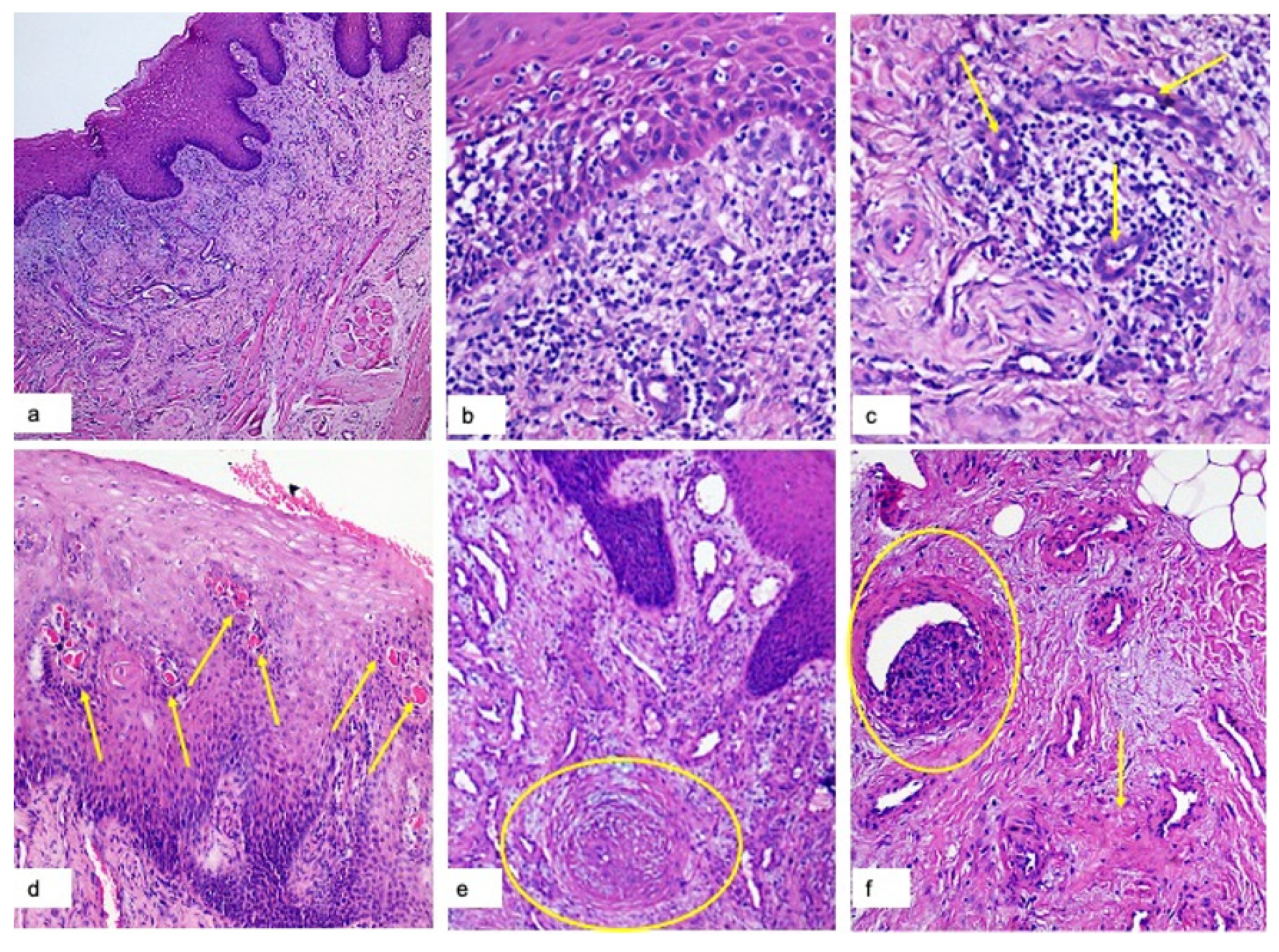
3.4. Histopathological Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization (WHO). Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 20 January 2021).
- Brandão, T.B.; Gueiros, L.A.; Melo, T.S.; Prado-Ribeiro, A.C.; Nesrallah, A.C.F.A.; Prado, G.V.B.; Santos-Silva, A.R.; Migliorati, C.A. Oral lesions in patients with SARS-CoV-2 infection: Could the oral cavity be a target organ? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 131, e45–e51. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Chaux-Bodard, A.G.; Deneuve, S.; Desoutter, A. Oral manifestation of COVID-19 as an inaugural symptom? J. Oral Med. Oral Surg. 2020, 26, 18. [Google Scholar] [CrossRef]
- Amorim Dos Santos, J.; Normando, A.G.C.; Carvalho da Silva, R.L.; de Paula, R.M.; Cembranel, A.C.; Santos-Silva, A.R.; Guerra, E.N.S. Oral mucosal lesions in a COVID-19 patient: New signs or secondary manifestations? Int. J. Infect. Dis. 2020, 97, 326–328. [Google Scholar] [CrossRef]
- Ansari, R.; Gheitani, M.; Heidari, F.; Heidari, F. Oral cavity lesions as a manifestation of the novel virus (COVID-19). Oral Dis. 2020. [CrossRef] [PubMed]
- Cebeci Kahraman, F.; Çaşkurlu, H. Mucosal involvement in a COVID-19-positive patient: A case report. Dermatol. Ther. 2020, 33, e13797. [Google Scholar] [CrossRef]
- Martín Carreras-Presas, C.; Amaro Sánchez, J.; López-Sánchez, A.F.; Jané-Salas, E.; Somacarrera Pérez, M.L. Oral vesiculobullous lesions associated with SARS-CoV-2 infection. Oral Dis. 2020. [CrossRef]
- Putra, B.E.; Adiarto, S.; Dewayanti, S.R.; Juzar, D.A. Viral exanthem with “Spins and needles sensation” on extremities of a COVID-19 patient: A self-reported case from an Indonesian medical frontliner. Int. J. Infect. Dis. 2020, 96, 355–358. [Google Scholar] [CrossRef]
- Cruz Tapia, R.O.; Peraza Labrador, A.J.; Guimaraes, D.M.; Matos Valdez, L.H. Oral mucosal lesions in patients with SARS-CoV-2 infection. Report of four cases. Are they a true sign of COVID-19 disease? Spec. Care Dent. 2020, 40, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, R.; Recalcati, S.; Fantini, F.; Riva, C.; Milani, M.; Dainese, E.; Boggio, F. Histopathological study of a broad spectrum of skin dermatoses in patients affected or highly suspected of infection by COVID-19 in the northern part of italy: Analysis of the many faces of the viral-induced skin diseases in previous and new reported cases. Am. J. Dermatopathol. 2020, 42, 564–570. [Google Scholar] [CrossRef]
- Capodiferro, S.; Tempesta, A.; Bucci, S.; Maiorano, E.; Favia, G.; Limongelli, L. Aminogam® gel allows fasterwound healing after oral surgery by formation of mature connective tissue with low vascular density and reducing inflammatory infiltration. A retrospective study on 580 cases with histological and confocal laser investigation. Appl. Sci. 2020, 10, 1105. [Google Scholar] [CrossRef] [Green Version]
- Casale, M.; Moffa, A.; Vella, P.; Rinaldi, V.; Lopez, M.A.; Grimaldi, V.; Salvinelli, F. Systematic review: The efficacy of topical hyaluronic acid on oral ulcers. J. Biol. Regul. Homeost. Agents 2017, 27, 63–69. [Google Scholar]
- Zhang, L.W.; Fu, J.Y.; Hua, H.; Yan, Z.M. Efficacy and safety of miconazole for oral candidiasis: A systematic review and meta-analysis. Oral Dis. 2016, 22, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Boccio, E.; Hultz, K.; Wong, A.H. Topical tranexamic acid for hemostasis of an oral bleed in a patient on a direct oral anticoagulant. Clin. Pract. Cases Emerg. Med. 2020, 27, 146–149. [Google Scholar] [CrossRef]
- Sameni, F.; Hajikhani, B.; Yaslianifard, S.; Goudarzi, M.; Owlia, P.; Nasiri, M.J.; Shokouhi, S.; Bakhtiyari, M.; Dadashi, M. COVID-19 and skin manifestations: An overview of case reports/case series and meta-analysis of prevalence studies. Front. Med. 2020, 7, 573188, . [Google Scholar] [CrossRef]
- Bemquerer, L.M.; de Arruda, J.A.A.; Soares, M.P.D.; Mesquita, R.A.; Silva, T.A. The oral cavity cannot be forgotten in the COVID-19 era: Is there a connection between dermatologic and oral manifestations? J. Am. Acad. Dermatol. 2020, 83, 1118–1129. [Google Scholar] [CrossRef]
- Amorim Dos Santos, J.; Normando, A.G.C.; Carvalho da Silva, R.L.; Acevedo, A.C.; de Luca Canto, G.; Sugaya, N.; Santos-Silva, A.R.; Guerra, E.N.S. Oral manifestations in patients with COVID-19: A living systematic review. J. Dent. Res. 2021, 100, 141–154. [Google Scholar] [CrossRef]
- Sinadinos, A.; Shelswell, J. Oral ulceration and blistering in patients with COVID-19. Evid. Based Dent. 2020, 21, 49. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Woolley, J. Necrotizing periodontal disease: Oral manifestation of COVID-19. Oral Dis. 2020, 7. [Google Scholar] [CrossRef]
- Iranmanesh, B.; Khalili, M.; Amiri, R.; Zartab, H.; Aflatoonian, M. Oral manifestations of COVID-19 disease: A review article. Dermatol. Ther. 2020, e14578. [Google Scholar] [CrossRef]
- Seirafianpour, F.; Sodagar, S.; Pour Mohammad, A.; Panahi, P.; Mozafarpoor, S.; Almasi, S.; Goodarzi, A. Cutaneous manifestations and considerations in COVID-19 pandemic: A systematic review. Dermatol. Ther. 2020, 33, e13986, . [Google Scholar] [CrossRef]
- Yarom, N.; Cantony, U.; Gorsky, M. Prevalence of fissured tongue, geographic tongue and median rhomboid glossitis among Israeli adults of different ethnic origins. Dermatology 2004, 209, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Form of Covid-19 | N. of Patients | Age (Mean Value) | General Symptoms | Type of Oral Lesions | Oral Symptoms | Day of Appearance | Taste Disorders |
|---|---|---|---|---|---|---|---|
| MODERATE | 95 (77%) | 63 | Fever > 39 °C, anosmia, cough, sore throat, congestion and runny nose, nausea or vomiting, muscle and body aches, dermatologic manifestation, pneumonia |
|
|
| 87% |
| SEVERE | 21 (17%) | 74 | Fever >39 °C, anosmia, cough, sore throat, congestion and runny nose, nausea or vomiting, muscle and body aches, dermatologic manifestation, severe pneumonia, Dyspnea and hypoxia (SpO2 < 90%); severe respiratory distress |
|
|
| 88% |
| CRITICAL | 8 (6%) | 81 | Acute respiratory distress syndrome, multiorgan failure |
| Not possible to achieve |
| 83% |
| Probably Pre-Existing Conditions | Geographic Tongue, Fissured Tongue |
|---|---|
| Sars-CoV-2-related lesions | Early ulcerative lesions, blisters, early erythema multiforme-like lesions, petechiae |
| Treatment-related lesions | Late ulcerative lesions, late erythema multiforme-like lesions, candidiasis, angina bullosa, spontaneous oral hemorrhage, petechiae |
| Lesions related to poor oral hygiene | Ulcero-necrotic gingivitis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favia, G.; Tempesta, A.; Barile, G.; Brienza, N.; Capodiferro, S.; Vestito, M.C.; Crudele, L.; Procacci, V.; Ingravallo, G.; Maiorano, E.; et al. Covid-19 Symptomatic Patients with Oral Lesions: Clinical and Histopathological Study on 123 Cases of the University Hospital Policlinic of Bari with a Purpose of a New Classification. J. Clin. Med. 2021, 10, 757. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10040757
Favia G, Tempesta A, Barile G, Brienza N, Capodiferro S, Vestito MC, Crudele L, Procacci V, Ingravallo G, Maiorano E, et al. Covid-19 Symptomatic Patients with Oral Lesions: Clinical and Histopathological Study on 123 Cases of the University Hospital Policlinic of Bari with a Purpose of a New Classification. Journal of Clinical Medicine. 2021; 10(4):757. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10040757
Chicago/Turabian StyleFavia, Gianfranco, Angela Tempesta, Giuseppe Barile, Nicola Brienza, Saverio Capodiferro, Maria Concetta Vestito, Lucilla Crudele, Vito Procacci, Giuseppe Ingravallo, Eugenio Maiorano, and et al. 2021. "Covid-19 Symptomatic Patients with Oral Lesions: Clinical and Histopathological Study on 123 Cases of the University Hospital Policlinic of Bari with a Purpose of a New Classification" Journal of Clinical Medicine 10, no. 4: 757. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10040757