
Bone Metabolism and RANKL/OPG Ratio in Rheumatoid Arthritis Women Treated with TNF-α Inhibitors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Laboratory Parameters and Evaluation of RA Activity
2.3. Measurement of Bone Turnover Markers
2.4. Measurement of Bone Mineral Density
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
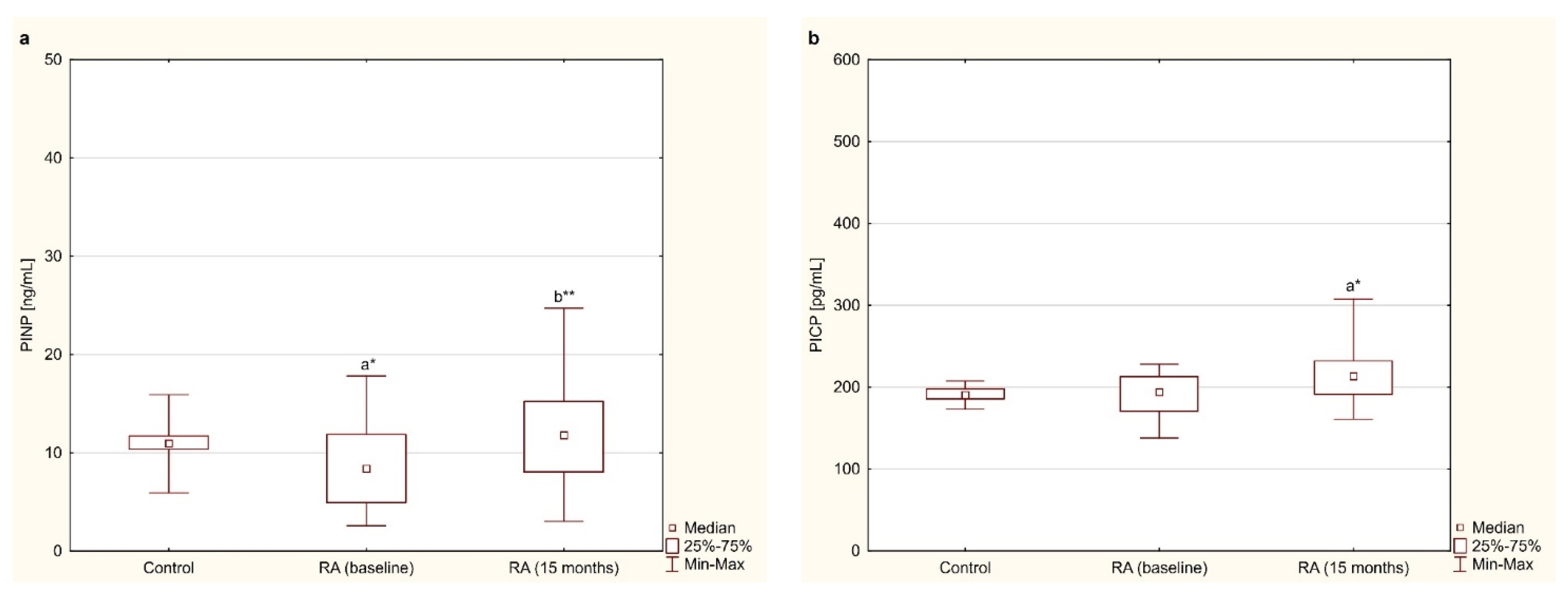
3.2. Bone Formation Markers—PINP and PICP
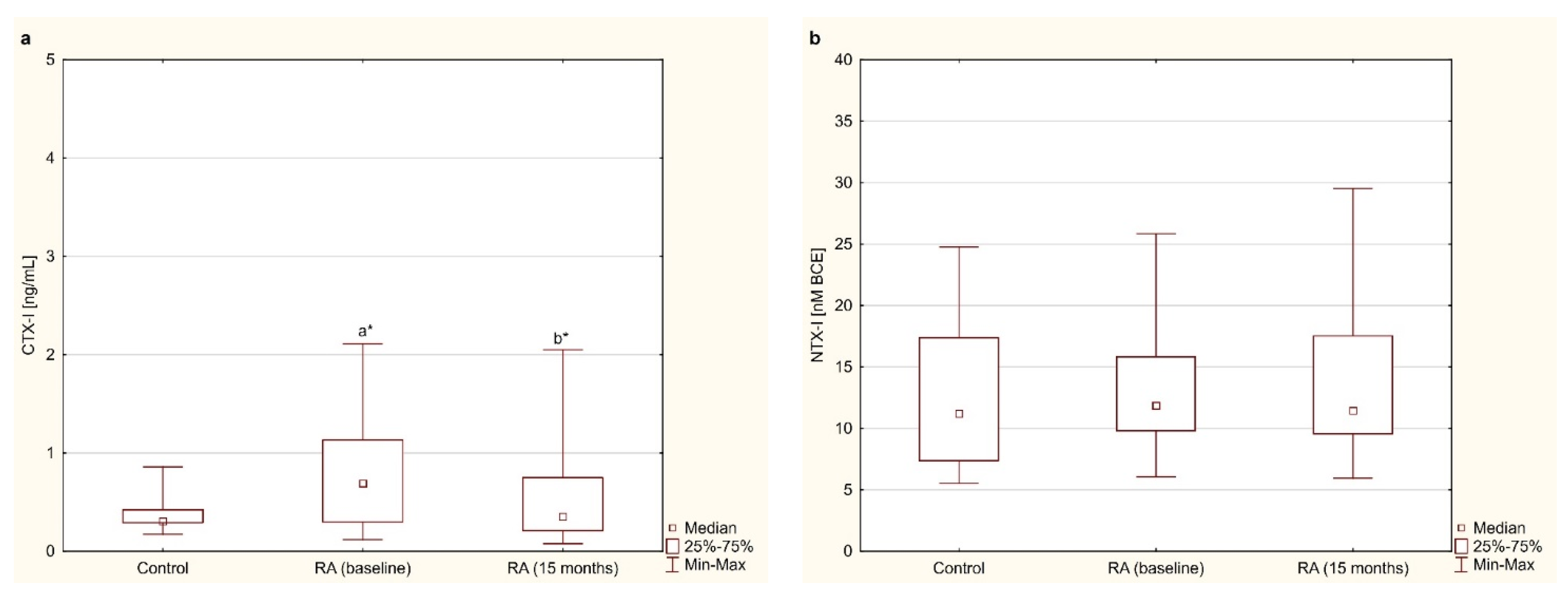
3.3. Bone Resorption Markers—CTX-I and NTX-I
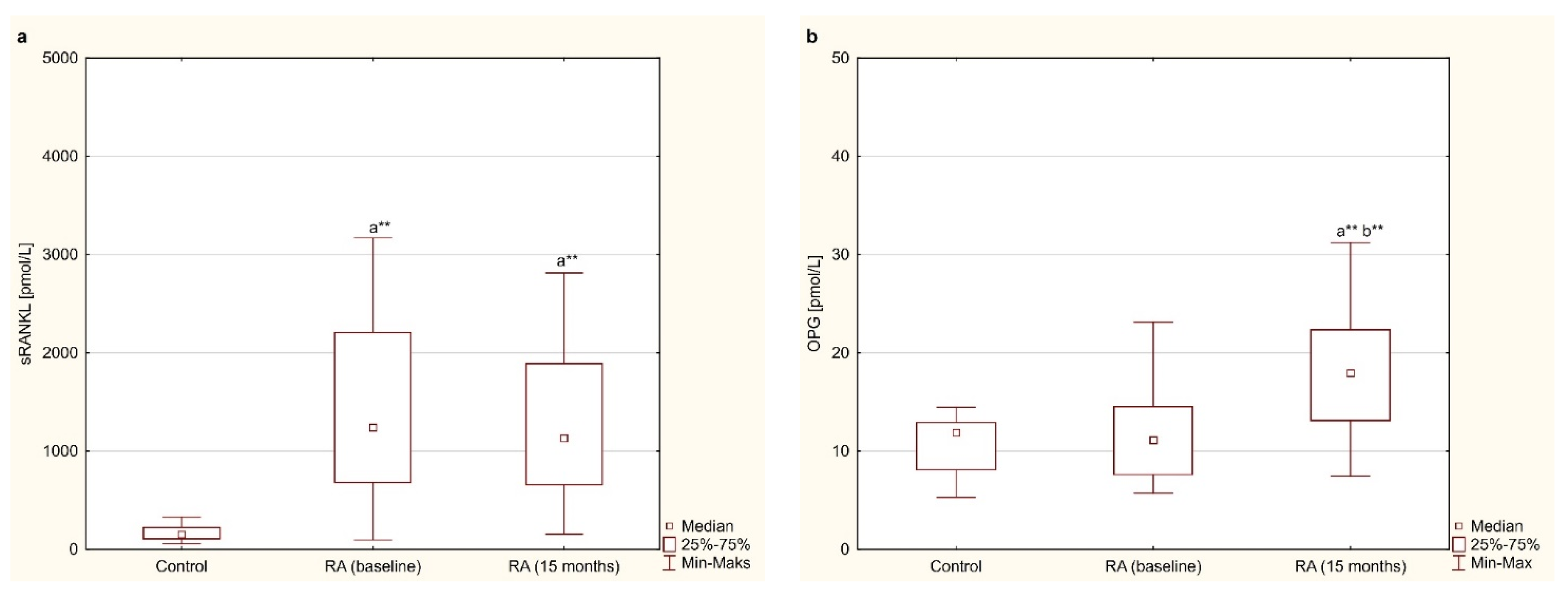
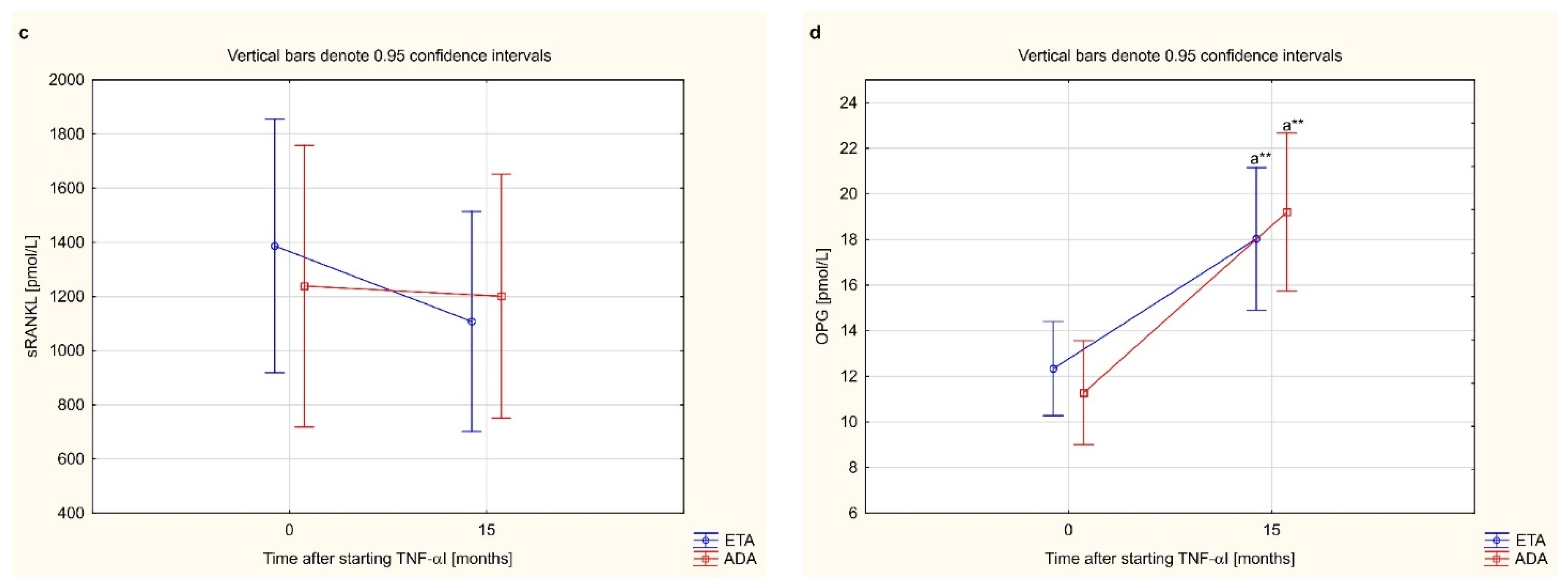
3.4. Osteoclastogenesis Markers—sRANKL and OPG
3.5. Analysis of the Relationship between Bone Turnover Markers, Osteoclastogenesis Markers as Well as Clinical and Laboratory Indicators of Disease Activity
3.6. Effect of Anti-TNF-α Treatment on Bone Mineral Density
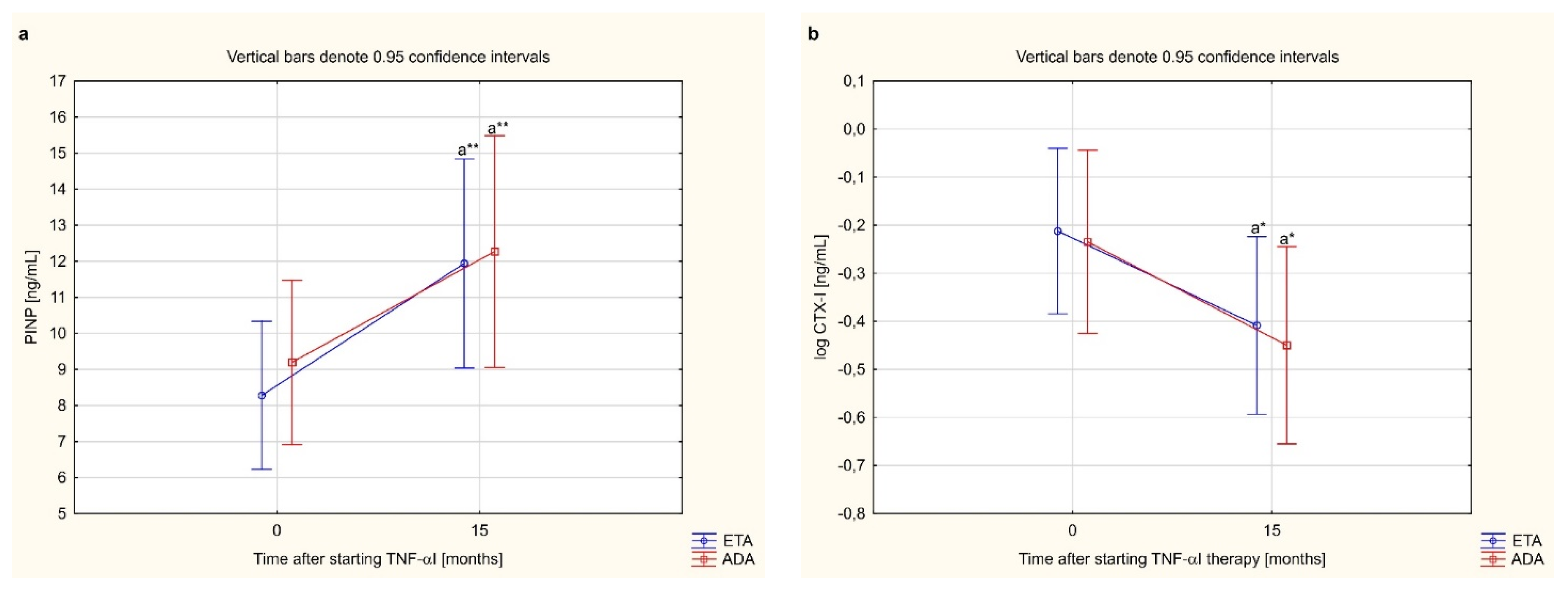
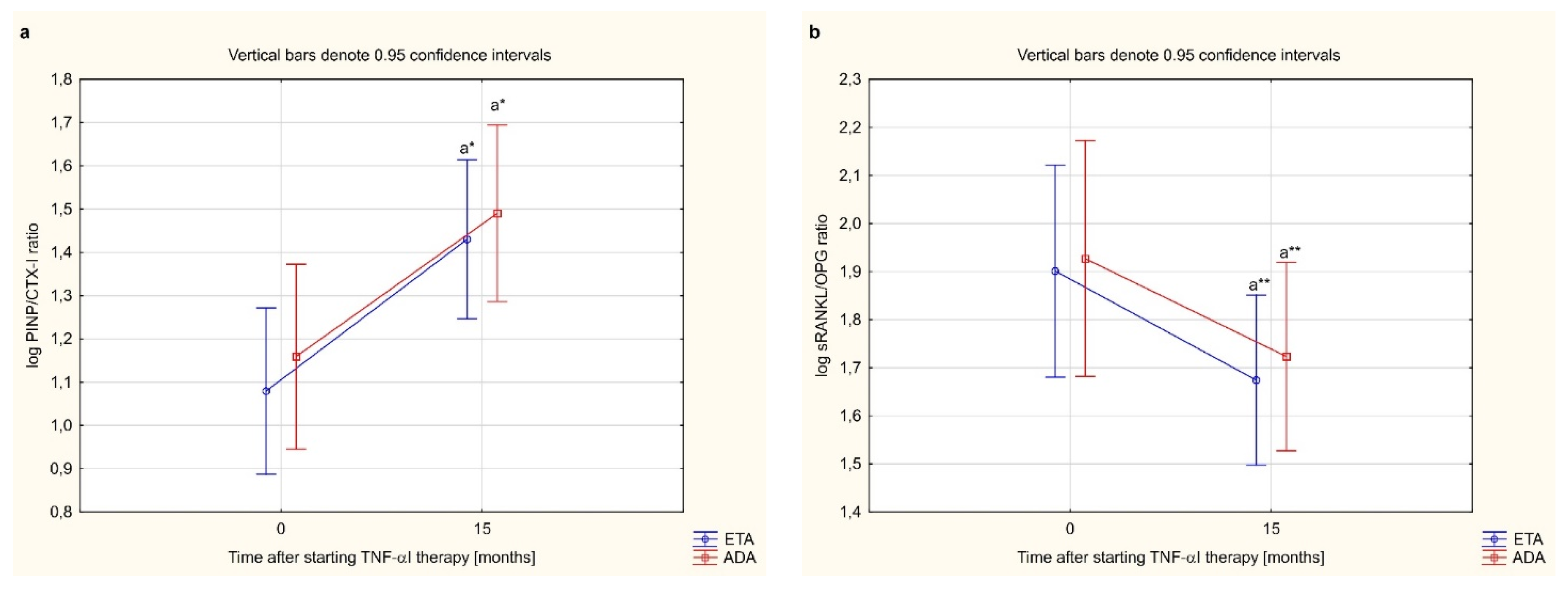
3.7. Bone Metabolism Markers and PINP/CTX-I, sRANKL/OPG Ratios Depending on the Type of TNF-α Inhibitor Used
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coras, R.; Murillo-Saich, J.D.; Guma, M. Circulating pro- and anti-inflammatory metabolites and its potential role in rheumatoid arthritis pathogenesis. Cells 2020, 9, 827. [Google Scholar] [CrossRef] [Green Version]
- Heinlen, L.; Humphrey, M.B. Skeletal complications of rheumatoid arthritis. Osteoporos. Int. 2017, 28, 2801–2812. [Google Scholar] [CrossRef] [PubMed]
- Adami, G.; Saag, K.G. Osteoporosis pathophysiology, epidemiology, and screening in rheumatoid arthritis. Curr. Rheumatol. Rep. 2019, 21, 34. [Google Scholar] [CrossRef] [PubMed]
- Goldring, S.R. Differential mechanisms of de-regulated bone formation in rheumatoid arthritis and spondyloarthritis. Rheumatology 2016, 55, ii56–ii60. [Google Scholar] [CrossRef] [Green Version]
- Sims, N.A.; Martin, T.J. Osteoclasts provide coupling signals to osteoblast lineage cells through multiple mechanisms. Annu. Rev. Physiol. 2020, 82, 507–529. [Google Scholar] [CrossRef] [PubMed]
- Kenkre, J.S.; Bassett, J.H.D. The bone remodelling cycle. Ann. Clin. Biochem. 2018, 55, 308–327. [Google Scholar] [CrossRef] [PubMed]
- Schett, G.; Gravallese, E. Bone erosion in rheumatoid arthritis: Mechanisms, diagnosis and treatment. Nat. Rev. Rheumatol. 2012, 8, 656–664. [Google Scholar] [CrossRef]
- Karmakar, S.; Kay, J.; Gravallese, E.M. Bone damage in rheumatoid arthritis–mechanistic insights and approaches to prevention. Rheum. Dis. Clin. N. Am. 2010, 36, 385–404. [Google Scholar] [CrossRef] [Green Version]
- Walsh, N.C.; Crotti, T.N.; Goldring, S.R.; Gravallese, E.M. Rheumatic diseases: The effects of inflammation on bone. Immunol. Rev. 2005, 208, 228–251. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B. TNF and bone remodeling. Curr. Osteoporos. Rep. 2017, 15, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Tobeiha, M.; Moghadasian, M.H.; Amin, N.; Jafarnejad, S. RANKL/RANK/OPG pathway: A mechanism involved in exercise-induced bone remodeling. BioMed Res. Int. 2020, 19, 6910312. [Google Scholar] [CrossRef] [Green Version]
- Zerbini, C.A.F.; Clark, P.; Mendez-Sanchez, L.; Pereira, R.M.R.; Messina, O.D.; Uña, C.R.; Adachi, J.D.; Lems, W.F.; Cooper, C.; Lane, N.E. Biologic therapies and bone loss in rheumatoid arthritis. Osteoporos. Int. 2017, 28, 429–446. [Google Scholar] [CrossRef]
- Tanaka, S. Regulation of bone destruction in rheumatoid arthritis through RANKL-RANK pathways. World J. Orthop. 2013, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kohli, S.S.; Kohli, V.S. Role of RANKL-RANK/osteoprotegerin molecular complex in bone remodeling and its immunopathologic implications. Indian J. Endocrinol. Metab. 2011, 15, 175–181. [Google Scholar] [CrossRef] [PubMed]
- van Tuyl, L.H.; Voskuyl, A.E.; Boers, M.; Geusens, P.; Landewe, R.B.; Dijkmans, B.A.; Lems, W.F. Baseline RANKL: OPG ratio and markers of bone and cartilage degradation predict annual radiological progression over 11 years in rheumatoid arthritis. Ann. Rheum. Dis. 2010, 69, 1623–1628. [Google Scholar] [CrossRef]
- Gulyás, K.; Horváth, Á.; Végh, E.; Pusztai, A.; Szentpétery, Á.; Pethö, Z.; Váncsa, A.; Bodnár, N.; Csomor, P.; Hamar, A.; et al. Effects of 1-year anti-TNF-α therapies on bone mineral density and bone biomarkers in rheumatoid arthritis and ankylosing spondylitis. Clin. Rheumatol. 2020, 39, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Wijbrandts, C.A.; Klaasen, R.; Dijkgraaf, M.G.W.; Gerlag, D.M.; van Eck-Smit, B.L.F.; Tak, P.P. Bone mineral density in rheumatoid arthritis patients 1 year after adalimumab therapy: Arrest of bone loss. Ann. Rheum. Dis. 2009, 68, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Saidenberg-Kermanac’h, N.; Corrado, A.; Lemeiter, D.; deVernejoul, M.C.; Boissier, M.C.; Cohen-Solal, M.E. TNF-alpha antibodies and osteoprotegerin decrease systemic bone loss associated with inflammation through distinct mechanisms in collagen-induced arthritis. Bone 2004, 35, 1200–1207. [Google Scholar] [CrossRef]
- Morris, H.A.; Eastell, R.; Jorgensen, N.R.; Cavalier, E.; Vasikaran, S.; Chubb, S.A.P.; Kanis, J.A.; Cooper, C.; Makris, K.; IFCC-IOF Working Group for Standardisation of Bone Marker Assays (WG-BMA). Clinical usefulness of bone turnover marker concentrations in osteoporosis. Clin. Chim. Acta 2017, 467, 34–41. [Google Scholar] [CrossRef]
- Chopin, F.; Garnero, P.; le Henanff, A.; Debiais, F.; Daragon, A.; Roux, C.; Sany, J.; Wendling, D.; Zarnitsky, C.; Ravaud, P.T.; et al. Long-term effects of infliximab on bone and cartilage turnover markers in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2008, 67, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Vis, M.; Havaardsholm, E.A.; Haugeberg, G.; Uhlig, T.; Voskuyl, A.E.; van de Stadt, R.J.; Dijkmans, B.A.C.; Woolf, A.D.; Kvien, T.K.; Lems, W.F. Evaluation of bone mineral density, bone metabolism, osteoprotegerin and receptor activator of the NFκB ligand serum levels during treatment with infliximab in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2006, 65, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Torikai, E.; Kageyama, Y.; Takahashi, M.; Suzuki, M.; Ichikawa, T.; Nagafusa, T.; Nagano, A. The effect of infliximab on bone metabolism markers in patients with rheumatoid arthritis. Rheumatology 2006, 45, 761–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perpétuo, I.P.; Caetano-Lopes, J.; Rodrigues, A.M.; Campanilho-Marques, R.; Ponte, C.; Canhão, H.; Ainola, M.; Fonseca, J.E. Effect of tumor necrosis factor inhibitor therapy on osteoclasts precursors in rheumatoid arthritis. BioMed. Res. Int. 2017, 2690402. [Google Scholar] [CrossRef]
- Yasunori, K.; Masaaki, T.; Tetsuyuki, N.; Hayato, K.; Akira, N. Reduction of urinary levels of pyridinoline and deoxypyridinoline and serum levels of soluble receptor activator of NF-kappaB ligand by etanercept in patients with rheumatoid arthritis. Clin. Rheumatol. 2008, 27, 1093–1101. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheuma-tism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef]
- Szeremeta, A.; Jura-Półtorak, A.; Zoń-Giebel, A.; Kopeć-Mędrek, M.; Kucharz, J.E.; Olczyk, K. Aggrecan turnover in women with rheumatoid arthritis treated with TNF-α inhibitors. J. Clin. Med. 2020, 9, 1377. [Google Scholar] [CrossRef]
- Fransen, J.; van Riel, P.L. The Disease activity score and the EULAR response criteria. Rheum. Dis. Clin. N. Am. 2009, 35, 745–757. [Google Scholar] [CrossRef]
- Myasoedova, E.; Crowson, C.S.; Kremers, H.M.; Roger, V.L.; Fitz-Gibbon, P.D.; Therneau, T.M.; Gabriel, S.E. Lipid paradox in rheumatoid arthritis: The impact of serum lipid measures and systemic inflammation on the risk of cardiovascular disease. Ann. Rheum. Dis. 2011, 70, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Konukoglu, D. Bone markers. Int. J. Med. Biochem. 2019, 2, 65–78. [Google Scholar] [CrossRef]
- Civitelli, R.; Armamento-Villareal, R.; Napoli, N. Bone turnover markers: Understanding their value in clinical trials and clinical practice. Osteoporos. Int. 2009, 20, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Patil, S.; Gao, Y.G.; Qian, A. The bone extracellular matrix in bone formation and regeneration. Front. Pharmacol. 2020, 11, 757. [Google Scholar] [CrossRef]
- Fardellone, P.; Séjourné, A.; Paccou, J.; Goëb, V. Bone remodelling markers in rheumatoid arthritis. Mediat. Inflamm. 2014, 2014, 484280. [Google Scholar] [CrossRef]
- Garnero, P.; Landewé, R.; Boers, M.; Verhoeven, A.; Van Der Linden, S.; Christgau, S.; Van Der Heijde, D.; Boonen, A.; Geusens, P. Association of baseline levels of markers of bone and cartilage degradation with long-term progression of joint damage in patients with early rheumatoid arthritis: The COBRA study. Arthritis Rheum. 2002, 46, 2847–2856. [Google Scholar] [CrossRef] [PubMed]
- Wheater, G.; Elshahaly, M.; Naraghi, K.; Tuck, S.P.; Datta, H.K.; van Laar, J.M. Changes in bone density and bone turnover in patients with rheumatoid arthritis treated with rituximab, results from an exploratory, prospective study. PLoS ONE 2018, 13, e0201527. [Google Scholar] [CrossRef]
- Fassio, A.; Adami, G.; Gatti, D.; Orsolini, G.; Giollo, A.; Idolazzi, L.; Benini, C.; Vantaggiato, E.; Rossini, M.; Viapiana, O. Inhibition of tumor necrosis factor-alpha (TNF-alpha) in patients with early rheumatoid arthritis results in acute changes of bone modulators. Int. Immunopharmacol. 2019, 67, 487–489. [Google Scholar] [CrossRef]
- Llorente, I.; García-Castañeda, N.; Valero, C.; González-Álvaro, I.; Castañeda1, S. Osteoporosis in rheumatoid arthritis: Dangerous liaisons. Front. Med. 2020, 7, 601618. [Google Scholar] [CrossRef]
- Marotte, H.; Pallot-Prades, B.; Grange, L.; Gaudin, P.; Alexandre, C.; Miossec, P. A 1-year case-control study in patients with rheumatoid arthritis indicates prevention of loss of bone mineral density in both responders and nonresponders to infliximab. Arthritis Res. Ther. 2007, 9, R61. [Google Scholar] [CrossRef] [Green Version]
- Sponholtz, T.R.; Zhang, X.; Fontes, J.D.; Meigs, J.B.; Cupples, L.A.; Kiel, D.P.; Hannan, M.T.; McLean, R.R. Association between inflammatory biomarkers and bone mineral density in a community-based cohort of men and women. Arthritis Care Res. 2014, 66, 1233–1240. [Google Scholar] [CrossRef]
- Kawai, V.K.; Stein, C.M.; Perrien, D.S.; Griffin, M.R. Effects of anti-tumor necrosis factor α agents on bone. Curr. Opin. Rheumatol. 2012, 24, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Hoff, M.; Kvien, T.K.; Kälvesten, J.; Elden, A.; Haugeberg, G. Adalimumab therapy reduces hand bone loss in early rheumatoid arthritis: Explorative analyses from the PREMIER study. Ann. Rheum. Dis. 2009, 68, 1171–1176. [Google Scholar] [CrossRef]
- Hoff, M.; Kvien, T.K.; Kälvesten, J.; Elden, A.; Kavanaugh, A.; Haugeberg, G. Adalimumab reduces hand bone loss in rheumatoid arthritis independent of clinical response: Subanalysis of the PREMIER study. BMC Musculoskelet. Disord. 2011, 27, 12–54. [Google Scholar] [CrossRef] [Green Version]
- Geusens, P. The role of RANK ligand/osteoprotegerin in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2012, 4, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.N.; Mao, Y.M.; Zhao, C.N.; Wang, H.; Yuan, F.F.; Li, X.M.; Pan, H.F. Circulating levels of osteoprotegerin, osteocalcin and osteopontin in patients with rheumatoid arthritis: A systematic review and meta-analysis. Immunol. Investig. 2019, 48, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Wang, Y.; Lu, J.; Xu, J. Osteoprotegerin and RANKL in the pathogenesis of rheumatoid arthritis-induced osteoporosis. Rheumatol. Int. 2012, 32, 3397–3403. [Google Scholar] [CrossRef]
- Destiani, D.P.; Naja, S.; Dewi, S.; Rahmadi, A.R.; Sulaiman, S.A.S.; Abdulah, R. Efficacy of methotrexate in reducing the risk of bone erosion in patients with rheumatoid arthritis: A systematic review of randomized controlled trials. Osteoporos. Int. 2021, 32, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Ziolkowska, M.; Kurowska, M.; Radzikowska, A.; Luszczykiewicz, G.; Wiland, P.; Dziewczopolski, W.; Filipowicz-Sosnowska, A.; Pazdur, J.; Szechinski, J.; Kowalczewski, J.; et al. High levels of osteoprotegerin and soluble receptor activator of nuclear factor kappa B ligand in serum of rheumatoid arthritis patients and their normalization after anti-tumor necrosis factor alpha treatment. Arthritis Rheum. 2002, 46, 1744–1753. [Google Scholar] [CrossRef]
- Fadda, S.; Hamdy, A.; Abulkhair, E.; Elsify, H.M.; Mostafa, A. Serum levels of osteoprotegerin and RANKL in patients with rheumatoid arthritis and their relation to bone mineral density and disease activity. Egypt. Rheumat. 2015, 37, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Catrina, A.I.; Klint, E.A.; Ernestam, S.; Catrina, S.B.; Makrygiannakis, D.; Botusan, I.R.; Klareskog, L.; Ulfgren, A.K. Anti-tumor necrosis factor therapy increases synovial osteoprotegerin expression in rheumatoid arthritis. Arthritis Rheum. 2006, 54, 76–81. [Google Scholar] [CrossRef]
- Dhooria, A.; Pandurangan, N.; Mahesh, K.V.; Sachdev, S.; Sharma, A.; Sharma, S.; Gupta, N.; Dhir, V. Circulating levels of osteoprotegerin and sRANKL and the effect of methotrexate in patients with rheumatoid arthritis. Indian J. Rheumatol. 2018, 13, 90–94. [Google Scholar]
- González-Alvaro, I.; Ortiz, A.M.; Tomero, E.G.; Balsa, A.; Orte, J.; Laffon, A.; García-Vicuña, R. Baseline serum RANKL levels may serve to predict remission in rheumatoid arthritis patients treated with TNF antagonists. Ann. Rheum. Dis. 2007, 66, 1675–1678. [Google Scholar] [CrossRef] [Green Version]
- Wechalekar, M.D.; Lester, S.; Nagpal, S.; Cole, S.; Das, A.; Hissaria, P.; Crotti, T.; Spargo, L.; Walker, J.G.; Smith, M.D.; et al. THU0070 RANKL, OPG and OSCAR but not Dkk-1 predict radiographic progression in an inception cohort of seropositive rheumatoid arthritis (RA) treated-to-target with combination conventional DMARD therapy. Ann. Rheumat. Dis. 2016, 75, 204. [Google Scholar] [CrossRef]
- Montagnana, M.; Lippi, G.; Danese, E.; Guidi, G.C. The role of osteoprotegerin in cardiovascular disease. Ann. Med. 2013, 45, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Dovio, A.; Allasino, B.; Palmas, E.; Ventura, M.; Pia, A.; Saba, L.; Aroasio, E.; Terzolo, M.; Angeli, A. Increased osteoprotegerin levels in Cushing’s syndrome are associated with an adverse cardiovascular risk profile. J. Clin. Endocrinol. Metab. 2007, 92, 1803–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochette, L.; Meloux, A.; Rigal, E.; Zeller, M.; Cottin, Y.; Vergely, C. The role of osteoprotegerin and its ligands in vascular function. Int. J. Mol. Sci. 2019, 20, 705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasso, G.R.; Florencio-Silva, R.; Simões, R.S.; Baracat, M.C.; Soares Júnior, J.M.; Baracat, E.C. Elevated serum osteoprotegerin levels in women: Friend or foe? Rev. Assoc. Med. Bras. 2015, 61, 524–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.Y.; Peng, Y.Q.; Zhang, H.; Xie, H.; Sheng, Z.F.; Luo, X.H.; Dai, R.C.; Zhou, H.D.; Wu, X.P.; Liao, E.Y. Relationship between serum levels of OPG and TGF-β with decreasing rate of BMD in native Chinese women. Int. J. Endocrinol. 2013, 2013, 727164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannata-Andia, J.B.; Roman-Garcia, P.; Hruska, K. The connections between vascular calcification and bone health. Nephrol. Dial. Transpl. 2011, 26, 3429–3436. [Google Scholar] [CrossRef]
- Chen, J.; Norling, L.V.; Cooper, D. Cardiac dysfunction in rheumatoid arthritis: The role of inflammation. Cells 2021, 10, 881. [Google Scholar] [CrossRef]
- Hansildaar, R.; Vedder, D.; Baniaamam, M.; Tausche, A.K.; Gerritsen, M.; Nurmohamed, M.T. Cardiovascular risk in inflammatory arthritis: Rheumatoid arthritis and gout. Lancet Rheumatol. 2021, 3, e58–e70. [Google Scholar] [CrossRef]
- Nybo, M.; Rasmussen, L.M. The capability of plasma osteoprotegerin as a predictor of cardiovascular disease: A systematic literature review. Eur. J. Endocrinol. 2008, 159, 603–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caidahl, K.; Ueland, T.; Aukrust, P. Osteoprotegerin: A biomarker with many faces. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1684–1686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Campenhout, A.; Golledge, J. Osteoprotegerin, vascular calcification and atherosclerosis. Atherosclerosis 2009, 204, 321–329. [Google Scholar] [CrossRef] [Green Version]
- Tschiderer, L.; Willeit, J.; Schett, G.; Kiechl, S.; Willeit, P. Osteoprotegerin concentration and risk of cardiovascular outcomes in nine general population studies: Literature-based meta-analysis involving 26,442 participants. PLoS ONE 2017, 12, e0183910. [Google Scholar] [CrossRef] [Green Version]
- Callegari, A.; Coons, M.L.; Ricks, J.L.; Rosenfeld, M.E.; Scatena, M. Increased calcification in osteoprotegerin-deficient smooth muscle cells: Dependence on receptor activator of NF-κB ligand and interleukin 6. J. Vasc. Res. 2014, 51, 118–131. [Google Scholar] [CrossRef] [Green Version]
- Fardellone, P.; Salawati, E.; Le Monnier, L.; Goëb, V. Bone loss, osteoporosis, and fractures in patients with rheumatoid arthritis: A review. J. Clin. Med. 2020, 20, 3361. [Google Scholar] [CrossRef]
- Li, P.; Schwarz, E.M.; O’Keefe, R.J.; Ma, L.; Looney, R.J.; Ritchlin, C.T.; Boyce, B.F.; Xing, L. Systemic tumor necrosis factor α mediates an increase in peripheral CD11bhigh osteoclast precursors in tumor necrosis factor α–transgenic mice. Arthritis Rheum. 2004, 50, 265–276. [Google Scholar] [CrossRef]
- Tanaka, S. Emerging anti-osteoclast therapy for rheumatoid arthritis. J. Orthop. Sci. 2018, 23, 717–721. [Google Scholar] [CrossRef]
- Ritchlin, C.T.; Haas-Smith, S.A.; Li, P.; Hicks, D.G.; Schwarz, E.M. Mechanisms of TNF-α- and RANKL-mediated osteoclastogenesis and bone resorption in psoriatic arthritis. J. Clin. Investig. 2003, 111, 821–831. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years) | 47.52 ± 11.91 |
| Disease duration (years) | 6 (3–12) |
| Height (cm) | 163.58 ± 6.78 |
| Weight (kg) | 65.52 ± 14.40 |
| BMI (kg/m2) | 24.46 ± 5.17 |
| IgM-RF (+), n (%) | 44 (88) |
| Anti-CCP (+), n (%) | 43 (86) |
| ESR (mm/h) | 17.0 (10.0–29.0) |
| CRP (mg/L) | 6.37 (3.0–10.30) |
| SJC, n | 7 (5–10) |
| TJC, n | 12 (9–14) |
| VAS, (0–100 mm) | 80 (70–80) |
| DAS 28-ESR | 5.83 ± 0.49 |
| Anti-rheumatic drugs, n (%) | |
| MTX (25 mg/week) | 50 (100) |
| GC (≤7.5 mg/day) | 50 (100) |
| FA (5 mg/day) | 50 (100) |
| Calcium (1 g/day) | 50 (100) |
| 25-OH vitamin D (800–1000 IU/day) | 50 (100) |
| TNFαI therapy, n (%) | |
| ETA (Enbrel) | 24 (48) |
| ADA (Humira) | 22 (44) |
| CZP (Cimzia) | 2 (4) |
| GLM (Simponi) | 2 (4) |
| Parameter | Value |
|---|---|
| Age (years) | 46.12 ± 10.91 |
| Height (cm) | 166.64 ± 6.23 |
| Weight (kg) | 62.64 ± 8.46 |
| BMI (kg/m2) | 22.64 ± 2.26 |
| ESR (mm/h) | 9.00 (8.00–12.00) |
| RBC (106/μL) | 4.28 ± 0.23 |
| Hb (g/dL) | 13.08 ± 0.97 |
| Ht (%) | 38.68 ± 3.10 |
| PLT (103/μL) | 263.88 ± 49.43 |
| WBC (103/μL) | 8.16 ± 1.63 |
| Glucose (mg/dL) | 88.00 (86.00–95.00) |
| Total cholesterol (mg/dL) | 181.08 ± 6.02 |
| HDL-C (mg/dL) | 59.51 ± 12.85 |
| LDL-C (mg/dL) | 95.44 ± 20.19 |
| Triglycerides (mg/dL) | 118,70 (91.90–149.70) |
| hsCRP (mg/L) | 0.61 (0.40–2.81) |
| Creatinine (mg/dL) | 0.86 ± 0.10 |
| Calcium C (mmol/L) | 2.27 ± 0,08 |
| Phosphorus (mmol/L) | 1.34 ± 0.25 |
| ALP (U/L) | 159.77 ± 25.18 |
| ALT (U/L) | 20.61 ± 8.35 |
| ASP (U/L) | 20.00 ± 4.55 |
| TSH (mU/L) | 2.4 (2.20–2.81) |
| Uric acid (mg/dL) | 4.70 ± 0.70 |
| Parameter | Time after Initiation of TNFαI Therapy | |||
|---|---|---|---|---|
| Baseline (T0) | 3 Months (T1) | 9 Months (T2) | 15 Months (T3) | |
| Women with RA, n (%) | 31 (100) | |||
| Premenopausal females, n (%) | 17 (54.84) | |||
| Postmenopausal females, n (%) | 14 (45.16) | |||
| Age (years) | 45.87 ± 12.28 | |||
| Disease duration (years) | 5 (3–11) | |||
| Growth (cm) | 163.77 ± 6.63 | |||
| Weight (kg) | 65.89 ± 14.60 | |||
| BMI (kg/m2) | 24.62 ± 5.65 | |||
| IgM-RF (+), n (%) | 28 (90.32) | |||
| Anti-CCP (+), n (%) | 26 (83.87) | |||
| ESR (mm/h) | 17.0 (10.0–34.0) | 14.0 (9.0–23.0) | 13.0 (9.0–18.0) a | 13.0 (8.0–18.0) a |
| CRP (mg/L) | 6.3 (3.08–14.0) | 4.0 (2.0–9.0) | 4.0 (2.0–4.3) a | 4.0 (1.5–5.1) a |
| Calcium C (mmol/L) | 2.30 ± 0.11 | 2.31 ± 0.11 | ||
| Phosphorus (mmol/L) | 1.36 ± 0.20 | 1.37 ± 0.21 | ||
| ALP (U/L) | 168.5 (152.5–202) | 165.5 (149.5–192) | ||
| SJC, n | 7 (5–10) | 2 (0–3) a,c | 0 (0–0) a,b | 0 (0–0) a,b |
| TJC, n | 12 (9–16) | 4 (2–7) a,c | 1 (0–2) a,b | 0 (0–0) a,b,c |
| VAS, (0–100 mm) | 80 (80–80) | 40 (30–50) a,c | 20 (10–30) a,b | 15 (5–20) a,b |
| DAS 28-ESR | 5.78 (5.51–6.24) | 3.92 (3.08–4.42) a,c | 2.75 (2.24–3.13) a,b | 2.19 (1.75–2.51) a,b,c |
| Disease activity, n (%) | ||||
| High (>5.1) | 31 (100) | 2 (6.45) | 0 (0) | 0 (0) |
| Moderate (>3.2 and ≤5.1) | 0 (0) | 20 (64.52) | 3 (9.68) | 0 (0) |
| Low (≤3.2 and >2.6) | 0 (0) | 4 (12.91) | 14 (45.16) | 5 (16.13) |
| Remission (≤2.6) | 0 (0) | 5 (16.13) | 14 (45.16) | 26 (83.87) |
| Lumbar L2-L4 BMD (g/cm3) | 0.89 (0.73–1.00) | 0.92 (0.79–1.03) | ||
| Lumbar L2-L4 T-score | −2.05 (−2.93–0.32) | −1.70 (−2.75–-0.65) | ||
| Lumbar L2-L4 Z-score | −1.43 (−2.38–0.23) | −1.15 (−2.00–0.15) | ||
| Neck femur BMD (g/cm3) | 0.83 (0.69–0.78) | 0.85 (0.77–0.85) | ||
| Neck femur T-score | −0.30 (−1.30–0.40) | −0.30 (−1.8–0.50) | ||
| Neck femur Z-score | −0.10 (−0.90–0.10) | 0.00 (−0.70–0.10) | ||
| Patients which responded to TNFαI therapy, n (%) | ||||
| ETA (Enbrel) | 16 (51.62) | |||
| ADA (Humira) | 13 (41.93) | |||
| CZP (Cimzia) | 2 (6.45) | |||
| Parameter | Healthy Subjects | RA Patients (n = 31) | p | |||
|---|---|---|---|---|---|---|
| Time after Initiation of TNFαI Therapy | ||||||
| A | Baseline (T0) B | 15 Months (T3) C | A vs. B | A vs. C | B vs. C | |
| PINP/CTX-I ratio | 33.79 (25.15–48.31) | 12.30 (6.69–20.20) | 30.74 (14.51–50.06) | <0.001 | NS | <0.001 |
| sRANKL/OPG ratio | 14.77 (10.20–23.97) | 107.21 (39.20–190.12) | 52.87 (34.25–94.28) | <0.001 | <0.001 | <0.001 |
| Parameter | RA Patients (n = 31) Time after Initiation of TNFαI Therapy | |||||
|---|---|---|---|---|---|---|
| Baseline (T0) | ||||||
| PINP | CTX-I | PINP/CTX-I | sRANKL | OPG | sRANKL/OPG | |
| CRP | −0.167 NS | −0.216 NS | 0.03 NS | 0.238 NS | −0.05 NS | 0.302 NS |
| ESR | 0.044 NS | −0.075 NS | 0.213 NS | 0.247 NS | 0.233 NS | 0.176 NS |
| DAS28-ESR | 0.012 NS | −0.216 NS | 0.132 NS | −0.221 NS | 0.07 NS | −0.207 NS |
| SJC | −0.130 NS | −0.223 NS | 0.068 NS | −0.307 NS | 0.001 NS | −0.305 NS |
| TJC | −0.027 NS | 0.0245 NS | −0.088 NS | −0.044 NS | −0.236 NS | −0.320 NS |
| VAS | 0.105 NS | 0.146 NS | −0.097 NS | −0.047 NS | 0.101 NS | −0.160 NS |
| 15 Months (T3) | ||||||
| CRP | −0.08 NS | 0.319 NS | −0.333 NS | −0.03 NS | −0.128 NS | 0.059 NS |
| ESR | 0.202 NS | 0.067 NS | 0.145 NS | 0.169 NS | 0.285 NS | 0.091 NS |
| DAS28-ESR | 0.185 NS | 0.112 NS | 0.054 NS | 0.193 NS | 0.255 NS | 0.077 NS |
| SJC | 0.353 NS | 0.085 NS | 0.097 NS | 0.000 NS | −0.036 NS | 0.012 NS |
| TJC | −0.028 NS | −0.028 NS | 0.0176 NS | 0.097 NS | −0.214 NS | 0.051 NS |
| VAS | 0.082 NS | 0.040 NS | −0.047 NS | 0.071 NS | 0.322 NS | −0.091 NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jura-Półtorak, A.; Szeremeta, A.; Olczyk, K.; Zoń-Giebel, A.; Komosińska-Vassev, K. Bone Metabolism and RANKL/OPG Ratio in Rheumatoid Arthritis Women Treated with TNF-α Inhibitors. J. Clin. Med. 2021, 10, 2905. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10132905
Jura-Półtorak A, Szeremeta A, Olczyk K, Zoń-Giebel A, Komosińska-Vassev K. Bone Metabolism and RANKL/OPG Ratio in Rheumatoid Arthritis Women Treated with TNF-α Inhibitors. Journal of Clinical Medicine. 2021; 10(13):2905. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10132905
Chicago/Turabian StyleJura-Półtorak, Agnieszka, Anna Szeremeta, Krystyna Olczyk, Aleksandra Zoń-Giebel, and Katarzyna Komosińska-Vassev. 2021. "Bone Metabolism and RANKL/OPG Ratio in Rheumatoid Arthritis Women Treated with TNF-α Inhibitors" Journal of Clinical Medicine 10, no. 13: 2905. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10132905