
Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis


 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marks, M.; O’Hara, G.; Houlihan, C.; Bell, L.; Heightman, M.; Hart, N. Severe acute respiratory syndrome coronavirus 2. Ref. Modul. Biomed. Sci. 2021, 231–242. [Google Scholar] [CrossRef]
- Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive value of comorbid conditions for COVID-19 mortality. J. Clin. Med. 2021, 10, 2652. [Google Scholar] [CrossRef]
- Yu, D.; Du, Q.; Yan, S.; Guo, X.-G.; He, Y.; Zhu, G.; Zhao, K.; Ouyang, S. Liver injury in COVID-19: Clinical features and treatment management. Virol. J. 2021, 18, 121. [Google Scholar] [CrossRef]
- Cerbu, B.; Pantea, S.; Bratosin, F.; Vidican, I.; Turaiche, M.; Frent, S.; Borsi, E.; Marincu, I. Liver impairment and hematological changes in patients with chronic hepatitis C and COVID-19: A retrospective study after one year of pandemic. Medicina 2021, 57, 597. [Google Scholar] [CrossRef]
- Łykowska-Szuber, L.; Wołodźko, K.; Rychter, A.M.; Szymczak-Tomczak, A.; Krela-Kaźmierczak, I.; Dobrowolska, A. Liver injury in patients with coronavirus disease 2019 (COVID-19)—A narrative review. J. Clin. Med. 2021, 10, 5048. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Hepatitis C. In ECDC Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Negro, F. Epidemiology of hepatitis C in Europe. Dig. Liver Dis. 2014, 46, S158–S164. [Google Scholar] [CrossRef]
- Maticic, M.; Lombardi, A.; Mondelli, M.U.; Colombo, M. Elimination of hepatitis C in Europe: Can WHO targets be achieved? Clin. Microbiol. Infect. 2020, 26, 818–823. [Google Scholar] [CrossRef]
- Guerra, J.V.S.; Dias, M.M.G.; Brilhante, A.J.V.C.; Terra, M.F.; García-Arévalo, M.; Figueira, A.C.M. Multifactorial basis and therapeutic strategies in metabolism-related diseases. Nutrients 2021, 13, 2830. [Google Scholar] [CrossRef]
- Kukla, M.; Skonieczna-Żydecka, K.; Kotfis, K.; Maciejewska, D.; Łoniewski, I.; Lara, L.F.; Pazgan-Simon, M.; Stachowska, E.; Kaczmarczyk, M.; Koulaouzidis, A.; et al. COVID-19, MERS and SARS with concomitant liver injury—Systematic review of the existing literature. J. Clin. Med. 2020, 9, 1420. [Google Scholar] [CrossRef]
- McGrowder, D.A.; Miller, F.; Anderson Cross, M.; Anderson-Jackson, L.; Bryan, S.; Dilworth, L. Abnormal liver biochemistry tests and acute liver injury in COVID-19 patients: Current evidence and potential pathogenesis. Diseases 2021, 9, 50. [Google Scholar] [CrossRef]
- Butaru, A.E.; Gheonea, D.I.; Rogoveanu, I.; Diculescu, M.; Boicea, A.-R.; Bunescu, M.; Streba, C.-T.; Oancea, C.N. Micro-elimination: Updated pathway to global elimination of hepatitis C in small communities and industrial settings during the COVID 19 pandemic. J. Clin. Med. 2021, 10, 4976. [Google Scholar] [CrossRef]
- Papic, N.; Radmanic, L.; Dusek, D.; Kurelac, I.; Lepej, S.Z.; Vince, A. Trends of late presentation to care in patients with chronic hepatitis C during a 10-year period in Croatia. Infect. Dis. Rep. 2020, 12, 74–81. [Google Scholar] [CrossRef]
- Rullier, A.; Trimoulet, P.; Urbaniak, R.; Winnock, M.; Zauli, D.; Ballardini, G.; Rosenbaum, J.; Balabaud, C.; Bioulac-Sage, P.; Le Bail, B. Immunohistochemical detection of HCV in cirrhosis, dysplastic nodules, and hepatocellular carcinomas with parallel-tissue quantitative RT-PCR. Mod. Pathol. 2001, 14, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y.; Dungubat, E.; Kusano, H.; Ganbat, D.; Tomita, Y.; Odgerel, S.; Fukusato, T. Application of immunohistochemistry in the pathological diagnosis of liver tumors. Int. J. Mol. Sci. 2021, 22, 5780. [Google Scholar] [CrossRef]
- Sahin, A.; Artas, H.; Tunc, N.; Yalniz, M.; Bahcecioglu, I.H. Hematological indices in portal hypertension: Cirrhosis versus noncirrhotic portal hypertension. J. Clin. Med. 2018, 7, 196. [Google Scholar] [CrossRef] [Green Version]
- Galsgaard, K.D. The vicious circle of hepatic glucagon resistance in non-alcoholic fatty liver disease. J. Clin. Med. 2020, 9, 4049. [Google Scholar] [CrossRef]
- Kotlyarov, S.; Bulgakov, A. Lipid metabolism disorders in the comorbid course of nonalcoholic fatty liver disease and chronic obstructive pulmonary disease. Cells 2021, 10, 2978. [Google Scholar] [CrossRef]
- Di Costanzo, A.; Ronca, A.; D’Erasmo, L.; Manfredini, M.; Baratta, F.; Pastori, D.; Di Martino, M.; Ceci, F.; Angelico, F.; Del Ben, M.; et al. HDL-mediated cholesterol efflux and plasma loading capacities are altered in subjects with metabolically—But not genetically driven non-alcoholic fatty liver disease (NAFLD). Biomedicines 2020, 8, 625. [Google Scholar] [CrossRef]
- Ismail, I.T.; Elfert, A.; Helal, M.; Salama, I.; El-Said, H.; Fiehn, O. Remodeling lipids in the transition from chronic liver disease to hepatocellular carcinoma. Cancers 2021, 13, 88. [Google Scholar] [CrossRef]
- Garcia-Compean, D.; Jaquez-Quintana, J.O.; Gonzalez-Gonzalez, J.A.; Maldonado-Garza, H.J. Liver cirrhosis and diabetes: Risk factors, pathophysiology, clinical implications and management. World J. Gastroenterol. 2009, 15, 280–288. [Google Scholar] [CrossRef]
- Coman, L.I.; Coman, O.A.; Bădărău, I.A.; Păunescu, H.; Ciocîrlan, M. Association between liver cirrhosis and diabetes mellitus: A review on hepatic outcomes. J. Clin. Med. 2021, 10, 262. [Google Scholar] [CrossRef]
- Miarka, M.; Gibiński, K.; Janik, M.K.; Główczyńska, R.; Zając, K.; Pacho, R.; Raszeja-Wyszomirska, J. Sarcopenia—The impact on physical capacity of liver transplant patients. Life 2021, 11, 740. [Google Scholar] [CrossRef]
- Nishikawa, H.; Fukunishi, S.; Asai, A.; Nishiguchi, S.; Higuchi, K. Sarcopenia and frailty in liver cirrhosis. Life 2021, 11, 399. [Google Scholar] [CrossRef]
- Vrachatis, D.A.; Papathanasiou, K.A.; Giotaki, S.G.; Raisakis, K.; Kossyvakis, C.; Kaoukis, A.; Kolokathis, F.; Deftereos, G.; Iliodromitis, K.E.; Avramides, D.; et al. Immunologic dysregulation and hypercoagulability as a pathophysiologic background in COVID-19 infection and the immunomodulating role of colchicine. J. Clin. Med. 2021, 10, 5128. [Google Scholar] [CrossRef]
- Di Micco, P.; Russo, V.; Carannante, N.; Imparato, M.; Cardillo, G.; Lodigiani, C. Prognostic value of fibrinogen among COVID-19 patients admitted to an emergency department: An Italian cohort study. J. Clin. Med. 2020, 9, 4134. [Google Scholar] [CrossRef]
- Gambino, C.; Piano, S.; Angeli, P. Acute-on-chronic liver failure in cirrhosis. J. Clin. Med. 2021, 10, 4406. [Google Scholar] [CrossRef]
- Morgan, K.; Samuel, K.; Vandeputte, M.; Hayes, P.C.; Plevris, J.N. SARS-CoV-2 infection and the liver. Pathogens 2020, 9, 430. [Google Scholar] [CrossRef]
- Foglia, B.; Novo, E.; Protopapa, F.; Maggiora, M.; Bocca, C.; Cannito, S.; Parola, M. Hypoxia, hypoxia-inducible factors and liver fibrosis. Cells 2021, 10, 1764. [Google Scholar] [CrossRef]
- Charalabopoulos, K.; Peschos, D.; Zoganas, L.; Bablekos, G.; Golias, C.; Charalabopoulos, A.; Stagikas, D.; Karakosta, A.; Papathanasopoulos, A.; Karachalios, G.; et al. Alterations in arterial blood parameters in patients with liver cirrhosis and ascites. Int. J. Med. Sci. 2007, 4, 94–97. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics * | COVID (n = 46) | Non-COVID (n = 196) | p-Value ** |
|---|---|---|---|
| Age, years | 0.291 | ||
| 18–65 | 34 (73.9%) | 129 (65.8%) | |
| >65 | 12 (26.1%) | 67 (34.2%) | |
| Sex | 0.751 | ||
| Men | 27 (58.7%) | 110 (56.1%) | |
| Women | 19 (41.3%) | 86 (43.9%) | |
| BMI (mean ± SD) | 20.2 ± 2.1 | 21.4 ± 3.7 | 0.035¶ |
| Underweight (<18.5 kg/m2) | 15 (32.6%) | 37 (18.8%) | 0.041 |
| Medical Background | |||
| Chronic alcohol consumption | 16 (34.8%) | 61 (31.1%) | 0.631 |
| History of hepatitis A infection | 7 (15.2%) | 19 (9.7%) | 0.276 |
| Cardiovascular disease | 28 (60.9%) | 125 (63.8%) | 0.712 |
| Metabolic disease | 11 (23.9%) | 51 (26.0%) | 0.768 |
| Cerebrovascular disease | 11 (23.9%) | 47 (23.9%) | 0.992 |
| Chronic kidney disease | 9 (19.6%) | 40 (20.4%) | 0.898 |
| Malignancy | 6 (13.0%) | 31 (15.8%) | 0.638 |
| Cirrhosis complications | |||
| Jaundice | 13 (28.2%) | 48 (24.5%) | 0.596 |
| Portal hypertension | 28 (60.9%) | 103 (52.6%) | 0.308 |
| Upper gastrointestinal bleeding | 19 (41.3%) | 68 (34.7%) | 0.400 |
| Hepatic encephalopathy | 25 (54.3%) | 71 (36.2%) | 0.023 |
| Gastritis | 27 (58.7%) | 99 (50.5%) | 0.317 |
| Pleural effusion | 7 (15.2%) | 33 (16.8%) | 0.790 |
| Ascites | 19 (41.3%) | 67 (34.2%) | 0.363 |
| Spontaneous bacterial peritonitis | 4 (8.7%) | 8 (4.1%) | 0.194 |
| Hepatorenal syndrome | 4 (8.7%) | 7 (3.6%) | 0.133 |
| Child–Pugh | 0.542 | ||
| A | 26 (56.5%) | 115 (58.7%) | |
| B | 13 (28.2%) | 42 (21.4%) | |
| C | 7 (15.2%) | 39 (19.9%) | |
| Disease outcomes | |||
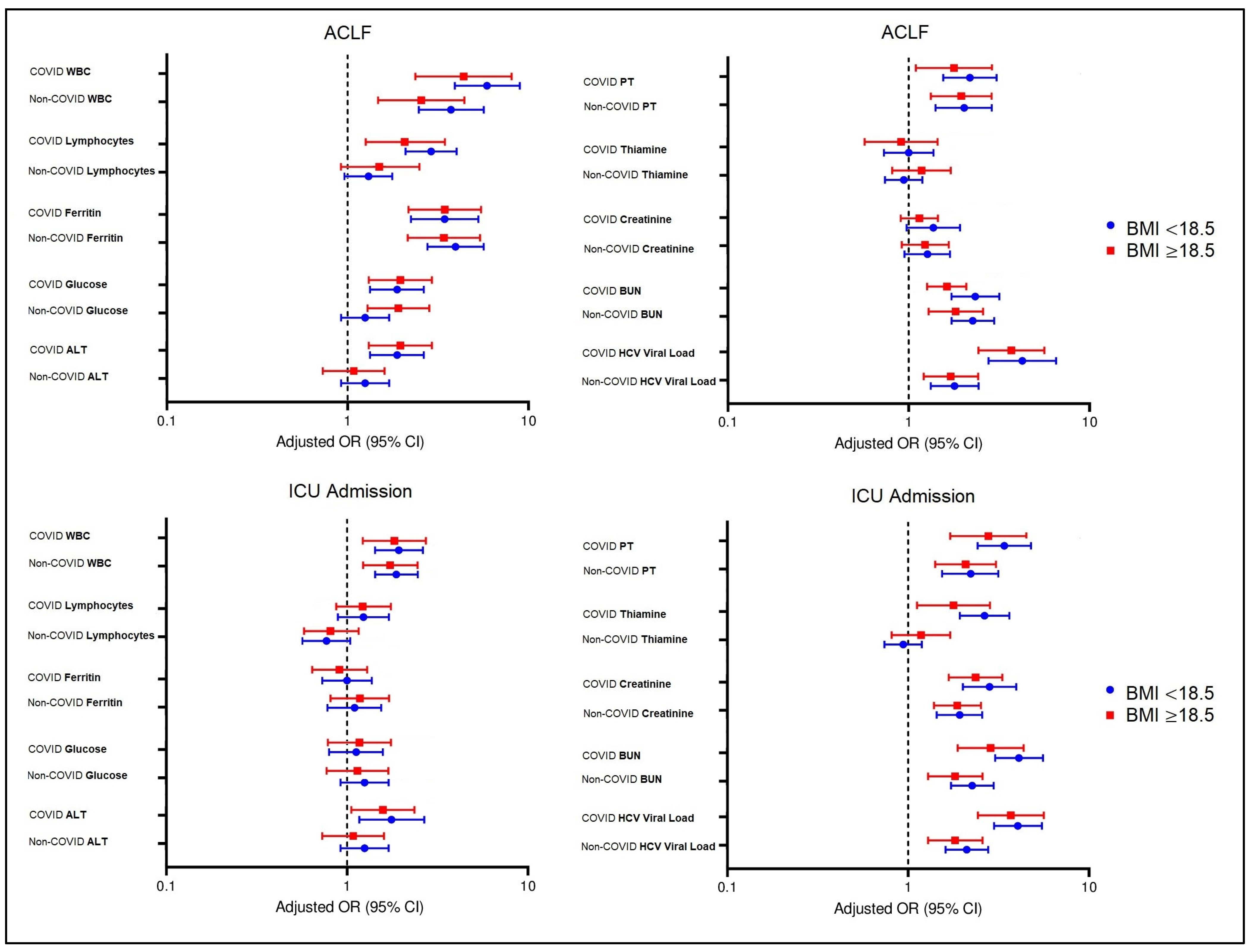
| ACLF | 9 (19.6%) | 10 (5.1%) | <0.001 |
| ICU admission | 12 (26.0%) | 16 (8.2%) | <0.001 |
| Mortality | 7 (15.2%) | 12 (6.1%) | 0.039 |
| Variables * | Normal Range | COVID (n = 46) | % Outside Normality | Non-COVID (n = 196) | % Outside Normality | p-Value ** |
|---|---|---|---|---|---|---|
| Complete blood count | ||||||
| RBC (millions/mm3) | 4.35–5.65 | 3.31 ^ (1.5) | 70.4% | 3.39 ^ (1.3) | 67.2% | 0.301 |
| PLT (thousands/mm3) | 150–450 | 94 ^ (116) | 75.1% | 90 ^ (98) | 71.0% | 0.442 |
| WBC (thousands/mm3) | 4.5–11.0 | 12.2 ^ (7.3) | 48.1% | 4.6 (2.6) | 22.4% | <0.001 |
| Neutrophils (thousands/mm3) | 1.5–8.0 | 5.0 (5.3) | 16.1% | 3.8 (4.0) | 20.7% | 0.056 |
| Monocytes (thousands/mm3) | 0.1–1.0 | 0.4 (0.5) | 7.8% | 0.6 (0.3) | 9.2% | 0.840 |
| Eosinophils (units/mm3) | 30–300 | 142 (96) | 2.2% | 173 (101) | 4.9% | 0.727 |
| Lymphocytes (thousands/mm3) | 1.0–4.8 | 6.9 ^ (6.2) | 63.6% | 2.5 (3.6) | 38.8% | <0.001 |
| Hb (g/dL) | 13.0–17.0 | 11.8 ^ (4.6) | 67.2% | 12.0 ^ (5.2) | 65.6% | 0.882 |
| Hematocrit (%) | 36–48 | 37 (12) | 22.4% | 39 (13) | 20.5% | 0.904 |
| Ferritin (µg/L) | 24–336 | 479 ^ (301) | 88.1% | 355 ^ (205) | 52.2% | <0.001 |
| Haptoglobin (mg/dL) | 41–165 | 72 (52) | 35.3% | 79 (64) | 31.6% | 0.651 |
| Mean corpuscular volume (fL) | 80–96 | 88 (94) | 32.7% | 85 (91) | 34.5% | 0.629 |
| Liver function tests | ||||||
| Fasting glucose (mmol/L) | 60–125 | 146 ^ (84) | 73.5% | 128 ^ (80) | 62.4% | 0.024 |
| ALT (U/L) | 7–35 | 57 ^ (42) | 68.2% | 44 ^ (35) | 54.7% | 0.049 |
| AST (U/L) | 10–40 | 43 ^ (36) | 35.5% | 36 (30) | 28.0% | 0.063 |
| ALP (U/L) | 40–130 | 141 ^ (110) | 53.6% | 138 ^ (106) | 48.4% | 0.474 |
| Serum albumin (g/dL) | 3.4–5.4 | 3.6 (1.2) | 15.3% | 3.8 (1.4) | 12.9% | 0.703 |
| Total proteins (g/dL) | 6.0–8.3 | 6.2 (3.5) | 17.8% | 6.1 (2.3) | 17.1% | 0.936 |
| Total bilirubin (g/dL) | 0.3–1.2 | 1.5 ^ (1.6) | 52.0% | 1.4 ^ (1.2) | 48.3% | 0.522 |
| GGT (U/L) | 0–30 | 48 ^ (34) | 73.1% | 46 ^ (30) | 66.5% | 0.162 |
| LDH (U/L) | 140–280 | 245 (144) | 23.5% | 267 (151) | 26.8% | 0.329 |
| PT (seconds) | 11.0–13.5 | 13.9 ^ (7.5) | 40.3% | 11.2 (4.2) | 24.6% | 0.008 |
| APTT (seconds) | 30–40 | 39 (12) | 23.6% | 36 (8) | 13.0% | 0.101 |
| Nutritional deficiency | ||||||
| Iron (µg/dL) | 60–170 | 64 (32) | 37.4% | 62 (32) | 38.9% | 0.946 |
| Folate (nmol/mL) | 2.7–17.0 | 2.9 (2.0) | 31.0% | 3.0 (2.1) | 32.4% | 0.951 |
| Vitamin B12 (pg/mL) | 160–950 | 167 (237) | 44.6% | 171 (222) | 40.3% | 0.704 |
| Vitamin B6 (µg/L) | 5–50 | 8 (11) | 35.5% | 8 (14) | 36.9% | 0.892 |
| Thiamine (µg/dL) | 2.5–7.5 | 2.4 ^ (3.1) | 59.6% | 2.6 (2.3) | 48.3% | 0.041 |
| Kidney function tests | ||||||
| Creatinine (µmol/L) | 0.74–1.35 | 1.54 ^ (2.62) | 68.7% | 1.31 (1.50) | 50.7% | <0.001 |
| BUN (mmol/L) | 2.1–8.5 | 14 ^ (16) | 75.5% | 11 ^ (11) | 62.2% | 0.002 |
| Urinary albumin (mg/g) | 0–30 | 42 ^ (13) | 62.6% | 40 ^ (10) | 59.3% | 0.776 |
| GFR | >60 | 49 ^ (32) | 73.0% | 56 ^ (26) | 64.9% | 0.055 |
| Lipid profile | ||||||
| Total cholesterol (mg/dL) | 100–200 | 101.5 (60.3) | 52.7% | 112 (54.6) | 48.6% | 0.266 |
| Triglycerides | 50–150 | 66.4 (41.7) | 17.3% | 69.2 (39.4) | 15.1% | 0.826 |
| VLDL-C (mg/dL) | 2–30 | 17.1 (9.5) | 7.2% | 18.2 (9.0) | 7.6% | 0.943 |
| LDL-C (mg/dL) | <100 | 79.2 (36.8) | 11.6% | 76.1 (38.4) | 9.9% | 0.794 |
| HDL-C (mg/dL) | 40–60 | 34.0 ^ (19.3) | 35.4% | 39.5 ^ (21.4) | 27.4% | 0.057 |
| HCV viral load (U/L × 103) | <15 | 38,402 (35,195) | 100% | 29,365 (24,392) | 100% | <0.001 |
| Variables * | Normal Range | During COVID (n = 46) | After COVID (n = 39) | p-Value *** |
|---|---|---|---|---|
| Inflammatory markers | ||||
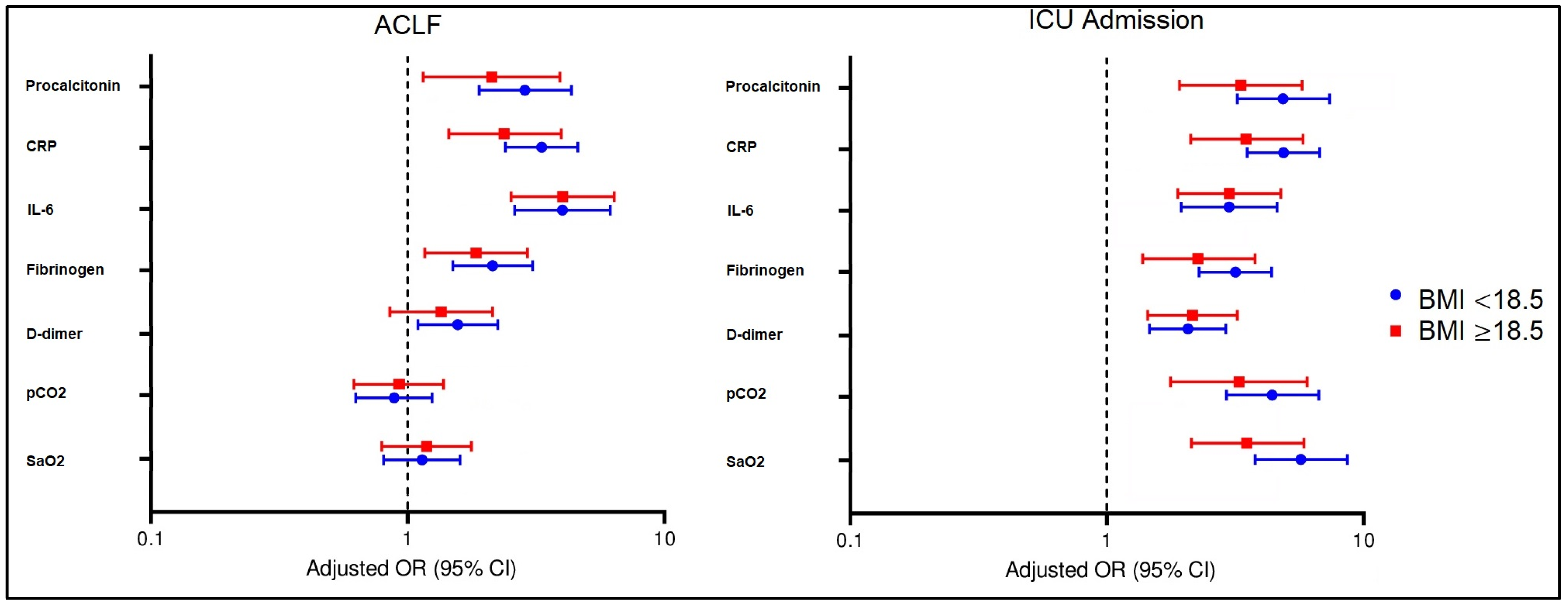
| Procalcitonin (ug/L) ** | 0–0.5 ug/L | 0.5 ± 0.2 | ^ 1.2 ± 1.0 | <0.001 |
| CRP (mg/L) ** | 0–10 mg/L | ^ 56 ± 13 | ^ 12 ± 7 | <0.001 |
| IL-6 (pg/mL) ** | 0–16 pg/mL | ^ 49 ± 17 | ^ 17 ± 10 | <0.001 |
| TNF-α (pg/mL) | 0–29 pg/mL | ^ 42 ± 9 | ^ 39 ± 8 | 0.111 |
| IFN-γ (pg/mL) | 0–3 pg/mL | ^ 3.2 ± 0.5 | 3.0 ± 0.6 | 0.097 |
| ESR (mm/h) | 0–22 mm/hr | ^ 43 ± 8 | ^ 40 ± 8 | 0.088 |
| Fibrinogen (g/L) | 2–4 g/L | ^ 5.1 ± 1.0 | 3.7 ± 1.0 | <0.001 |
| D-dimer (ng/mL) | <250 | ^ 331 ± 53 | ^ 262 ± 31 | <0.001 |
| Arterial blood gas | ||||
| Arterial pH | 7.35–7.45 | ^ 7.46 ± 0.6 | 7.37 ± 0.9 | 0.584 |
| pO2 (mmHg) | 80–100 mmHg | ^ 77 ± 12 | 80 ± 9 | 0.202 |
| pCO2 (mmHg) | 35–45 mmHg | ^ 49 ± 5 | 43 ± 7 | <0.001 |
| HCO3 (mEq/L) | 22–28 mEq/L | 23 ± 6 | 24 ± 4 | 0.377 |
| SaO2 (%) | 94–100% | ^ 89 ± 7 | ^ 92 ± 5 | 0.028 |
| Clinical Outcomes * | Acute COVID (n = 46) | After COVID (n = 39) | p-Value ** |
|---|---|---|---|
| Jaundice | 13 (28.3%) | 16 (41.0%) | 0.216 |
| Portal hypertension | 28 (60.9%) | 28 (71.8%) | 0.289 |
| Upper gastrointestinal bleeding | 6 (13.0%) | 2 (5.1%) | 0.497 |
| Encephalopathy | 25 (54.3%) | 24 (61.5%) | 0.503 |
| Gastritis | 27 (58.7%) | 24 (61.5%) | 0.789 |
| Pleural effusion | 7 (15.2%) | 13 (33.3%) | 0.049 |
| Ascites | 19 (41.3%) | 21 (53.9%) | 0.248 |
| Spontaneous bacterial peritonitis | 4 (8.7%) | 7 (17.9%) | 0.205 |
| Hepatorenal syndrome | 4 (8.7%) | 3 (7.7%) | 0.866 |
| Child–Pugh Score | 0.543 | ||
| Child–Pugh A | 26 (56.5%) | 25 (64.1%) | |
| Child–Pugh B | 13 (28.3%) | 11 (28.2%) | |
| Child–Pugh C | 7 (15.2%) | 3 (7.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerbu, B.; Grigoras, M.L.; Bratosin, F.; Bogdan, I.; Citu, C.; Bota, A.V.; Timircan, M.; Bratu, M.L.; Levai, M.C.; Marincu, I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. J. Clin. Med. 2022, 11, 652. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030652
Cerbu B, Grigoras ML, Bratosin F, Bogdan I, Citu C, Bota AV, Timircan M, Bratu ML, Levai MC, Marincu I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. Journal of Clinical Medicine. 2022; 11(3):652. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030652
Chicago/Turabian StyleCerbu, Bianca, Mirela Loredana Grigoras, Felix Bratosin, Iulia Bogdan, Cosmin Citu, Adrian Vasile Bota, Madalina Timircan, Melania Lavinia Bratu, Mihaela Codrina Levai, and Iosif Marincu. 2022. "Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis" Journal of Clinical Medicine 11, no. 3: 652. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11030652