Enhanced Salivary and General Oxidative Stress in Hashimoto’s Thyroiditis Women in Euthyreosis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Collection
2.3. Saliva Collection
2.4. Dental and Periodontal Examination
2.5. Xerostomy Assessment and Schirmer Test
2.6. Selection of Patients and the Control Group Participants
2.7. Biochemical Determinations: Salivary Amylase Activity and IL-1β Concentration
2.8. Biochemical Determinations: Redox Assay
2.8.1. Enzymatic Antioxidants
2.8.2. Non-Enzymatic Antioxidants
2.8.3. Total Oxidant Status (TOS) and Oxidative Stress Index (OSI)
2.8.4. Oxidative Damage to Proteins and Lipids
2.9. Statistical Analysis
3. Results
3.1. Clinical Data
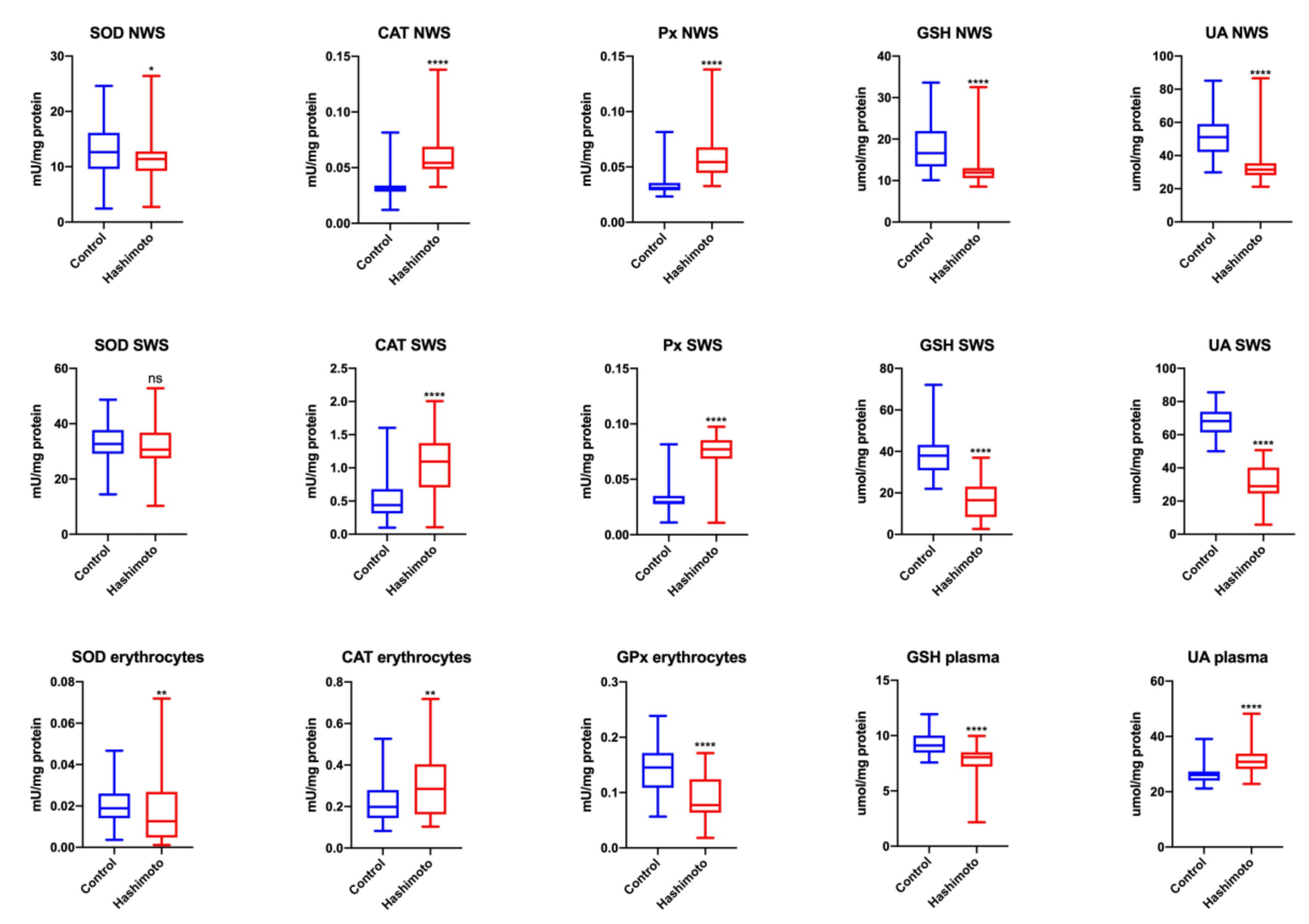
3.2. Antioxidant Defense Parameters
3.2.1. NWS
3.2.2. SWS
3.2.3. Erythrocytes, Plasma
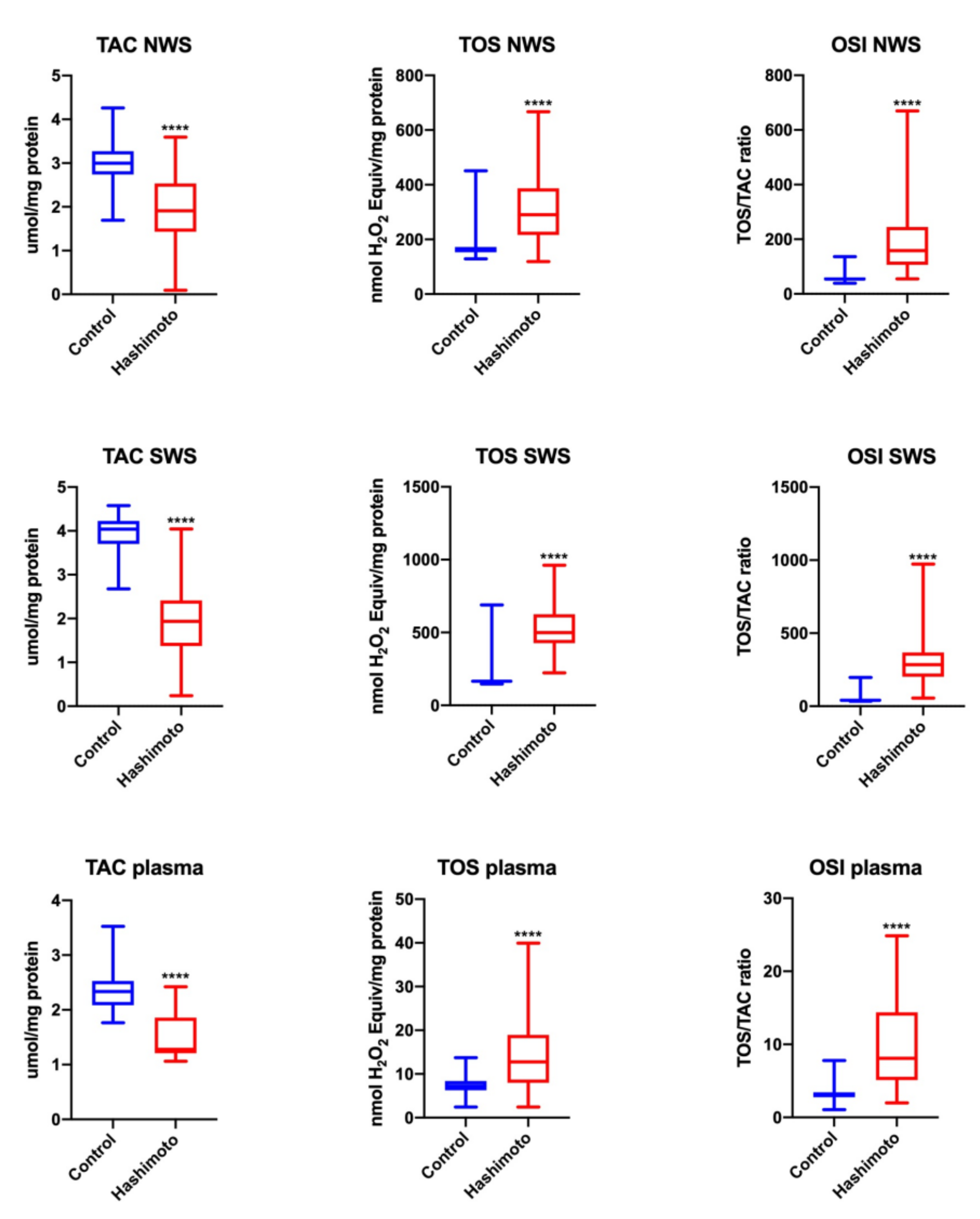
3.2.4. TOS and OSI
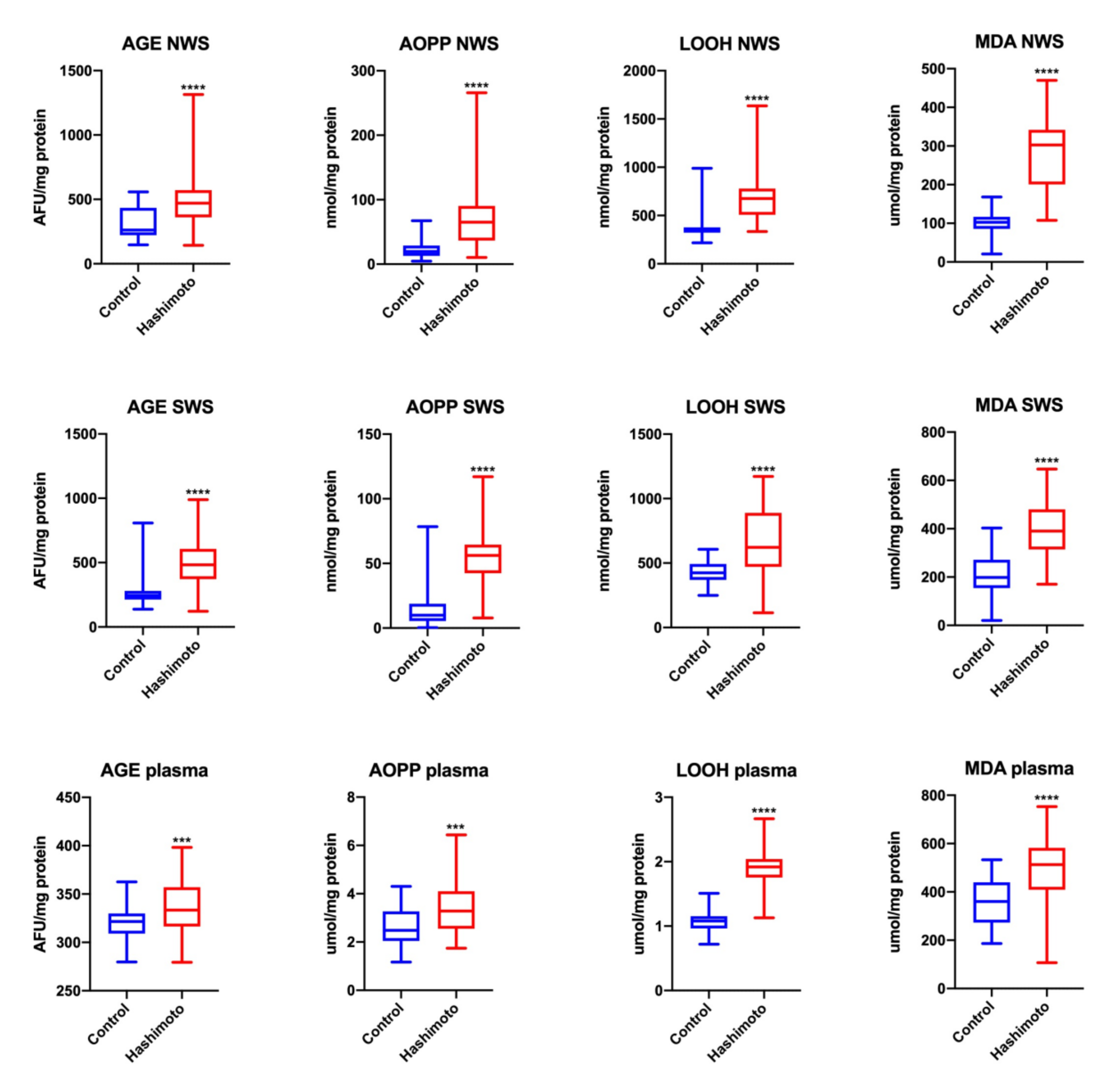
3.2.5. Products of Oxidative Modifications
3.2.6. Comparison of Antioxidants and Redox Balance Markers between NWS and SWS
Control
HT Women
3.2.7. Saliva–Blood Ratio
NWS
SWS
3.2.8. Correlations
4. Discussion
5. Conclusions
- (1)
- Parotid as well as submandibular salivary glands of HT female patients in euthyreosis had an impaired ability to maintain the redox status at the level observed in the salivary glands of the control women.
- (2)
- The saliva of patients with HT in euthyreosis demonstrated a reduced antioxidant potential. Moreover, a significant increase in oxidatively modified molecules in NWS and SWS suggests the failure of the salivary gland antioxidant barrier to combat excess ROS production.
- (3)
- OS in NWS and SWS of HT women appears to be closely connected with autoimmunity-related inflammation, and not with the level of thyroid hormones or TSH.
- (4)
- The secretory function of the submandibular glands of HT female patients in euthyreosis is decreased, which is manifested as a significant reduction of unstimulated saliva secretion.
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rose, N.R.; Bonita, R.; Burek, C.L. Iodine: An environmental trigger of thyroiditis. Autoimmun Rev. 2002, 1, 97–103. [Google Scholar] [CrossRef]
- Rostami, R.; Aghasi, M.R.; Mohammadi, A.; Nourooz-Zadeh, J. Enhanced oxidative stress in Hashimoto’s thyroiditis: Inter-relationships to biomarkers of thyroid function. Clin. Biochem. 2013, 46, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Ates, I.; Yilmaz, F.M.; Altay, M.; Yilmaz, N.; Berker, D.; Guler, S. The relationship between oxidative stress and autoimmunity in Hashimoto’s thyroiditis. Eur. J. Endocrinol 2015, 173, 791–799. [Google Scholar] [CrossRef]
- Ates, I.; Arikan, M.F.; Altay, M.; Yilmaz, F.M.; Yilmaz, N.; Berker, D.; Guler, S. The effect of oxidative stress on the progression of Hashimoto’s thyroiditis. Arch. Physiol. Biochem. 2018, 124, 351–356. [Google Scholar] [CrossRef]
- Knaś, M.; Maciejczyk, M.; Waszkiel, D.; Zalewska, A. Oxidative stress and salivary antioxidants. Dent. Med. Probl. 2013, 50, 461–466. [Google Scholar]
- Lassoued, S.; Mseddi, M.; Mnif, F.; Abid, M.; Guermazi, F.; Masmoudi, H.; El Feki, A.; Attia, H. A comparative study of the oxidative profile in Graves’ disease, Hashimoto’s thyroiditis, and papillary thyroid cancer. Biol. Trace Elem. Res. 2010, 138, 107–115. [Google Scholar] [CrossRef]
- Nanda, N.; Bobby, Z.; Hamide, A. Oxidative stress in anti thyroperoxidase antibody positive hypothyroid patients. Asian J. Biochem. 2012, 7, 54–58. [Google Scholar]
- Agha-Hosseini, F.; Shirzad, N.; Moosavi, M.S. Evaluation of Xerostomia and salivary flow rate in Hashimoto’s Thyroiditis. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Toczewska, J.; Konopka, T.; Zalewska, A.; Maciejczyk, M. Nitrosative stress biomarkers in the non-stimulated and stimulated saliva, as well as gingival crevicular fluid of patients with periodontitis: Review and clinical study. Antioxidants 2020, 9, 259. [Google Scholar] [CrossRef] [Green Version]
- Toczewska, J.; Konopka, T. Activity of enzymatic antioxidants in periodontitis: A systematic overview of the literature. Dent. Med. Probl. 2019, 56, 419–426. [Google Scholar] [CrossRef] [Green Version]
- Darczuk, D.; Krzyściak, W.; Bystrowska, B.; Kęsek, B.; Kościelniak, D.; Chomyszyn-Gajewska, M.; Kaczmarzyk, T. The relationship between the concentration of salivary tyrosine and antioxidants in patients with oral lichen planus. Oxid. Med. Cell Longev. 2019, 2019, 5801570. [Google Scholar] [CrossRef] [PubMed]
- Babiuch, K.; Bednarczyk, A.; Gawlik, K.; Pawlica-Gosiewska, D.; Kęsek, B.; Darczuk, D.; Stępień, P.; Chomyszyn-Gajewska, M.; Kaczmarzyk, T. Evaluation of enzymatic and non-enzymatic antioxidant status and biomarkers of oxidative stress in saliva of patients with oral squamous cell carcinoma and oral leukoplakia: A pilot study. Acta Odont. Scand. 2019, 77, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Flisiak, I.; Kolodziej, J.K.U.; Kotowska-Rodziewicz, A.; Klimiuk, A.; Zalewska, A. Enhanced inflammation and nitrosative stress in the saliva and plasma of patients with plaque psoriasis. J. Clin. Med. 2020, 9, 745. [Google Scholar] [CrossRef] [Green Version]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Fejfer, K.; Krahel, J.; Flisiak, I.; Kołodziej, U.; Zalewska, A. Salivary antioxidants and oxidative stress in psoriatic patients: Can salivary total oxidant status and oxidative stress index be a plaque psoriasis biomarker? Oxid. Med. Cell Longev. 2020, 2020, 9086024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zalewska, A.; Knaś, M.; Waszkiewicz, N.; Waszkiel, D.; Sierakowski, S.; Zwierz, K. Rheumatoid arthritis patients with xerostomia have reduced production of key salivary constituents. Oral Surg. Oral Med. Oral Pathol. 2013, 115, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Zalewska, A.; Knaś, M.; Waszkiewicz, N.; Klimiuk, A.; Litwin, K.; Sierakowski, S.; Waszkiel, D. Salivary antioxidants in patients with systemic sclerosis. J. Oral Pathol. Med. 2014, 43, 61–68. [Google Scholar] [CrossRef]
- Zalewska, A.; Knaś, M.; Kuźmiuk, A.; Waszkiewicz, N.; Niczyporuk, M.; Waszkiel, D.; Zwierz, K. Salivary innate defense system in type 1 diabetes mellitus in children with mixed and permanent dentition. Acta Odont. Scand. 2013, 71, 1493–1500. [Google Scholar] [CrossRef]
- Norheim, K.B.; Jonsson, G.; Harboe, E.; Hanasand, M.; Gøransson, L.; Omdal, R. Oxidative stress, as measured by protein oxidation, is increased in primary Sjøgren’s syndrome. Free Radic. Res. 2012, 46, 141–146. [Google Scholar] [CrossRef]
- Karlík, M.; Valkovič, P.; Hančinová, V.; Krížová, L.; Tóthová, Ľ.; Celec, P. Markers of oxidative stress in plasma and saliva in patients with multiple sclerosis. Clin. Biochem. 2015, 48, 24–28. [Google Scholar] [CrossRef]
- Su, H.; Baron, M.; Benarroch, M.; Velly, A.M.; Gravel, S.; Schipper, H.M.; Gornitsky, M. Altered salivary redox homeostasis in patients with systemic sclerosis. J. Rheumatol. 2010, 37, 1858–1863. [Google Scholar] [CrossRef]
- Zaieni, S.H.; Derakhshan, Z.; Sariri, R. Alternations of salivary antioxidant enzymes in systemic lupus erythematosus. Lupus 2015, 24, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Nagler, R.M.; Klein, I.; Zarzhevsky, N.; Drigues, N.; Reznick, A.Z. Characterization of the differentiated antioxidant profile of human saliva. Free Radic. Biol. Med. 2002, 32, 268–277. [Google Scholar] [CrossRef]
- Klimiuk, A.; Zalewska, A.; Sawicki, R.; Knapp, M.; Maciejczyk, M. Salivary oxidative stress increases with the progression of chronic heart failure. J. Clin. Med. 2020, 9, 769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buege, J.A.; Aust, S.D. Microsomal lipid peroxidation. Methods Enzymol. 1978, 52, 302–310. [Google Scholar]
- Vitali, C.; Bombardieri, S.; Jonsson, R.; Moutsopoulos, H.M.; Alexander, E.L.; Carsons, S.E.; Daniels, T.E.; Fox, R.I.; Kasson, S.S.; Pillemer, S.R.; et al. Classification criteria for Sjogren’s syndrome: A revised version of the European criteria proposed by American-European Consensus Group. Ann. Rheum. Dis. 2002, 61, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Schirmer, O. Studien zur physiologie der tranenabsonderung und tranenabfuhr. Arch. Opthalmol. 1903, 56, 197–221. [Google Scholar] [CrossRef]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar] [PubMed]
- Aebi, H. Catalase in vitro. Methods Enzymol. 1984, 105, 121–126. [Google Scholar] [PubMed]
- Mansson-Rahemtulla, B.; Baldone, D.C.; Pruitt, K.M.; Rahemtulla, F. Specific assays for peroxidases in human saliva. Arch. Oral Biol. 1986, 31, 661–668. [Google Scholar] [CrossRef]
- Paglia, D.E.; Valentine, W.N. Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J. Lab. Clin. Med. 1967, 70, 158–169. [Google Scholar]
- Griffith, O.W. Determination of glutathione and glutathione disulfide using glutathione reductase and 2-vinylpyridine. Anal. Biochem. 1980, 106, 207–212. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 227–285. [Google Scholar] [CrossRef] [PubMed]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef]
- Kołodziej, U.; Maciejczyk, M.; Niklińska, W.; Waszkiel, D.; Żendzian-Piotrowska, M.; Żukowski, P.; Zalewska, A. Chronic high-protein diet induces oxidative stress and alters the salivary gland function in rats. Arch. Oral Biol. 2017, 84, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Kalousová, M.; Skrha, J.; Zima, T. Advanced glycation end-products and advanced oxidation protein products in patients with diabetes mellitus. Physiol. Res. 2002, 51, 597–604. [Google Scholar] [PubMed]
- Grintzalis, K.; Zisimopoulos, D.; Grune, T.; Weber, D.; Georgiou, C.D. Method for the simultaneous determination of free/protein malondialdehyde and lipid/protein hydroperoxides. Free Radic. Biol. Med. 2013, 59, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Duthoit, C.; Estienne, V.; Giraud, A.; Durand-Gorde, J.M.; Rasmussen, A.K.; Feldt-Rasmussen, U.; Carayon, P.; Ruf, J. Hydrogen peroxide-induced production of a 40 kDa immunoreactive thyroglobulin fragment in human thyroid cells: The onset of thyroid autoimmunity? Biochem. J. 2001, 360, 557–562. [Google Scholar] [CrossRef]
- Burek, C.L.; Rose, N.R. Autoimmune thyroiditis and ROS. Autoimmun. Rev. 2008, 7, 530–537. [Google Scholar] [CrossRef]
- Lushchak, V.L. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Biol. Interact. 2014, 224, 164–175. [Google Scholar] [CrossRef]
- Lushchak, V.L. Classification of oxidative stress based on its intensity. Exp. Clin. Sci. 2014, 13, 922–937. [Google Scholar]
- Knaś, M.; Maciejczyk, M.; Sawicka, K.; Hady Razak, H.; Niczyporuk, M.; Ładny, J.R.; Matczuk, J.; Waszkiel, D.; Żendzian-Piotrowska, M.; Zalewska, A. Impact of morbid obesity and bariatric surgery on antioxidant/oxidant balance of the unstimulated and stimulated saliva. J. Oral Pathol. Med. 2016, 45, 455–464. [Google Scholar] [CrossRef]
- Knaś, M.; Maciejczyk, M.; Daniszewska, I.; Klimiuk, A.; Matczuk, J.; Kołodziej, U.; Waszkiel, D.; Ładny, J.R.; Żendzian-Piotrowska, M.; Zalewska, A. Oxidative damage to the salivary glands of rats with streptozotocin-induced diabetes-temporal study: Oxidative stress and diabetic salivary glands. J. Diabetes Res. 2016, 2016, 4583742. [Google Scholar] [CrossRef] [Green Version]
- Viazzi, F.; Garneri, D.; Leoncini, G.; Gonnella, A.; Muiesan, M.L.; Ambrosioni, E.; Costa, F.V.; Leonetti, G.; Pessina, A.C.; Trimarco, B.; et al. Serum uric acid and its relationship with metabolic syndrome and cardiovascular risk profile in patients with hypertension: Insights from the I-DEMAND study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Matczuk, J.; Zendzian-Piotrowska, M.; Maciejczyk, M.; Kurek, K. Salivary lipids: A review. Adv. Clin. Exp. Med. 2017, 26, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Zalewska, A.; Waszkiel, D.; Łuczaj-Cepowicz, D.; Szajda, S.D.; Waszkiewicz, N. Salivary gland involvement in rheumatoid arthritis: Salivary peroxidase and the flow rate. Pol. J. Environ. Stud. 2010, 19, 321–325. [Google Scholar]
- Pruitt, K.M.; Tenovuo, J.; Mansson-Rahemtulla, B.; Harrington, P.; Baldone, D.C. Is thiocyanate peroxidation at equilibrium in vivo? Biochim. Biophys. Acta 1986, 870, 385–391. [Google Scholar] [CrossRef]
- Tenovuo, J.; Larjava, H. The protective effect of peroxidase and thiocyanate against hydrogen peroxide toxicity assessed by the uptake of [3H]-thymidine by human gingival fibroblasts cultured in vitro. Arch. Oral Biol. 1984, 29, 445–451. [Google Scholar] [CrossRef]
- Hanstrom, L.; Johansson, A.; Carlsson, J. Lactoperoxidase and thiocyanate protect cultured mammalian cells against hydrogen peroxide toxicity. Med. Biol. 1983, 61, 268–274. [Google Scholar]
- Erejuwa, O.O.; Gurtu, S.; Sulaiman, S.A.; Wahab, M.S.A.; Sirajudeen, K.N.; Salleh, M.S. Hypoglycemic and antioxidant effects of honey supplementation in streptozotocin-induced diabetic rats. Int. J. Vitam. Nutr. Res. 2010, 80, 74–82. [Google Scholar]
- Cooper, A.J.; Pinto, J.T.; Callery, P.S. Reversible and irreversible protein glutathionylation: Biological and clinical aspects. Expert Opin. Drug Metab. Toxicol. 2011, 7, 891–910. [Google Scholar] [CrossRef] [Green Version]
- Lushchak, V.I. Glutathione homeostasis and functions: Potential targets for medical interventions. J. Amino Acids 2012, 2012, 736837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azuma, M.; Aota, K.; Tamatani, T.; Motegi, K.; Yamashita, T.; Ashida, Y.; Hayashi, Y.; Sato, M. Suppression of tumor necrosis factor alpha-induced matrix metalloproteinase 9 production in human salivary gland acinar cells by cepharanthine occurs via down-regulation of nuclear factor kappaB: A possible therapeutic agent for preventing the destruction of the acinar structure in the salivary glands of Sjogren’s syndrome patients. Arthr. Rheum. 2002, 46, 1585–1594. [Google Scholar] [CrossRef]
- Bozzato, A.; Burger, P.; Zenk, J.; Ulter, W.; Iro, H. Salivary gland biometry in female patients with eating disorders. Eur. Arch. Otorhinolaryngol. 2008, 265, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Heo, M.S.; Lee, S.C.; Lee, S.S.; Choi, H.M.; Choi, S.C.; Park, T.W. Quantitative analysis of normal major salivary glands using computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 240–244. [Google Scholar] [CrossRef]
- Watanabe, M.; Yamagishi-Wang, H.; Kawaguchi, M. Lowered susceptibility of muscarinic receptor involved in salivary secretion of streptozotocin-induced diabetic rats. Jpn. J. Pharmacol. 2001, 87, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanemaaijer, R.; Visser, H.; Konttinen, Y.T.; Koolwijk, P.; Verheijen, J.H. A novel and simple immunocapture assay for determination of gelatinase-B (MMP-9) activities in biological fluids: Saliva from patients with Sjogren’s syndrome contain increased latent and active gelatinase-B levels. Matrix Biol. 1998, 17, 657–665. [Google Scholar] [CrossRef]
- Skov Olsen, P.; Kirkegaard, P.; Rasmussen, T.; Magid, E.; Poulsen, S.S.; Nexø, E. Adrenergic effects on secretion of amylase from the rat salivary glands. Digestion 1988, 41, 34–38. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients Variables | Control, n = 45 M (Min–Max) | HT, n = 45 M (Min–Max) | p |
|---|---|---|---|
| Age (years) | 35 (29–43) | 35 (29–43) | NS |
| BMI (kg/m2) | 19.25 (18.3–24.52) | 23.15 (18.19–25.89) | NS |
| TSH (µU/mL) | 1,99 (0.35–2.85) | 2.85 (0.35–4.94) | NS |
| Free T4 (ng/mL) | 1.2 (0.91–1.4) | 1.1 (0.7–1.42) | NS |
| Free T3 (pg/mL) | 2.56 (1.9–3.45) | 2.4 (1.7–3.65) | NS |
| Anty TPO (IU/mL) | 0.35 (0–2.1) | 321.2 (108.25–652.1) | <0.0001 |
| Anty TG (IU/mL) | 0.32 (0–2.1) | 153.8 (99.9–333.1) | <0.0001 |
| PTH (pg/mL) | 39.45 (10–62.2) | 35.02 (15.51–63.56) | NS |
| Glucose (mg/dL) | 86.37 (76.96–95.49) | 84.11 (73.90–98.65) | NS |
| Euthyrox, n(%) | 0 | 24 (53.3%) |
| Clinical Parameters | Control | HT | p | ||||
|---|---|---|---|---|---|---|---|
| Median | Minimum | Maximum | Median | Minimum | Maximum | ||
| NWS mL/min | 0.51 | 0.27 | 0.96 | 0.32 | 0.07 | 0.77 | 0.02 |
| SWS mL/min | 1.01 | 0.9 | 2 | 0.9 | 0.2 | 2 | ns |
| TP NWS (mg/mL) | 704.2 | 556.5 | 924.5 | 1293 | 979.4 | 1707 | <0.0001 |
| TP SWS (mg/mL) | 1545 | 371.3 | 1672 | 1834 | 266.6 | 3861 | <0.0001 |
| Salivary amylase NWS (μmol/mg protein) | 0.22 | 0.18 | 0.28 | 0.11 | 0.09 | 0.15 | <0.0001 |
| Salivary amylase SWS (μmol/mg protein) | 0.3 | 0.19 | 0.38 | 0.14 | 0.1 | 0.16 | <0.0001 |
| Salivary IL-1β NWS (pg/mg protein) | 0.91 | 0.27 | 2 | 2 | 0.4 | 3 | <0.0001 |
| Salivary IL-1β SWS (pg/mg) | 5.1 | 2.7 | 6.8 | 7.8 | 4 | 12 | <0.0001 |
| Schirmer- I test (mm/5 min) Left eye Right eye | 21 25 | 10 11 | 28 30 | 19 20 | 12 9 | 23 30 | ns |
| Subjective dryness n (%) Xerostomiaxerophtalmia | 1(2.22) 3(6.67) | 26(57.7) 3(6.67) | 0.003 ns | ||||
| DMFT | 15 | 0 | 25 | 16 | 3 | 28 | ns |
| API | 41.85 | 0 | 100 | 54.5 | 8.3 | 100 | ns |
| GI | 1 | 0 | 2 | 1 | 0 | 2 | ns |
| PPD (mm) | 1.898 | 1.14 | 2.55 | 1.99 | 1.33 | 3.64 | ns |
| Redox Parameters | Control | HT | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NWS | SWS | p | NWS | SWS | p | |||||||||
| Median | Minimum | Maximum | Median | Minimum | Maximum | Median | Minimum | Maximum | Median | Minimum | Maximum | |||
| SOD | 12.63 | 2.439 | 24.6 | 32.67 | 14.42 | 48.69 | <0.0001 | 11.38 | 2.746 | 26.41 | 30.61 | 10.28 | 52.8 | <0.0001 |
| CAT | 0.0306 | 0.0121 | 0.0815 | 0.4379 | 0.1 | 1.603 | <0.0001 | 0.0544 | 0.0326 | 0.1381 | 1.094 | 0.1058 | 2.006 | <0.0001 |
| Px | 0.031 | 0.0234 | 0.0815 | 0.4379 | 0.1 | 1.603 | <0.0001 | 0.0545 | 0.0326 | 0.1381 | 1.094 | 0.1058 | 2.006 | <0.0001 |
| GSH | 16.61 | 10.09 | 33.62 | 37.94 | 21.98 | 72.11 | <0.0001 | 11.94 | 8.543 | 32.52 | 16.52 | 2.634 | 36.96 | 0.0258 |
| UA | 51.12 | 29.86 | 85.09 | 68.21 | 50.05 | 85.52 | <0.0001 | 31.53 | 21.19 | 86.65 | 28.98 | 5.787 | 50.67 | ns |
| TAC | 2.997 | 1.695 | 4.258 | 4.038 | 2.677 | 4.578 | <0.0001 | 1.909 | 0.0935 | 3.594 | 1.934 | 0.2413 | 4.044 | ns |
| TOS | 160.3 | 129.1 | 451.2 | 165.4 | 147.2 | 689.9 | ns | 290.1 | 118.7 | 666.8 | 499.2 | 223.6 | 961.4 | <0.0001 |
| OSI | 54.48 | 39.2 | 136.5 | 41.24 | 34.02 | 196.7 | <0.0001 | 158.5 | 54.79 | 669.8 | 284 | 55.28 | 973.4 | <0.0001 |
| AGE | 261.6 | 146.4 | 558.1 | 244.5 | 138.5 | 807.9 | ns | 471 | 143.2 | 1314 | 482.9 | 122 | 989.2 | ns |
| AOPP | 19.55 | 4.569 | 67.25 | 9.754 | 0.1632 | 78.37 | <0.0001 | 65.01 | 10.37 | 265.8 | 56.21 | 7.779 | 117 | ns |
| LOOH | 352 | 218.1 | 989.5 | 424.5 | 249.6 | 607.5 | <0.0001 | 675.2 | 334.4 | 1635 | 622.2 | 114.3 | 1172 | ns |
| MDA | 102.6 | 20.49 | 168.2 | 198.4 | 20.46 | 402.8 | <0.0001 | 302.6 | 107.6 | 469.9 | 390.1 | 170.2 | 647.3 | <0.0001 |
| Salivary/Blood Ratio | Control | HT | p | ||||
|---|---|---|---|---|---|---|---|
| Median | Minimum | Maximum | Median | Minimum | Maximum | ||
| SOD NWS | 655.6 | 145.7 | 3580 | 816.4 | 113.1 | 10,113 | ns |
| SOD SWS | 1625 | 396.1 | 10,721 | 2312 | 414.4 | 29,459 | ns |
| CAT NWS | 0.1582 | 0.0411 | 0.8706 | 0.2144 | 0.0501 | 0.8531 | 0.0115 |
| CAT SWS | 1.988 | 0.3915 | 10.61 | 3.337 | 0.3794 | 14.38 | 0.0053 |
| Px NWS | 0.2378 | 0.1272 | 0.9917 | 0.6863 | 0.2076 | 4.777 | <0.0001 |
| Px SWS | 3.186 | 0.6492 | 18.57 | 11.55 | 1.403 | 71.15 | <0.0001 |
| GSH NWS | 1.819 | 0.9336 | 3.613 | 1.464 | 0.9591 | 8.705 | 0.0009 |
| GSH SWS | 4.051 | 2.369 | 9.534 | 2.216 | 0.5282 | 3.961 | <0.0001 |
| UA NWS | 1.973 | 1.002 | 2.763 | 1.034 | 0.6256 | 2.508 | <0.0001 |
| UA SWS | 2.525 | 1.851 | 3.556 | 0.9855 | 0.2191 | 1.775 | <0.0001 |
| TAC NWS | 1.246 | 0.8213 | 2.401 | 1.356 | 0.0647 | 2.665 | ns |
| TAC SWS | 1.728 | 0.9485 | 2.466 | 1.268 | 0.1385 | 2.794 | <0.0001 |
| TOS NWS | 22.5 | 11.08 | 54.29 | 23.78 | 6.919 | 161.5 | ns |
| TOS SWS | 23.61 | 11.63 | 100.9 | 38.81 | 9.852 | 155.5 | <0.0001 |
| OSI NWS | 18.33 | 7.485 | 43.07 | 15.68 | 3.368 | 184 | ns |
| OSI SWS | 13.77 | 7.244 | 54 | 30.15 | 6.401 | 429.8 | <0.0001 |
| AGE NWS | 0.8406 | 0.4666 | 1.786 | 1.366 | 0.4045 | 4.279 | <0.0001 |
| AGE SWS | 0.761 | 0.4457 | 2.84 | 1.434 | 0.3307 | 3.133 | <0.0001 |
| AOPP NWS | 7.951 | 1.338 | 31 | 18.88 | 2.203 | 69.16 | <0.0001 |
| AOPP SWS | 3.725 | 0.0983 | 29.82 | 16.57 | 1.595 | 36.84 | <0.0001 |
| LOOH NWS | 327.5 | 214.4 | 1255 | 334.5 | 177.6 | 805.8 | ns |
| LOOH SWS | 419.4 | 249.7 | 677 | 341.4 | 65.17 | 637 | 0.0135 |
| MDA NWS | 0.2532 | 0.0631 | 0.6355 | 0.5392 | 0.2124 | 3.402 | <0.0001 |
| MDA SWS | 0.5698 | 0.0548 | 1.38 | 0.8321 | 0.2707 | 3.756 | 0.0024 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morawska, K.; Maciejczyk, M.; Popławski, Ł.; Popławska-Kita, A.; Krętowski, A.; Zalewska, A. Enhanced Salivary and General Oxidative Stress in Hashimoto’s Thyroiditis Women in Euthyreosis. J. Clin. Med. 2020, 9, 2102. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072102
Morawska K, Maciejczyk M, Popławski Ł, Popławska-Kita A, Krętowski A, Zalewska A. Enhanced Salivary and General Oxidative Stress in Hashimoto’s Thyroiditis Women in Euthyreosis. Journal of Clinical Medicine. 2020; 9(7):2102. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072102
Chicago/Turabian StyleMorawska, Katarzyna, Mateusz Maciejczyk, Łukasz Popławski, Anna Popławska-Kita, Adam Krętowski, and Anna Zalewska. 2020. "Enhanced Salivary and General Oxidative Stress in Hashimoto’s Thyroiditis Women in Euthyreosis" Journal of Clinical Medicine 9, no. 7: 2102. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072102