Absence of BCL-2 Expression Identifies a Subgroup of AML with Distinct Phenotypic, Molecular, and Clinical Characteristics

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Routine Laboratory Tests
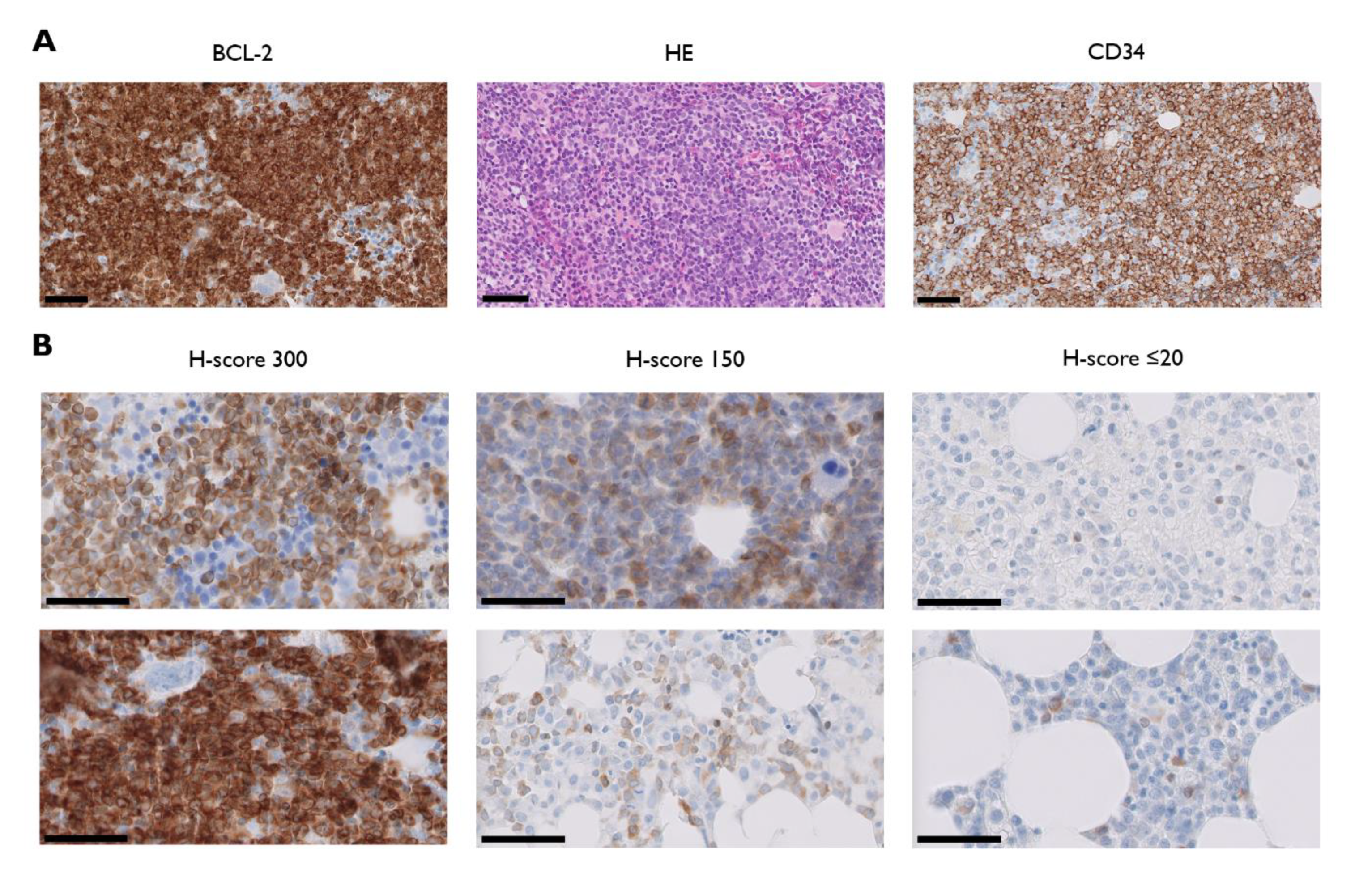
2.3. BCL-2 Immunohistochemistry
2.4. NGS
2.5. Clinical Outcome Evaluation
2.6. Statistical Analyses
3. Results
3.1. BCL-2 Is Heterogeneously Expressed in AML
3.2. BCL-2− and BCL-2+ AML Subgroups Show Similar Proliferative Activity but Different Bone Marrow Blast Percentages
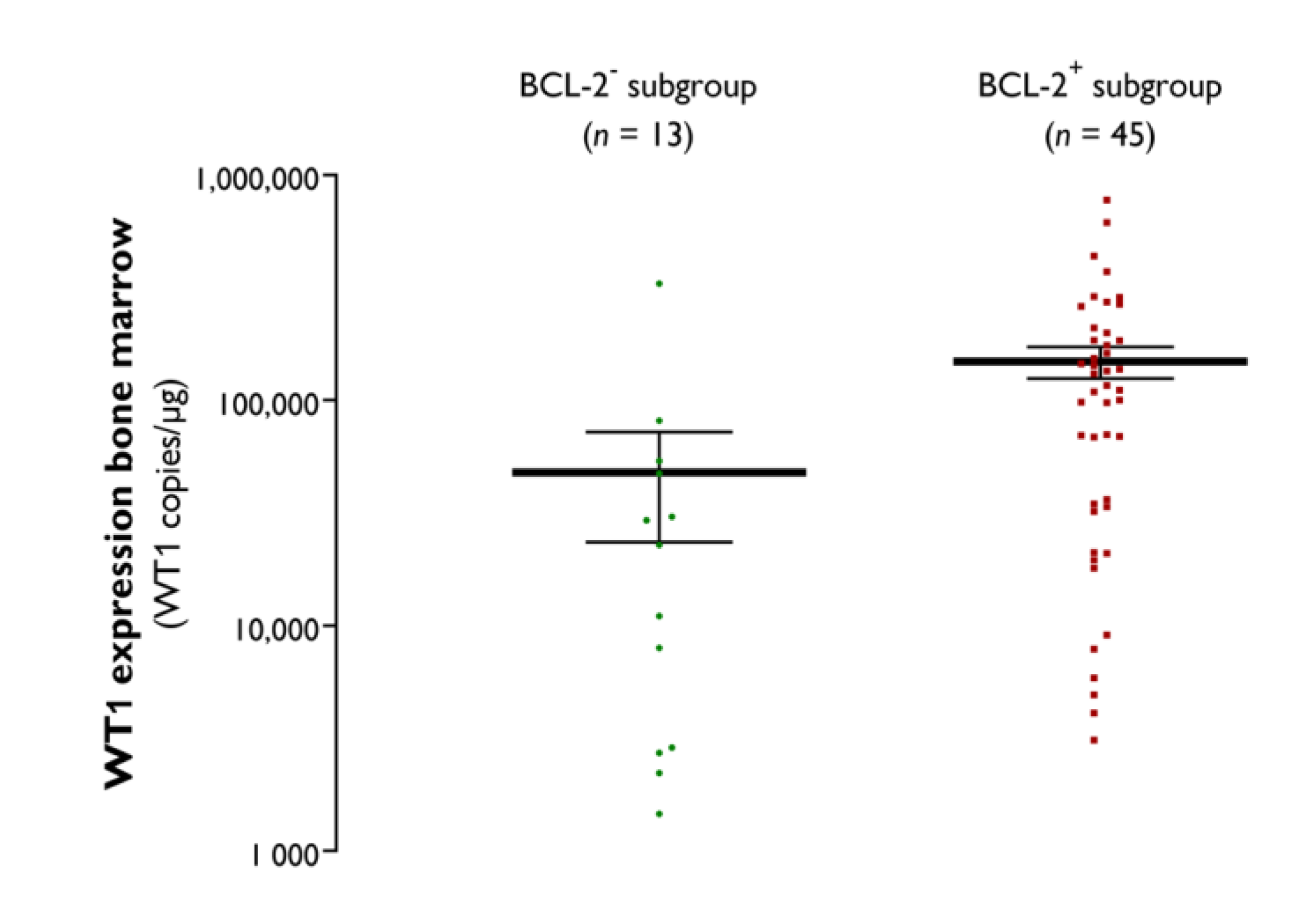
3.3. BCL-2− AML Subgroup Is Characterized by a Distinct Molecular Signature
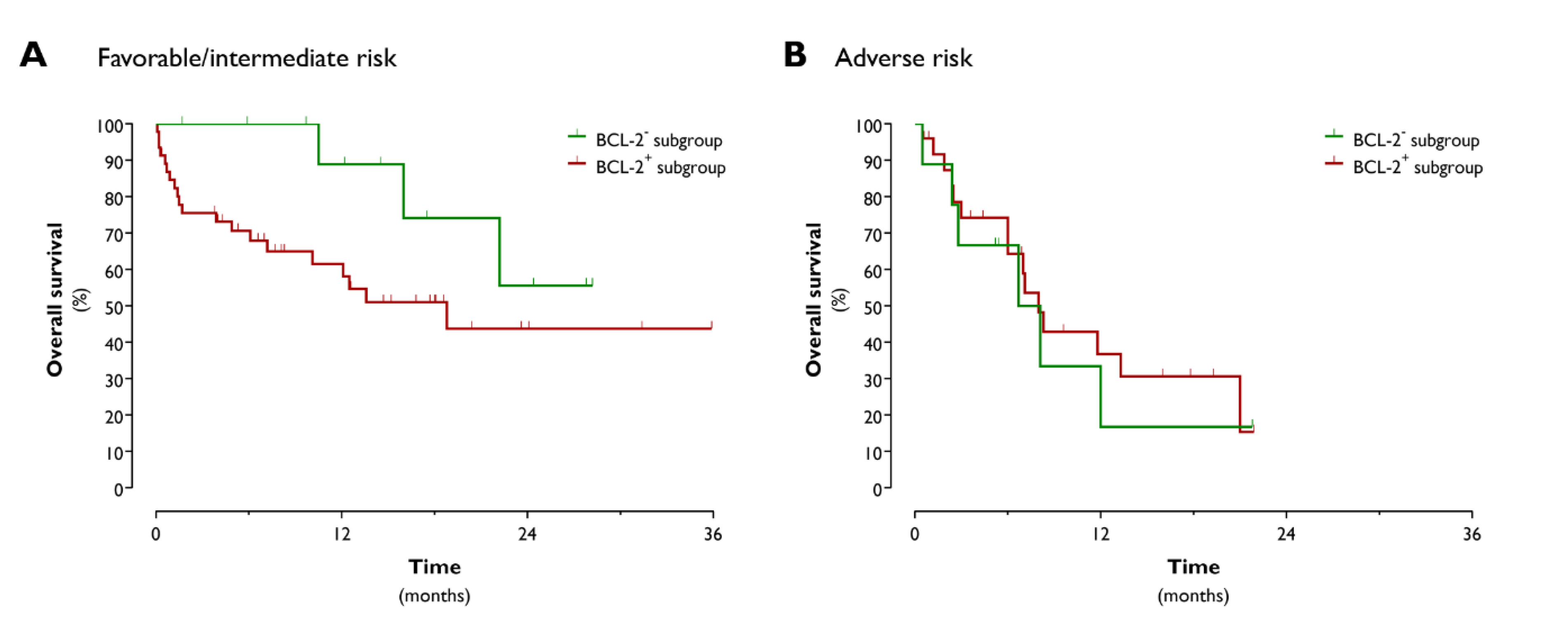
3.4. Absence of BCL-2 Expression Identifies a Subgroup of AML Patients with Good Response to Chemotherapy and Favorable OS
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Dohner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Buchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [Green Version]
- Lichtman, M.A. A historical perspective on the development of the cytarabine (7days) and daunorubicin (3days) treatment regimen for acute myelogenous leukemia: 2013 the 40th anniversary of 7+3. Blood Cells Mol. Dis. 2013, 50, 119–130. [Google Scholar] [CrossRef]
- Cruijsen, M.; Lübbert, M.; Wijermans, P.; Huls, G. Clinical results of hypomethylating agents in AML treatment. J. Clin. Med. 2014, 4, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.; et al. (Eds.) SEER Cancer Statistics Review 1975–2017; National Cancer Institute: Bethesda, MD, USA. Available online: https://seer.cancer.gov/csr/1975_2017/browse_csr.php?sectionSEL=13&pageSEL=sect_13_table.16 (accessed on 9 September 2020).
- DiNardo, C.D.; Wei, A.H. How I treat acute myeloid leukemia in the era of new drugs. Blood 2020, 135, 85–96. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, C.D.; Jonas, B.A.; Pullarkat, V.; Thirman, M.J.; Garcia, J.S.; Wei, A.H.; Konopleva, M.; Döhner, H.; Letai, A.; Fenaux, P.; et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. N. Engl. J. Med. 2020, 383, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.J.; Wilmot, B.; Bottomly, D.; Kurtz, S.E.; Eide, C.A.; Damnernsawad, A.; Romine, K.; Patel, S.; Druker, B.J.; McWeeney, S.K.; et al. Biomarkers predicting venetoclax sensitivity and strategies for venetoclax combination treatment. Blood 2018, 132, 175. [Google Scholar] [CrossRef]
- Wei, A.H.; Chua, C.C.; Tiong, I.S.; Fong, C.Y.; Ting, S.B.; Macraild, S.; Salmon, J.M.; Ivey, A.; Nguyen, J.; Yuen, F.; et al. Molecular patterns of response and outcome in the chemotherapy and venetoclax in elderly AML trial (CAVEAT study). Blood 2018, 132, 333. [Google Scholar] [CrossRef]
- Konopleva, M.; Pollyea, D.A.; Potluri, J.; Chyla, B.; Hogdal, L.; Busman, T.; McKeegan, E.; Salem, A.H.; Zhu, M.; Ricker, J.L.; et al. Efficacy and biological correlates of response in a phase II study of venetoclax monotherapy in patients with acute myelogenous leukemia. Cancer Discov. 2016, 6, 1106–1117. [Google Scholar] [CrossRef] [Green Version]
- Chyla, B.; Daver, N.; Doyle, K.; McKeegan, E.; Huang, X.; Ruvolo, V.; Wang, Z.; Chen, K.; Souers, A.; Leverson, J.; et al. Genetic biomarkers of sensitivity and resistance to venetoclax monotherapy in patients with relapsed acute myeloid leukemia. Am. J. Hematol. 2018, 93, E202–E205. [Google Scholar] [CrossRef] [Green Version]
- Chua, C.C.; Reynolds, J.; Salmon, J.M.; Fong, C.; Ting, S.B.; Tiong, I.S.; Fleming, S.; MacRaild, S.; Moujalled, D.M.; Pomilio, G.; et al. Anti-leukemic activity of single agent venetoclax in newly diagnosed acute myeloid leukemia: A sub-set analysis of the CAVEAT study. Blood 2019, 134, 462. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Tiong, I.S.; Quaglieri, A.; MacRaild, S.; Loghavi, S.; Brown, F.C.; Thijssen, R.; Pomilio, G.; Ivey, A.; Salmon, J.M.; et al. Molecular patterns of response and treatment failure after frontline venetoclax combinations in older patients with AML. Blood 2020, 135, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.H.; Montesinos, P.; Ivanov, V.; DiNardo, C.D.; Novak, J.; Laribi, K.; Kim, I.; Stevens, D.A.; Fiedler, W.; Pagoni, M.; et al. Venetoclax plus LDAC for newly diagnosed AML ineligible for intensive chemotherapy: A phase 3 randomized placebo-controlled trial. Blood 2020, 135, 2137–2145. [Google Scholar] [CrossRef] [PubMed]
- Panuzzo, C.; Signorino, E.; Calabrese, C.; Ali, M.S.; Petiti, J.; Bracco, E.; Cilloni, D. Landscape of tumor suppressor mutations in acute myeloid leukemia. J. Clin. Med. 2020, 9, 802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, S.M.; Thomas, D.; Corces-Zimmerman, M.R.; Xavy, S.; Rastogi, S.; Hong, W.J.; Zhao, F.; Medeiros, B.C.; Tyvoll, D.A.; Majeti, R. Isocitrate dehydrogenase 1 and 2 mutations induce BCL-2 dependence in acute myeloid leukemia. Nat. Med. 2015, 21, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Bisaillon, R.; Moison, C.; Thiollier, C.; Krosl, J.; Bordeleau, M.E.; Lehnertz, B.; Lavallee, V.P.; MacRae, T.; Mayotte, N.; Labelle, C.; et al. Genetic characterization of ABT-199 sensitivity in human AML. Leukemia 2020, 34, 63–74. [Google Scholar] [CrossRef]
- Bacher, U.; Shumilov, E.; Flach, J.; Porret, N.; Joncourt, R.; Wiedemann, G.; Fiedler, M.; Novak, U.; Amstutz, U.; Pabst, T. Challenges in the introduction of next-generation sequencing (NGS) for diagnostics of myeloid malignancies into clinical routine use. Blood Cancer J. 2018, 8, 113. [Google Scholar] [CrossRef] [Green Version]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- O’Donnell, M.R.; Abboud, C.N.; Altman, J.; Appelbaum, F.R.; Arber, D.A.; Attar, E.; Borate, U.; Coutre, S.E.; Damon, L.E.; Goorha, S.; et al. NCCN clinical practice guidelines acute myeloid leukemia. J. Natl. Compr. Cancer Netw. 2012, 10, 984–1021. [Google Scholar] [CrossRef] [Green Version]
- Van Tendeloo, V.F.; Van de Velde, A.; Van Driessche, A.; Cools, N.; Anguille, S.; Ladell, K.; Gostick, E.; Vermeulen, K.; Pieters, K.; Nijs, G.; et al. Induction of complete and molecular remissions in acute myeloid leukemia by Wilms’ tumor 1 antigen-targeted dendritic cell vaccination. Proc. Natl. Acad. Sci. USA 2010, 107, 13824–13829. [Google Scholar] [CrossRef] [Green Version]
- Anguille, S.; Van de Velde, A.L.; Smits, E.L.; Van Tendeloo, V.F.; Juliusson, G.; Cools, N.; Nijs, G.; Stein, B.; Lion, E.; Van Driessche, A.; et al. Dendritic cell vaccination as postremission treatment to prevent or delay relapse in acute myeloid leukemia. Blood 2017, 130, 1713–1721. [Google Scholar] [CrossRef] [Green Version]
- Fedchenko, N.; Reifenrath, J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue—A review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [PubMed] [Green Version]
- Campos, L.; Rouault, J.P.; Sabido, O.; Oriol, P.; Roubi, N.; Vasselon, C.; Archimbaud, E.; Magaud, J.P.; Guyotat, D. High expression of bcl-2 protein in acute myeloid leukemia cells is associated with poor response to chemotherapy. Blood 1993, 81, 3091–3096. [Google Scholar] [PubMed]
- DiNardo, C.D.; Garcia-Manero, G.; Pierce, S.; Nazha, A.; Bueso-Ramos, C.; Jabbour, E.; Ravandi, F.; Cortes, J.; Kantarjian, H. Interactions and relevance of blast percentage and treatment strategy among younger and older patients with acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS). Am. J. Hematol. 2016, 91, 227–232. [Google Scholar] [PubMed] [Green Version]
- Bradbury, D.A.; Zhu, Y.M.; Russell, N.H. Bcl-2 expression in acute myeloblastic leukaemia: Relationship with autonomous growth and CD34 antigen expression. Leuk. Lymphoma 1997, 24, 221–228. [Google Scholar]
- Dunphy, C.H.; Tang, W. The value of CD64 expression in distinguishing acute myeloid leukemia with monocytic differentiation from other subtypes of acute myeloid leukemia: A flow cytometric analysis of 64 cases. Arch. Pathol. Lab. Med. 2007, 131, 748–754. [Google Scholar] [PubMed]
- Cilloni, D.; Gottardi, E.; De Micheli, D.; Serra, A.; Volpe, G.; Messa, F.; Rege-Cambrin, G.; Guerrasio, A.; Divona, M.; Lo Coco, F.; et al. Quantitative assessment of WT1 expression by real time quantitative PCR may be a useful tool for monitoring minimal residual disease in acute leukemia patients. Leukemia 2002, 16, 2115–2121. [Google Scholar]
- Cilloni, D.; Renneville, A.; Hermitte, F.; Hills, R.K.; Daly, S.; Jovanovic, J.V.; Gottardi, E.; Fava, M.; Schnittger, S.; Weiss, T.; et al. Real-time quantitative polymerase chain reaction detection of minimal residual disease by standardized WT1 assay to enhance risk stratification in acute myeloid leukemia: A European LeukemiaNet study. J. Clin. Oncol. 2009, 27, 5195–5201. [Google Scholar]
- Metzeler, K.H.; Herold, T.; Rothenberg-Thurley, M.; Amler, S.; Sauerland, M.C.; Gorlich, D.; Schneider, S.; Konstandin, N.P.; Dufour, A.; Braundl, K.; et al. Spectrum and prognostic relevance of driver gene mutations in acute myeloid leukemia. Blood 2016, 128, 686–698. [Google Scholar]
- Bensi, L.; Longo, R.; Vecchi, A.; Messora, C.; Garagnani, L.; Bernardi, S.; Tamassia, M.G.; Sacchi, S. Bcl-2 oncoprotein expression in acute myeloid leukemia. Haematologica 1995, 80, 98–102. [Google Scholar]
- Andreeff, M.; Jiang, S.; Zhang, X.; Konopleva, M.; Estrov, Z.; Snell, V.E.; Xie, Z.; Okcu, M.F.; Sanchez-Williams, G.; Dong, J.; et al. Expression of Bcl-2-related genes in normal and AML progenitors: Changes induced by chemotherapy and retinoic acid. Leukemia 1999, 13, 1881–1892. [Google Scholar]
- van Stijn, A.; van der Pol, M.A.; Kok, A.; Bontje, P.M.; Roemen, G.M.; Beelen, R.H.; Ossenkoppele, G.J.; Schuurhuis, G.J. Differences between the CD34+ and CD34− blast compartments in apoptosis resistance in acute myeloid leukemia. Haematologica 2003, 88, 497–508. [Google Scholar] [PubMed]
- Pei, S.; Pollyea, D.A.; Gustafson, A.; Stevens, B.M.; Minhajuddin, M.; Fu, R.; Riemondy, K.A.; Gillen, A.E.; Sheridan, R.M.; Kim, J.; et al. Monocytic subclones confer resistance to venetoclax-based therapy in patients with acute myeloid leukemia. Cancer Discov. 2020, 10, 536–551. [Google Scholar] [CrossRef] [PubMed]
- Kuusanmäki, H.; Leppä, A.M.; Pölönen, P.; Kontro, M.; Dufva, O.; Deb, D.; Yadav, B.; Brück, O.; Kumar, A.; Everaus, H.; et al. Phenotype-based drug screening reveals association between venetoclax response and differentiation stage in acute myeloid leukemia. Haematologica 2020, 105, 708–720. [Google Scholar] [CrossRef] [PubMed]
- Karakas, T.; Miething, C.C.; Maurer, U.; Weidmann, E.; Ackermann, H.; Hoelzer, D.; Bergmann, L. The coexpression of the apoptosis-related genes bcl-2 and wt1 in predicting survival in adult acute myeloid leukemia. Leukemia 2002, 16, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Lyu, X.; Xin, Y.; Mi, R.; Ding, J.; Wang, X.; Hu, J.; Fan, R.; Wei, X.; Song, Y.; Zhao, R.Y. Overexpression of Wilms tumor 1 gene as a negative prognostic indicator in acute myeloid leukemia. PLoS ONE 2014, 9, e92470. [Google Scholar] [CrossRef] [Green Version]
- Garg, M.; Moore, H.; Tobal, K.; Liu Yin, J.A. Prognostic significance of quantitative analysis of WT1 gene transcripts by competitive reverse transcription polymerase chain reaction in acute leukaemia. Br. J. Haematol. 2003, 123, 49–59. [Google Scholar]
- Ritter, M.; Kim, T.D.; Lisske, P.; Thiede, C.; Schaich, M.; Neubauer, A. Prognostic significance of N-RAS and K-RAS mutations in 232 patients with acute myeloid leukemia. Haematologica 2004, 89, 1397–1399. [Google Scholar]
- DiNardo, C.D.; Cortes, J.E. Mutations in AML: Prognostic and therapeutic implications. Hematol. Am. Soc. Hematol. Educ. Program 2016, 2016, 348–355. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, E.I.; Gawish, H.H.; Al Azizi, N.M.; Elhefni, A.M. The prognostic impact of K-RAS mutations in adult acute myeloid leukemia patients treated with high-dose cytarabine. Onco Targets Ther. 2011, 4, 115–121. [Google Scholar]
- Liu, X.; Ye, Q.; Zhao, X.P.; Zhang, P.B.; Li, S.; Li, R.Q.; Zhao, X.L. RAS mutations in acute myeloid leukaemia patients: A review and meta-analysis. Clin. Chim. Acta 2019, 489, 254–260. [Google Scholar] [CrossRef]
- Stirewalt, D.L.; Radich, J.P. The role of FLT3 in haematopoietic malignancies. Nat. Rev. Cancer 2003, 3, 650–665. [Google Scholar] [CrossRef] [PubMed]
- Daver, N.; Schlenk, R.F.; Russell, N.H.; Levis, M.J. Targeting FLT3 mutations in AML: Review of current knowledge and evidence. Leukemia 2019, 33, 299–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Patients | BCL-2− | BCL-2+ | |
|---|---|---|---|
| H-Score 0–20 | H-Score 21–300 | ||
| Number (%) | 112 | 21 (22.6%) | 72 (77.4%) |
| Median age in years (range) | 65 yr (19–92 yr) | 67 yr (24–87 yr) | 67 yr (19–89 yr) |
| Male (%) | 60 (53.6%) | 10 (47.6%) | 42 (58.3%) |
| Female (%) | 52 (46.4%) | 11 (52.4%) | 30 (41.7%) |
| De novo AML (%) | 78 (69.6%) | 14 (66.7%) | 49 (68.1%) |
| Secondary AML (%) | 34 (30.4%) | 7 (33.3%) | 23 (31.9%) |
| ELN/Cytogenetic risk | |||
| Favorable | 26 (25.0%) | 7 (33.3%) | 14 (19.7%) |
| Intermediate | 41 (39.4%) | 5 (23.8%) | 32 (45.1%) |
| Adverse | 37 (35.6%) | 9 (42.9%) | 25 (35.2%) |
| BCL-2− | BCL-2+ | p-Value | |
|---|---|---|---|
| (H-Score 0-20) | (H-Score 21-300) | ||
| DNA methylation | |||
| DNMT3A | 5 (27.8%) | 15 (24.6%) | >0.05 |
| TET2 | 4 (22.2%) | 16 (26.2%) | >0.05 |
| IDH1 | 1 (5.6%) | 6 (9.8%) | n.d. |
| IDH2 | 3 (16.7%) | 5 (8.2%) | >0.05 |
| Tumor suppressor genes | |||
| TP53 | 3 (16.7%) | 9 (14.8%) | n.d. |
| WT1 | 0 (0.0%) | 6 (9.8%) | >0.05 |
| Epigenetic modifiers | |||
| ASXL1 | 3 (16.7%) | 3 (4.9%) | >0.05 |
| BCOR1 | 2 (11.1%) | 7 (11.5%) | n.d. |
| EZH2 | 0 (0.0%) | 1 (1.6%) | n.d. |
| KMT2A | 0 (0.0%) | 0 (0.0%) | n.d. |
| Transcription factors | |||
| CEBPA | 0 (0.0%) | 6 (9.2%) | n.d. |
| RUNX1 | 4 (22.2%) | 9 (14.8%) | >0.05 |
| SETBP1 | 0 (0.0%) | 0 (0.0%) | n.d. |
| Nucleophosmin 1 | |||
| NPM1 | 6 (31.6%) | 18 (27.7%) | >0.05 |
| Activated signaling | |||
| CBL | 0 (0.0%) | 0 (0.0%) | n.d. |
| FLT3 | 1 (5.6%) | 20 (30.8%) | =0.0331 |
| JAK2 | 1 (5.6%) | 4 (6.6%) | n.d. |
| KIT | 0 (0.0%) | 3 (4.6%) | n.d. |
| KRAS | 4 (22.2%) | 1 (1.6%) | n.d. |
| MPL | 1 (5.6%) | 0 (0.0%) | n.d. |
| NRAS | 0 (0.0%) | 10 (16.4%) | =0.0626 |
| RNA Splicing | |||
| SF3B1 | 1 (5.6%) | 4 (6.6%) | n.d. |
| SRSF2 | 3 (16.7%) | 4 (6.6%) | >0.05 |
| U2AF1 | 1 (5.6%) | 2 (3.3%) | n.d. |
| Cohesin complex | |||
| STAG2 | 2 (11.1%) | 4 (6.6%) | n.d. |
| Other | |||
| CALR | 0 (0.0%) | 1 (1.6%) | n.d. |
| CSF3R, ETNK1 and ZRSR2 | 0 (0.0%) | 0 (0.0%) | n.d. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
haes, I.D.; Dendooven, A.; Mercier, M.L.; Puylaert, P.; Vermeulen, K.; Kockx, M.; Deiteren, K.; Maes, M.-B.; Berneman, Z.; Anguille, S. Absence of BCL-2 Expression Identifies a Subgroup of AML with Distinct Phenotypic, Molecular, and Clinical Characteristics. J. Clin. Med. 2020, 9, 3090. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103090
haes ID, Dendooven A, Mercier ML, Puylaert P, Vermeulen K, Kockx M, Deiteren K, Maes M-B, Berneman Z, Anguille S. Absence of BCL-2 Expression Identifies a Subgroup of AML with Distinct Phenotypic, Molecular, and Clinical Characteristics. Journal of Clinical Medicine. 2020; 9(10):3090. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103090
Chicago/Turabian Stylehaes, Inke De, Amélie Dendooven, Marie Le Mercier, Pauline Puylaert, Katrien Vermeulen, Mark Kockx, Kathleen Deiteren, Marie-Berthe Maes, Zwi Berneman, and Sébastien Anguille. 2020. "Absence of BCL-2 Expression Identifies a Subgroup of AML with Distinct Phenotypic, Molecular, and Clinical Characteristics" Journal of Clinical Medicine 9, no. 10: 3090. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9103090