
Augmenting Performance: A Systematic Review of Optical See-Through Head-Mounted Displays in Surgery



1
Department of Medical Biophysics, University of Toronto, Toronto, ON M5S 1A1, Canada
2
Schulich Heart Program, Sunnybrook Health Sciences Centre, Toronto, ON M4N 3M5, Canada
3
Physical Sciences Platform, Sunnybrook Research Institute, Toronto, ON M4N 3M5, Canada
*
Author to whom correspondence should be addressed.
J. Imaging 2022, 8(7), 203; https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8070203
Submission received: 24 June 2022
/
Revised: 15 July 2022
/
Accepted: 18 July 2022
/
Published: 20 July 2022
(This article belongs to the Special Issue The Application of Imaging Technology in Medical Intervention and Surgery)
Abstract
:We conducted a systematic review of recent literature to understand the current challenges in the use of optical see-through head-mounted displays (OST-HMDs) for augmented reality (AR) assisted surgery. Using Google Scholar, 57 relevant articles from 1 January 2021 through 18 March 2022 were identified. Selected articles were then categorized based on a taxonomy that described the required components of an effective AR-based navigation system: data, processing, overlay, view, and validation. Our findings indicated a focus on orthopedic () and maxillofacial surgeries (). For preoperative input data, computed tomography (CT) (), and surface rendered models () were most commonly used to represent image information. Virtual content was commonly directly superimposed with the target site (); this was achieved by surface tracking of fiducials (), external tracking (), or manual placement (). Microsoft HoloLens devices ( in 2021, in 2022) were the most frequently used OST-HMDs; gestures and/or voice () served as the preferred interaction paradigm. Though promising system accuracy in the order of 2–5 mm has been demonstrated in phantom models, several human factors and technical challenges—perception, ease of use, context, interaction, and occlusion—remain to be addressed prior to widespread adoption of OST-HMD led surgical navigation.
1. Introduction
In their 1994 paper, Milgram and Kishino detail a continuum to describe the ways in which virtual and real environments can be combined to create different experiences for a user [1]. The left side of the spectrum in Figure 1 describes a fully real environment with no virtual elements; conversely, the right side of the spectrum details an environment which consists of an immersive, fully virtual experience, where a user can interact with synthetic elements. Augmented reality (AR) encompasses a combination of real world and virtual components and is the focus of this proposed work (Figure 1). Extended reality (XR) is a recently coined term used to broadly describe immersive technologies, such as AR, virtual reality (VR), and mixed reality, under a single umbrella.
1.1. Medical Augmented Reality
Augmented reality led guidance for surgical navigation was first suggested nearly 40 years ago, where Kelly et al. (1982) superimposed tumor outlines from preoperative CT data into the view of a surgical microscope rigidly attached to a stereotactic frame [2]. Though the accuracy of this initial system was not acceptable for clinical deployment, the contributions from this work inspired future investigations into frameless stereotaxy (or image-guided surgery) in neurosurgery [3], and today, image-guided surgery is routinely used for treatment of a multitude of brain disorders.
2. Background
In the context of AR visualization, displays can be classified into three separate categories: hand-held displays, spatial display systems, and head-mounted displays (HMDs), based on their position between the viewer and the real environment [15]. A fundamental requirement of an AR system is the ability to combine, register, and display interactive 3D virtual content with real-world scenes in real time [15]. Although the focus here is on HMDs, we also briefly introduce handheld and spatial display systems for context [8,13,15,16].
2.1. Handheld and Spatial Displays
Hand-held displays include video see-through displays like mobile devices (smartphones or tablets) which are held near the user. Hand-held AR has seen broad uptake into applications in entertainment, product marketing, education, and social networking [17]. With the current computing power of smartphone hardware, hand-held AR experiences can be effectively delivered to the vast user base of billions of device owners; however, the ergonomic limitations of mobile AR, such as the small screen size for augmenting virtual content and requirement for hand-held interaction, limit the effective use cases [17]. Spatial display systems are placed statically within an environment and include screen-based video see-through displays and projective displays [15]. Video see-through spatial display systems, such as conventional 2D and 3D monitors or televisions, blend virtual content with real imagery for user consumption. A limitation of spatial AR is the static nature of the display and, due to remote viewing, the requirement for a user to create a mental mapping to understand the context and placement of virtually augmented information shown on the display when mapped in the real world [18].
2.2. See-Through Head-Mounted Displays
See-through HMDs provide hands-free interaction, direct projection of virtually augmented entities into the field of view (FOV) of the user, and 3D viewing capacity via stereoscopic rendering. See-through HMDs can be further classified into video see-through HMD (Figure 2a) and OST-HMD (Figure 2b) categories based on their mechanism of display [19]. Video see-through HMDs make use of front-facing cameras to record and digitize the scene before combining with computer-generated virtual images, limiting the user view to the camera field-of-view and visual display resolutions, and potentially introducing lag [16] and geometric aberrations, such as distorted spatial perception [20]. Recent work has investigated the use of non-orthostereoscopic video see-through HMDs to minimize the contribution of these geometric aberrations to perceptual error [21]. Optical see-through HMDs are less obtrusive to the user and allow for an unhindered view of reality and natural stereo vision with no additional disruption to their view due to lag or reduced resolution. Optical see-through HMDs make use of beam splitting holographic optical elements to visualize computer generated graphics [19], although, they have FOV and contrast limitations due to the quality of display technology and require additional calibration to accommodate for the eye positions of an individual user [22]. Additionally, there are challenges with occlusion in OST-HMDs, where distant virtual content will appear on top of nearer real objects [23]. For uses in image guidance for safety-critical applications, optical see-through systems have shown a clear benefit over video see-through systems due to the ability of the wearer to maintain an uninterrupted and instantaneous view of the scene [24,25]. In this review, we focus specifically on the evaluation of optical see-through HMDs.
Optical See-Through Head-Mounted Displays
Optical see-through HMDs were developed and first introduced in the 1960s, with Ivan Sutherland demonstrating the first computer graphics-based HMD in 1968 using miniaturized cathode-ray tubes as stereoscopic displays and a mechanical tracker to provide head position and orientation in real-time [26]. Though there have been significant recent improvements to HMD technology, the basic display configuration of OST-HMDs remains relatively unchanged from the designs of the early 2000s which used half-silvered mirrors or beam combiners to merge virtual content with the real view [27]. These OST-HMDs are operated by rendering virtual content on a 2D micro display outside the FOV of a user and redirecting light rays to the eye of the wearer using a beam combiner [10]. Lenses are placed between the beam combiner and display to focus the virtual images on a semitransparent surface of projection (SSP) at a viewing distance that is comfortable for the wearer, allowing the wearer to perceive 3D virtual augmentations through stereoscopic vision of the two 2D SSPs [28].
2.3. Overview of Commercially Available Optical See-Through Head-Mounted Displays
Coinciding with the ongoing COVID-19 pandemic and global paradigm shift to remote work, there have been significant investments by technology companies, including Google, Apple, Microsoft, and Meta (Facebook), into AR and VR HMD technology in the creation of their own renditions of 3D virtual worlds to enable enhanced social connection and telepresence (metaverse). We focus solely on outlining the relevant commercially available OST-HMDs and do not consider video see-through HMDs and virtual reality HMDs. Images of the relevant commercially available OST-HMDs are included in Figure 3. A detailed summary of the relevant OST-HMDs and their associated technical specifications are included in Table 1.
As indicated in Table 1, all the catalogued OST-HMDs have six-degrees of freedom (6DoF) simultaneous localization and mapping (SLAM) capabilities. Simultaneous localization and mapping combines multiple sensor inputs to create, and continuously update, a construction of an unknown environment and allow for the HMD to know its position and orientation (pose) within the environment. With continual knowledge of HMD pose, it becomes possible to place or anchor virtually augmented entities to locations in the real world and create an immersive virtual experience.
Virtual Model Alignment
A foundational aspect of AR is the capacity for accurate spatial alignment of virtual content with real objects in the world [8]. Conventional strategies for HMD-led tracking of real objects rely on 2D feature-matching of square marker fiducials captured through input video from a red-green-blue (RGB) camera (Figure 4).
Sensor calibration and estimation of the intrinsic and extrinsic parameters of an RGB camera is a fundamental requirement prior to performing any sort of computer vision-based task, as it enables the relation of points in the world coordinate frame to their respective image projections on the camera plane through perspective projection [29] (Figure 4). The intrinsic parameters (focal length, principal points, and skew) are computed once for a specific RGB camera using a planar chessboard-based calibration procedure [30]. The extrinsic parameters (rotation and translation) are constant provided the camera coordinate frame does not change with respect to the world.
In most cases, however, the wearer of the HMD will be moving around the environment, so the camera coordinate frame will be constantly changing with respect to the world, requiring the extrinsic parameters to be recomputed each frame; this is where marker tracking is of value, as it allows the precise localization of the HMD (and camera coordinate frame) relative to the markers through knowledge of marker size and the use of our intrinsic parameters that defined a projection matrix [31].
Simultaneous localization and mapping allows for HMD localization within the world; however, it does not provide the same accuracy as marker-based localization and is subject to drift caused by error propagation over time [32]. Though the accuracy and stability of SLAM is not enough to rely on for precise tasks, it can be invaluable as an alternative method to maintain alignment of virtual entities to real objects during instances where marker-based localization is unstable or lost [33].
2.4. Augmented Reality Perception
Although there have been significant improvements to the performance and comfort of OST-HMDs, limitations associated with human perception remain to be addressed. In the context of this review, perception refers to the quantitative assessment of a user’s interpretation and understanding of virtually augmented elements. Primary contributors to perceptual limitations of current OST-HMDs include: the small FOV of virtually augmented content; the obtrusiveness and weight of the device [34]; the low luminance of the micro-displays; the requirement for frequent recalibrations to maintain precise spatial alignment of virtual content [22]; depth perception and depth cues [35]; and the perceptual conflicts between the 3D view of the real world and the 2D virtual images on the stereoscopic lenses [10,36,37]. With the recent influx of commercial interest into HMD technology, we anticipate that the limitations due to device form factor, and challenges with FOV and display luminance will be addressed with upcoming device iterations. Instead, we will focus on a brief discussion of the other factors which contribute to perceptual challenges in commercially available OST-HMDs. Perhaps the most important is depth perception. Section 2.4.1 highlights visual cues and subsequent sections summarize how these are addressed by OST-HMDs.
2.4.1. Depth Perception and Depth Cues
The human visual system relies on several sources of perceptual information related to depth, or depth cues, to perceive depth from imagery [35]. Cutting and Vishton have identified nine depth cues that are essential to depth perception; we will discuss the most prominent in detail: occlusion, binocular disparity, motion perspective, relative size/density, and vergence and accommodation [38]. Occlusion refers to the blocking of a distant object by a nearer one. Binocular disparity is the difference between image projections to left and right retinal images based on the horizontal separation of the eyes. Motion perspective describes the different inferred velocities of moving objects at different distances from the observer. Relative size refers to retinal angle of projection of similarly sized objects at different distances, where the farther object will project to a smaller retinal angle [35]. Accommodation refers to the changing shape of the human eye to bring objects into focus, and vergence describes the rotation of the left and right eyes to fixate on an object [9]. To fixate on a near object, the pupils converge and rotate towards each other. To fixate on a distant object, the pupils diverge and rotate away from each other. Binocular disparity and vergence and accommodation contribute to depth perception via physiological cues, whereas occlusion, motion perspective, and relative size/density rely on psychological cues [39]. Through the effective combination of these cues, it is possible to create imagery which will enable a user to perceive depth.
2.4.2. Interpupillary Distance
To render a virtual scene on an OST-HMD, we require knowledge of the internal projection parameters of the eye cameras of the device. These internal projection parameters are typically provided by the manufacturer and will function to define the left and right eye virtual cameras. An additional metric, the interpupillary distance (IPD) of the user, is used to define the horizontal distance offset between the left and right virtual eye cameras to ensure comfortable 3D perception of virtually augmented content through binocular disparity of the 2D image pair. Early OST-HMDs included a predefined horizontal distance offset based on the average IPD of a typical user; however, this was not ideal as miscalibrations in the IPD can result in poor depth perception of the displayed virtual content [40]. Both the HoloLens and Magic Leap device classes include an application to estimate IPD which is launched when a new user wears the HMD. The second-generation HoloLens and Magic Leap headsets improve on the accuracy of IPD estimation of their predecessors using active-eye tracking. A secondary benefit of the active-eye tracking incorporated into second generation headsets is the capacity for adaptive correction for changes in the positioning of the HMD relative to the eyes of a wearer via additional corrections made to virtual content augmentation, reducing the contribution to distortion of virtual content [23].
2.4.3. Vergence-Accommodation Conflict
Vergence-accommodation conflict is not unique to HMDs and is inherent to all conventional stereoscopic 3D displays which simulate 3D perception from a pair of 2D perspective images using binocular disparity and other depth cues [36]. To enable 3D perception of augmented virtual content, an OST-HMD requires an optical combiner that is positioned in front of the eye of a wearer to combine the optical path of the virtual display and real scene [36]. Vergence-accommodation conflict arises from the inability to render correct focus cues for the augmented virtual information which can appear at different distances from the corresponding virtual image plane [36,37] and can contribute to blurred content and visual fatigue during prolonged use [9]. In traditional stereoscopic HMDs, the vergence distance varies based on the depth of targets (virtual or real), whereas the accommodation, or focal distance, is fixed at the distance of the focal plane of the virtual display [9].
Depth of focus (F) refers to the range of distances in display space within which an image appears sharp and correctly formed and is measured in diopters (D), a standard depth of focus estimate is on the order of D [10,41]. Related to depth of focus is depth of field (DOF): the depth interval over which a stimulus remains in focus and the accommodative response of a viewer does not substantially change [41]. Depth of field is inversely related to depth of focus as [41]. For a given fixation distance (P), we can estimate the near () and far () DOF as [41]:
As described earlier, the HoloLens 1 and 2 HMDs include a single fixed focal plane, set at a distance of 1.5–2 m [42,43]. In contrast, the Magic Leap 1 HMD includes two fixed focal planes, one for content near the user at a distance of 1 m and a second for room scale content at a distance of 3 m. With Magic Leap devices, the active focal plane is adaptively selected based on the rendering distance of virtual content. Multiple focal planes can contribute to reduced vergence-accommodation conflict; however, this occurs only when the virtual content appears within a threshold of the distance of the active focal plane. For example, with a focal plane distance of 1 m, we use Equation (1) to compute an estimated depth of field range from 0.67–2 m, meaning that within this threshold virtual content will appear without blur. Current commercially available OST-HMDs are not intended for augmenting virtual content in the peripersonal space (roughly 0.3–0.5 m from the wearer) and, as a consequence, can introduce discomfort and content blur for some users with long sessions.
3. Methods
3.1. Literature Search Strategy
A systematic literature review was conducted using Google Scholar and the following search terms (surgery “head mounted display” AND “augmented reality” OR “mixed reality” AND “optical see through” OR “hololens” OR “magic leap” OR “google glass”). The literature search was performed on 18 March 2022, and included research articles from 1 January 2021 through the current date.
The Google Scholar search resulted in 441 total records, from which we included 57 articles in the review. Duplicate articles, non-peer reviewed manuscripts, and work that did not: (1) describe the use of an OST-HMD; (2) indicate a focus on a surgical application; and (3) investigate the application of an OST-HMD in a surgical setting were removed. Further details of our systematic review search strategy are included in Figure 5.
In Figure 6, we include a chart depicting the article frequency categorized by the publication year. For the years 2014 to 2020, we include the data provided in a recent review of OST-HMD indications in surgery by Birlo et al. [6]. In our review, we used similar search terms and criteria as Birlo et al. to provide comparable data. An uptick in the frequency of publications involving the use of OST-HMDs for surgical applications is visible and coincides with the introduction of commercially available HMDs: the first edition Google Glass OST-HMD in 2014 and the Microsoft HoloLens 1 OST-HMD in 2016.
3.2. Review Strategy and Taxonomy
In Figure 7, we detail a taxonomy of the required components of an effective AR-based navigation solution for image guided surgery. Our taxonomy is adapted from the Data, Visualization processing, View (DVV) framework presented by Kersten-Oertel et al. [44]. Core requirements include preoperative image data (data); image processing (processing); calibration and tracking for augmented content overlay (overlay); interaction, display device, and perception location (view); and performance assessment metrics (validation).
4. Results and Discussion
4.1. Distribution of Relevant Articles by Surgical Application
In Figure 8, a breakdown of the 57 papers included in our survey is depicted based on their general surgical speciality. The majority of papers () focused on orthopedic applications, such as osteotomy [45,46,47,48,49] and K-wire placement [50,51], with the second largest () involving maxillofacial surgery procedures, such as tumor resection [52] and craniofacial fibrous dysplasia [53,54]. The prevalence of OST-HMD investigation in orthopedic and maxillofacial surgeries is likely due to the rigid nature of the relevant anatomy, the availability of consistent landmarks for registration and tracking, and the prevalence of commercially available surgical navigation suites.
General applications (), general surgery (), neurosurgery (), robot-assisted surgery (), and vascular surgery () were the next most prevalent. Robot-assisted surgery applications included orthopedic applications [55], general bedside tasks [56], and endoluminal interventions [57]. Papers focused on general surgery and associated applications included telementoring [58], teleproctoring [59], surgical navigation [60], and liver resection [61]. Neurosurgery-related applications included incision planning [62,63], navigation [64,65], and complex craniotomies [66]. Vascular surgery related papers focused on use for percutaneous femoral artery access [67] and tumor puncture [68].
Laparoscopic surgery (), reconstructive surgery (), radiotherapy (), dental surgery (), and heart surgery () were the last categories surveyed. Reconstructive surgery included orbital floor reconstruction [69] and radiotherapy applications involved AR-based patient positioning [70,71]. Laparoscopic surgery applications included cholecystectomy [72] and general laparoscopic surgery [73]. Heart surgery related applications included guiding the targeted delivery of media to the surface of the infarcted heart in regenerative medicine [33]. Otolaryngology applications included median neck and brachial cyst excision [74] and neck cancer [75].
4.2. Data
In Table 2, the articles are categorized based on the data type used for surgical guidance.
4.2.1. Preoperative Image Data
The majority of papers made use of preoperative CT data as the input to the surgical guidance strategy, corresponding with the frequent application space of orthopedic surgery and the enhanced ability of CT to generate geometrically accurate representations of rigid anatomical structures, such as bone [45,76,77]. The second most frequently used data type was MRI, either as a standalone data type [62,72,78] or in combination with CT [49,52,53]. Magnetic resonance imaging has better sensitivity than CT when imaging soft tissue structures; however, it is less geometrically precise [79] and has less signal intensity when imaging bony structures. The registration of MRI and CT data is advantageous in situations where geometrically precise bone imaging and soft tissue information are used in tandem. Prerecorded video content was used in the case of an immersive telementoring solution to support the remote surgeon during a simulated task [58].
4.2.2. Intraoperative Image Data
The most frequently used intraoperative data strategy was X-ray fluoroscopy, which is commonly used in orthopedic procedures as a real-time 2D imaging strategy to confirm the current navigation precision prior to performing a surgical action [57,80,81]. Ultrasound imaging was the second most frequently used form of intraoperative data, and is commonly used as a tool for confirming real-time tissue targets in needle biopsy procedures [82,83]. Telestrations, such as virtual arrows and other virtual annotations were common in telementoring and teleproctoring [58,59,60]. Intraoperative endoscope video is the primary real-time data source for laparoscopic and endoscopic procedures and robot-assisted surgery [56,82]. Cone-beam CT employs a similar imaging strategy as CT and improves on some limitations of X-ray fluoroscopy, mainly the 2D nature of the data, by providing the capacity for a 3D snapshot of the intraoperative patient anatomy [84,85]. The final intraoperative data sources were from patient sensors and monitoring equipment [86] and simulated intraoperative data [73].
4.3. Processing
Table 3 lists the paper distribution based on the type of processing to prepare the preoperative or intraoperative data for display on the OST-HMD. The most frequent type of preprocessing of preoperative data was the creation of surface rendered models (shells).
Image Data Processing
After preoperative imaging, Digital Imaging and Communications in Medicine (DICOM) formatted data are typically provided which can be read in an open source library, such as 3D Slicer (https://www.slicer.org/, accessed on 23 March 2022) [46,65,74,87], or proprietary software, such as Mimics (https://www.materialise.com/, accessed on 23 March 2022) [47,61,88] or Brainlab (https://www.brainlab.com/digital-o-r/surgical-planning/, accessed on 23 March 2022) [67,84]. Surface rendered models provide enormous utility due to their ease of creation, lightweight model representation, and additional modifiable visualization properties, such as color, transparency, wireframe representations, and heatmaps [89]. For performance limited devices, such as current commercially available OST-HMDs, the number of vertices used to represent a 3D virtual model needs to be limited to ensure a performant application; many groups have mentioned the simplification of their model using open source tools, such as Blender (https://www.blender.org/, accessed on 23 March 2022) and MeshLab (https://www.meshlab.net/, accessed on 23 March 2022) [61].
Other 3D information that was included alongside the surface rendered models included relevant preoperative planning information, such as locations of pedicle screws [47], target anatomical contours in maxillofacial surgery [54,90], and tissue deformation models in liver resection surgery [61]. Several papers mentioned the streaming of raw 3D data directly to the OST-HMD for visualization, including intraoperative stereo endoscope video for robotic bedside task support [56], flexible endoscope steering [91], and endoluminal interventions [57]. Unlike 3D surface models, volume-rendered 3D models do not require manual segmentation and preprocessing to create and instead rely on discrete sampling of a 3D dataset. Volume rendering requires significant memory and computing power for loading and performant data display, which likely has limited the uptake into OST-HMD-led surgical navigation. Several groups reported the use of volume-rendered models for display on an OST-HMD during guidance for use in maxillofacial tumor resection [52] and neurosurgery [64]. Some groups mentioned the use of 3D printed models created from segmented surface models of preoperative patient anatomy for enhanced visualization and assessment alongside the virtual model display [51].
Not all virtually augmented content needs to be inherently 3D for it to provide value during surgical navigation. Several groups reported the use of 2D information in the form of telestrations for telementoring in general surgical task training [58] or teleproctoring for assistance during neurovascular procedures [59]. Other uses of 2D data included the display of raw 2D ultrasound data for general intraprocedural guidance [83,92] and assistance during cervical pedicle screw placement [93].
4.4. Overlay
In Table 4, each paper is categorized based on the method of achieving virtual content overlay, using either an external tracker, the OST-HMD camera (RGB or infrared), or manual placement. Further, we include the tracking marker used to achieve this overlay: external markers, such as retroreflective spheres, electromagnetic instruments or typical visible markers; or optical markers, such as ArUco [31], Vuforia (https://developer.vuforia.com/, accessed on 23 March 2022), custom markers, retroreflective spheres, QR-codes, AprilTag [94], or a marker-less approach.
Tracking Strategies
The most frequently employed external tracking-led strategy involved the use of an infrared tracking sensor, particularly: the Northern Digital Inc., Polaris (https://www.ndigital.com/products/, accessed on 23 March 2022) and Optitrack (https://optitrack.com/, accessed on 23 March 2022) (Northern Digital Inc., Waterloo, ON, Canada), or Medtronic StealthStation (https://www.medtronic.com/ca-en/, accessed on 23 March 2022) (Medtronic, Minneapolis, MN, USA). The sensor was used to detect rigidly mounted retroreflective spheres on the OST-HMD and instruments. The infrared tracking sensor served to locate the OST-HMD and tracked tools relative to its frame of reference, enabling the precise overlay of virtual content, provided the user and tracked tools remain in direct and uninterrupted line-of-sight of the tracking sensor. Electromagnetic tracking is capable of removing the line-of-sight requirement by defining an electromagnetic field in which micro-sensors can be located; the most frequently used system was the Northern Digital Inc. Aurora (https://www.ndigital.com/products/, accessed on 23 March 2022). Electromagnetic tracking is accurate within a specified volume, however, it has difficulty maintaining precise tracking in the presence of metallic instruments or devices. An external stereo RGB camera sensor, the MicronTracker from ClaroNav (https://www.claronav.com/, accessed on 23 March 2022) (ClaroNav, Toronto, ON, Canada) was also explored as the primary tracking solution and requires the use of typical visible marker fiducials for tracking. External tracking using stereo RGB is subject to the same line-of-sight challenges as with infrared tracking. Overall, in the external tracking-led approach, the OST-HMD served as a display medium for existing surgical navigation suites or sensors [54,68,84,93,95], replacing the traditional 2D computer monitor as the primary method of visualization.
The most commonly reported OST-HMD-led tracking solution was surface tracking, involving the use of the RGB camera capabilities of the headset, and square marker fiducials, such as those used in the Vuforia [64,69,74,96] (PTC, Boston, MA, USA) or ArUco [31,46,77,91] libraries. There were several papers which reported the use of custom markers for surface-based tracking, though the performance did not significantly differ from ArUco or Vuforia tracking solutions [82,97]. In the surface-based tracking strategy, the square marker fiducials served to localize the patient and any tracked tools relative to the reference frame of the OST-HMD, allowing for the overlay of virtual content [33,46,88,91,92]. Other groups reported the use of retroreflective spheres and the infrared camera capabilities on the HoloLens 1, HoloLens 2, or custom devices for improved tracking accuracy and performance over monocular RGB led tracking [60,75,90,98]. Moving away from the reliance on constructed marker configurations, several papers reported the use of point-based marker-less tracking for virtual content overlay [48,50,76].
During OST-HMD-based tracking, the line-of-sight requirement still exists; however, the tracked surgical instruments and patient are more likely to remain in a similar view configuration from the point-of-view of the HMD, and the HMD only needs to localize the patient and tracked instrument reference frames. In the case of an external tracking system, the patient, tracked instruments, and surgeon wearing the HMD all need to remain in the field of view of the tracking sensor of the navigation system to maintain their relative reference frames. For OST-HMD-based overlay, the HoloLens 1 was the most frequently mentioned device, followed by the HoloLens 2 and Magic Leap 1. Several groups reported successful guidance based on the OST-HMD camera and surface registration with markers [46,47,74,86] and point registration based on feature matching [48,50,87,99]. The final overlay strategy discussed is manual placement of virtual content; in this case it was up to either the surgeon [72,81] or a secondary user [55,74] to ensure comfortable placement of virtual content. After placement, virtual content remained anchored in place based on the SLAM predictions included with the HMD.
4.5. View
In Table 5 the 57 papers included in this review are categorized by the view type employed for virtual content visualization. Categories include the type of interaction with virtual content, the display device used for visualization, and the perception location of virtually augmented elements.
4.5.1. Interaction Paradigms
The most frequently utilized interaction paradigm was a combination of voice and gesture-based interaction () followed by control using gestures only () or voice only (). A combination of voice and/or gesture based interaction was commonly used alongside the HoloLens 1 or HoloLens 2 OST-HMDs due to their out-of-the-box support for several gestures and ease of integration of new voice commands. The next most frequently utilized interaction paradigm included the use of a controller (), which was common to papers which included the use of the Magic Leap 1 headset due to its reliance on controller-based manipulation of virtual content. Finally, the use of a Bluetooth keyboard and user head pose to control virtually augmented content was also reported.
4.5.2. Display Devices
Figure 9 includes a visual representation of the frequency of display device use; the HoloLens 1 was the most popular headset in 2021 () and in the first quarter of 2022 (). The HoloLens 2 was the second most frequently used headset in 2021 () and in the first quarter of 2022 (). The next most frequently used headset in 2021 and 2022 was the Magic Leap 1 () and (), respectively. The ODG R-6, Epson Moverio BT-200, and other custom devices were less frequently reported.
4.5.3. Perception Location
Perception location defined the placement of virtually augmented elements for surgical guidance; we defined two categories: direct overlay and adjacent overlay. Direct overlay involved the superimposition of virtual content with real objects, requiring a registration process for precise placement (Figure 10a). Adjacent overlay involved the placement of virtual content next to a real object and, as such, did not require the same stringent registration process for content alignment (Figure 10b). The majority of the surveyed articles () focused on direct overlay of virtual content with objects or tissue in the surgical scene to assist with guidance tasks. The remaining articles () involving adjacent overlay of virtual content centered on tasks which would typically rely on a computer monitor for data display and aimed to improve access to the relevant data. Use-cases involving adjacent overlay included the display of stereo endoscope video for robotic bedside assistants [56] and fluoroscopic imaging data [81] in the field of view of the user but adjacent to the patient.
4.6. Validation
A crucial aspect when evaluating any surgical navigation system involves validation: the assessment of quantitative performance metrics, such as accuracy and speed, and human factor considerations, such as perception, attention shift, and risk of error. In this section, the validation experiments performed in the surveyed articles are covered, and the main challenges and limitations described by the current literature are highlighted. In Table 6, the validation strategies employed by the articles included in the review are assessed and categorized based on the evaluation strategy, the reported accuracy metrics, and human factors limitations discussed.
4.6.1. System Evaluation
The most common strategy for OST-HMD system evaluation included the use of an anthropomorphic phantom ()—a reasonable approach, given the early stage investigational nature of many OST-HMD-based navigation platforms. Phantom models were used for assessment of error in orthopedic screw insertion [46,76,93], K-Wire placement for arthroplasty [50,51], maxillofacial drilling [54,69], head and neck cancer navigation [75], and as a means of simulating targeted media delivery in cardiac regenerative medicine [33]. Phantom models are relatively inexpensive and provide an excellent and safe platform for the initial quantitative assessment of a guidance system.
After phantom models, the next most frequently reported evaluation target was patients (). Evaluation in patients primarily involved early feasibility assessments which included surgeon feedback and usability considerations, and typically the virtual information was not used to inform treatment decisions [46,62,63,72,96]. Several papers investigated the quantitative accuracy of OST-HMD led navigation in preliminary patient studies, including assessment of orthopedic pedicle screw navigation [47], neuronavigation [65], maxillofacial osteotomy tracing [90], and maxillofacial tumor resection [52].
Cadaver models were the next most commonly utilized evaluation target (), followed by animal models (). As an evaluation platform, cadaver models are a step up from anthropomorphic phantoms in terms of anatomical realism; however, they do not require the same safety critical considerations as studies with patients. Cadaver models were used in the evaluation of navigation accuracy in complex pelvic osteotomies [45], assessment of performance during immersive telementoring [58], total shoulder arthroplasty [88], maxillofacial zygomatic arch reconstruction [85], and orthopedic K-Wire placement [50]. Animal models improve on the anatomical relevance of cadaver models due to the incorporation of realistic tissue deformation and real-time respiratory and cardiac motion. Animal models were investigated for OST-HMD-led percutaneous tumor puncture [68], placement of radioactive seeds during brachytherapy [98], and media delivery in targeted cardiac therapies [33].
4.6.2. System Accuracy
We have also indicated the measured accuracy of the surveyed papers in Table 6. Overall, the accuracy provided by an OST-HMD guidance system which is integrated with an existing surgical navigation suite has been demonstrated to be on the order of 2–5 mm [67,68,82,93,98,102], which is sufficient for certain surgical interventions, such as neurosurgical burr hole placement (<10 mm) [104] or complex pelvic osteotomies (<10 mm) [45]. As previously mentioned, the most popular tracking strategy for OST-HMD-camera-led surgical navigation relied on square-marker fiducials, such as ArUco [31] or Vuforia and monocular RGB video. However, the inherent assumption of planar surfaces introduced by the surface-based tracking strategy limited the precision for virtual content alignment on contoured surfaces, resulting in a tracking accuracy on the order of 5–8 mm [46,61,64,65,74]. Another source of error is the requirement for precise user-led placement of these square markers to permit accurate tracking. By leveraging the infrared cameras on the HoloLens 2 for stereo tracking, accuracy on the order of 2 mm was achieved in a phantom study [60]. Further, the introduction of an externally mounted red-green-blue-depth (RGBD) camera to the HoloLens 1 resulted in improved depth-based tracking with an accuracy of 4 mm as assessed by a phantom evaluation [77].
4.6.3. Human Factors, System Usability, and Technical Challenges
The final aspect of system validation which was documented in the articles was related to human factors and workflow benefits and limitations (Table 6). Human factors considerations have been consistently reported as one of the key challenges limiting the uptake of OST-HMD-based surgical navigation into the clinic [6]. In our assessment of OST-HMD-based surgical navigation systems, we categorized each reported human factors consideration as being: (1) addressed; (2) partially addressed; or (3) remaining to be addressed (persistent). As suggested by a recent FDA forum on the application of human factors and usability engineering to medical devices [105], we further categorized each individual human factors consideration into three general phases of user interaction including: (1) information perception; (2) cognitive processing; or (3) control actions. A chart summarizing the reported human factors considerations and status is included in Figure 11.
The most frequently reported persistent human factors consideration in the literature review was perception (). In the context of OST-HMD use in surgery, perception refers to the quantitative assessment of a user’s interpretation and understanding of virtually augmented content. Challenges in perception of virtually augmented elements can be attributed to a number of factors, including incorrect IPD estimation [40], incorrect or unaccounted for per-user display calibration [33,97], display limitations due to vergence-accommodation [10], misregistration of virtual content due to failed registration [106], and limitations of depth understanding of virtually augmented content [107]. Perceptual limitations contributed to additional errors in the stability of calibration during ultrasound image-guided robot cervical pedicle screw placement [93], with navigation during total shoulder arthroscopy [99], and with marker-less tracking for guidance in head and neck carcinoma imaging [75].
Following perception, the next most commonly discussed human factors components were mental mapping (), spatial awareness (), and attention shift (). In the survey, OST-HMDs were discussed as contributing to the improvement of spatial awareness and mental mapping, as well as the reduction in attention shift during surgical navigation and served to address or partially address these considerations. Spatial awareness refers to the fundamental limitation of conventional image guidance methods in their display of inherently 3D content for consumption on a 2D medium. Research into spatial awareness has indicated that 3D models of patient anatomy enable improved understanding of spatial relationships over 2D imaging slice planes [108,109]. Mental mapping is closely associated with spatial awareness and refers to the requirement for a surgeon to project (or mentally map) 2D image data onto the 3D scene in order to leverage this information for surgical guidance. A reliance on mental projection of data for surgical guidance can introduce errors to the surgery and additional mental workload on the surgeon [6,33]. Attention shift describes the requirement for a surgeon to frequently gaze between the provided navigation information on an external display and the patient; with an OST-HMD, virtual guidance information can be brought directly into the FOV of the wearer to remove this requirement. Improved spatial awareness and mental mapping as compared with traditional guidance paradigms was reported by numerous articles across different surgical applications [33,46,55,75,97]. Reduced attention shift by using an OST-HMD for the display of guidance information was measured in fluoroscopic imaging for orthopedic surgery [81] and ultrasound imaging for ultrasound-guided procedures [92].
Ergonomics () was a commonly discussed human factor consideration which was partially addressed with the use of OST-HMD led navigation. Ergonomics included physical factors, such as the effect of user posture and perceived comfort, as well as physiological factors, such as nausea and eye strain during OST-HMD use. With OST-HMD use, it is possible to position virtually augmented content in a comfortable location based on user preference. Despite the additional weight and bulk of wearing an HMD throughout a procedure, ergonomic benefits were reported in OST-HMD use for data display during robotic surgery bedside assistant tasks [56] and in live fluoroscopic imaging display during orthopedic interventions [81]. However, the contribution of OST-HMD use to ergonomics was not all positive; challenges with optical display quality and latency can contribute to nausea and eye strain [110].
Risk of error (), ease of use (), context (), and interaction challenges () were the next most frequently discussed persistent human factor limitations. Risk of error described the concerns of potential mistakes as a result of virtual guidance. Ease of use, context and interaction collectively describe the required inputs from a user to manually adapt the current virtually augmented guidance information to be optimal for their current surgical task. Several articles discussed concerns regarding the introduction of error by relying upon virtual guidance information presented by an OST-HMD that is no longer relevant to the current anatomical scene due to loss of tracking [76] or accidental user error [61]. An additional challenge with OST-HMD led surgical guidance is the lack of shared situational awareness for the care team and staff, meaning it is solely up to the primary surgeon or user to determine the validity of aligned virtual content. Any surgical intervention can be broken down into a series of steps or phases which comprise the duration of the procedure. These phases will vary between different procedures, and during each phase there will often be different data or relevant information which are used to inform clinical decision-making. During an OST-HMD led surgical navigation procedure, if the surgeon (or a bystander) is required to manually adapt or manipulate the presented virtual content to be relevant to their current surgical context it can introduce additional ease of use and interaction challenges. Several articles mentioned workflow challenges due to the manual interaction with virtual models required to adapt the information to the current surgical task [33,69,78,83]. These workflow challenges contributed to reduced enjoyment and overall usability of the guidance system [58,86].
Occlusion (), a persistent technical challenge, contributed to limitations in virtual model alignment and loss of tracking during OST-HMD based surgical navigation. With traditional navigation approaches based on an RGB or infrared camera and visible markers or retroreflective spheres, the loss of direct line-of-sight of the markers will result in loss of tracking. This is problematic as the line-of-sight requirement can be frequently interrupted over the course of an intervention due to crowding in the operating room and other surgical complications, such as blood and smoke [33,75]. By leveraging the stereo infrared cameras on the HoloLens 2 and an extended Kalman filter for pose prediction smoothing, it was demonstrated that the contribution of occlusion to loss of tracking could be reduced [60]. Further, with marker-less approaches there lies the potential to remove the requirement of the complex setup and calibration involved in traditional marker-based navigation strategies [76,99].
4.7. Recommendations for Future Work
Although there have been significant efforts to improve the design of OST-HMD led surgical navigation platforms, applications have remained constrained to research lab environments and there has been little clinical uptake [5,6]. As evidenced by the broad survey of recent literature, the poor clinical uptake of OST-HMDs for surgical guidance can be partially attributed to a lack of HMD performance [7], rendering resolution [8], and application or task-specific HMD design [21]; however, perceptual challenges [9,10,33], surgical context and interaction limitations [11,12], and registration and occlusion challenges [13,14] remain the key hurdles in the widespread clinical adoption of these technologies. To this end, we suggest several directions for future work which stand as meaningful initial steps in the mitigation of these limitations and in the improvement in design for more effective OST-HMD led surgical navigation platforms.
4.7.1. Marker-Less Tracking for Surgical Guidance
To address a frequently mentioned limitation of current marker-based tracking solutions—occlusion and the requirement for complex setup and potential user-introduced error during marker placement—we suggest the exploration of marker-less tracking strategies for leading surgical navigation. In the context of general computer vision and AR, marker-free object pose estimation remains a challenging and unsolved problem [111]; prior strategies have utilized conventional and deep learning-based techniques [111]. Related to the surgical domain, recent work has focused on leveraging constraints imposed by typical hand-object interactions for the prediction of precise hand and rigid surgical drill pose from monocular RGB data [112] and has indicated the feasibility of marker-less surgical tracking on a commercially available OST-HMD using a data streaming approach [113].
4.7.2. Context-Relevant Augmented Reality for Intelligent Guidance
Ease of use, context, and interaction challenges were repeatedly cited as limitations of current OST-HMD guidance systems and contributors to workflow and usability challenges. The requirement for a user to manually adapt the virtual information to be relevant to their current surgical context and preference can result in significant interruptions to the overall surgical workflow. These interruptions can be exacerbated by additional challenges with virtual content interaction introduced with current commercially available OST-HMDs, requiring users to perform gestures, say voice commands, or interact with virtual menus [11]. Understanding the current surgical context involves the interpretation of the vast amount of information created during a surgical procedure, which has been explored using traditional or deep learning-based [114] strategies. Recent work has explored the feasibility of OST-HMD-based guidance systems for context-relevant information display based on an interpretation of the current surgical task of the wearer of the HMD using specialized sensors [12] or monocular RGB video [115] as input.
5. Conclusions
In this systematic review, we discussed recent applications of OST-HMDs in AR-led surgical navigation and identified several key challenges which continue to limit clinical uptake. The most commonly reported surgical target involved orthopedic applications, likely due to the rigid nature of anatomy and availability of consistent landmarks for registration and tracking. As for input data for visualization, CT was the most common form of preoperative imaging, with fluoroscopy the most utilized form of intraoperative imaging. Preoperative CT and intraoperative fluoroscopy are commonly used in combination for leading orthopedic interventions. For visualization of imaging-derived virtual models, the most common strategy involved the display of surface rendered models or other planning information. The popularity of surface rendered models can be attributed to their ease of creation, modifiable visualization properties, and rendering performance on commercially available OST-HMDs.
The most popular overlay strategy for virtual content display involved the use of the HoloLens 1 or HoloLens 2 OST-HMDs with RGB based tracking based on ArUco or Vuforia markers. Second to this was the reliance of manual placement of virtual elements by the surgeon, followed by the incorporation of co-calibrated external tracking systems such as the Northern Digital Inc., Polaris. For interaction, a combination of voice and gesture-based or gesture-based only were the most frequently reported paradigms due to their out-of-the-box support on the HoloLens 1 and 2 devices. As for the perception location of virtual content, direct overlay of virtual content onto a target object was the most commonly pursued type of visualization.
Due to the early investigational nature of many OST-HMD based navigation platforms, an anthropomorphic phantom was used in the majority of validation studies. When integrated with an existing surgical navigation suite, accuracy on the order of 2–5 mm is feasible with an OST-HMD—a result that is sufficient for certain surgical interventions. As a stand-alone system, OST-HMDs are currently capable of accuracy on the order of 5–8 mm using marker-based tracking and monocular RGB video. In our evaluation, OST-HMD use in surgery fully or partially addressed several human factors including: mental mapping capacity, spatial awareness, attention shift, and ergonomics. However, we also identified several human factors and technical challenges commonly mentioned during OST-HMD use in surgery which continue to persist, including: perception, ease of use, context, interaction challenges, and occlusion.
Coinciding with the significant investments from leading technology companies into the metaverse and the XR technologies enabling associated shared virtual experiences, there has been increased interest in incorporating these transformational technologies, such as OST-HMDs, for improving many aspects of surgery. It is anticipated that the hardware and display limitations present in current generation OST-HMDs will be improved upon with future iterations. With additional contributions to reduce the impact of the remaining technical and human factors limitations, we believe that clinically viable OST-HMD-led surgical navigation is feasible.
Author Contributions
Conceptualization, M.D. and G.A.W.; Funding acquisition, N.R.G.; Methodology, M.D.; Project administration, N.R.G. and G.A.W.; Resources, N.R.G. and G.A.W.; Supervision, N.R.G. and G.A.W.; Writing—original draft, M.D.; Writing—review and editing, M.D., N.R.G. and G.A.W. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Natural Sciences and Engineering Research Council of Canada (NSERC) Discovery program (RGPIN-2019-06367) and New Frontiers in Research Fund-Exploration (NFRFE-2019-00333). N.R.G. is supported by the National New Investigator (NNI) award from the Heart and Stroke Foundation of Canada (HSFC).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Additional literature search data are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kishino, F.; Milgram, P. A Taxonomy of Mixed Reality Visual Displays. Ieice Trans. Inf. Syst. 1994, 77, 1321–1329. [Google Scholar]
- Kelly, P.J.; Alker, G.J.; Goerss, S. Computer-assisted stereotactic microsurgery for the treatment of intracranial neoplasms. Neurosurgery 1982, 10, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Peters, T.M.; Linte, C.A.; Yaniv, Z.; Williams, J. Mixed and Augmented Reality in Medicine; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Cleary, K.; Peters, T.M. Image-guided interventions: Technology review and clinical applications. Annu. Rev. Biomed. Eng. 2010, 12, 119–142. [Google Scholar] [CrossRef] [PubMed]
- Eckert, M.; Volmerg, J.S.; Friedrich, C.M. Augmented reality in medicine: Systematic and bibliographic review. JMIR mHealth uHealth 2019, 7, e10967. [Google Scholar] [CrossRef] [PubMed]
- Birlo, M.; Edwards, P.J.E.; Clarkson, M.; Stoyanov, D. Utility of Optical See-Through Head Mounted Displays in Augmented Reality-Assisted Surgery: A systematic review. Med. Image Anal. 2022, 77, 102361. [Google Scholar] [CrossRef]
- Bernhardt, S.; Nicolau, S.A.; Soler, L.; Doignon, C. The status of augmented reality in laparoscopic surgery as of 2016. Med. Image Anal. 2017, 37, 66–90. [Google Scholar] [CrossRef]
- Sielhorst, T.; Feuerstein, M.; Navab, N. Advanced medical displays: A literature review of augmented reality. J. Disp. Technol. 2008, 4, 451–467. [Google Scholar] [CrossRef] [Green Version]
- Kramida, G. Resolving the Vergence-Accommodation Conflict in Head-Mounted Displays. IEEE Trans. Vis. Comput. Graph. 2015, 22, 1912–1931. [Google Scholar] [CrossRef]
- Condino, S.; Carbone, M.; Piazza, R.; Ferrari, M.; Ferrari, V. Perceptual Limits of Optical See-Through Visors for Augmented Reality Guidance of Manual Tasks. IEEE Trans. Biomed. Eng. 2020, 67, 411–419. [Google Scholar] [CrossRef]
- Navab, N.; Traub, J.; Sielhorst, T.; Feuerstein, M.; Bichlmeier, C. Action-and workflow-driven augmented reality for computer-aided medical procedures. IEEE Comput. Graph. Appl. 2007, 27, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Katić, D.; Spengler, P.; Bodenstedt, S.; Castrillon-Oberndorfer, G.; Seeberger, R.; Hoffmann, J.; Dillmann, R.; Speidel, S. A system for context-aware intraoperative augmented reality in dental implant surgery. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.; Azimi, E.; Kazanzides, P.; Navab, N. Comprehensive Tracker Based Display Calibration for Holographic Optical See-Through Head-Mounted Display. arXiv 2017, arXiv:1703.05834. [Google Scholar]
- Qian, L.; Song, T.; Unberath, M.; Kazanzides, P. AR-Loupe: Magnified Augmented Reality by Combining an Optical See-Through Head-Mounted Display and a Loupe. IEEE Trans. Vis. Comput. Graph. 2011, 28, 2550–2562. [Google Scholar] [CrossRef] [PubMed]
- Van Krevelen, D.; Poelman, R. A survey of augmented reality technologies, applications and limitations. Int. J. Virtual Real. 2010, 9, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Rolland, J.P.; Fuchs, H. Optical Versus Video See-Through Head-Mounted Displays in Medical Visualization. Presence 2000, 9, 287–309. [Google Scholar] [CrossRef]
- Gervautz, M.; Schmalstieg, D. Anywhere Interfaces Using Handheld Augmented Reality. Computer 2012, 45, 26–31. [Google Scholar] [CrossRef]
- Bimber, O.; Raskar, R. Spatial Augmented Reality: Merging Real and Virtual Worlds; Peters, A.K., Ed.; CRC Press: Boca Raton, FL, USA, 2005. [Google Scholar]
- Hong, J.; Kim, Y.; Choi, H.J.; Hahn, J.; Park, J.H.; Kim, H.; Min, S.W.; Chen, N.; Lee, B. Three-dimensional display technologies of recent interest: Principles, status, and issues [Invited]. Appl. Opt. 2011, 50, H87–H115. [Google Scholar] [CrossRef] [Green Version]
- Cutolo, F.; Fontana, U.; Ferrari, V. Perspective preserving solution for quasi-orthoscopic video see-through HMDs. Technologies 2018, 6, 9. [Google Scholar] [CrossRef] [Green Version]
- Cattari, N.; Cutolo, F.; D’amato, R.; Fontana, U.; Ferrari, V. Toed-in vs parallel displays in video see-through head-mounted displays for close-up view. IEEE Access 2019, 7, 159698–159711. [Google Scholar] [CrossRef]
- Grubert, J.; Itoh, Y.; Moser, K.; Swan, J.E. A survey of calibration methods for optical see-through head-mounted displays. IEEE Trans. Vis. Comput. Graph. 2017, 24, 2649–2662. [Google Scholar] [CrossRef] [Green Version]
- Rolland, J.P.; Gibson, W.; Ariely, D. Towards Quantifying Depth and Size Perception in Virtual Environments. Presence Teleoperators Virtual Environ. 1995, 4, 24–49. [Google Scholar] [CrossRef]
- Cakmakci, O.; Rolland, J. Head-Worn Displays: A Review. J. Disp. Technol. 2006, 2, 199–216. [Google Scholar] [CrossRef]
- Guo, N.; Wang, T.; Yang, B.; Hu, L.; Liu, H.; Wang, Y. An online calibration method for microsoft HoloLens. IEEE Access 2019, 7, 101795–101803. [Google Scholar] [CrossRef]
- Sutherland, I.E. A head-mounted three dimensional display. In Proceedings of the 9–11 December 1968, Fall Joint Computer Conference, Part I, San Francisco, CA, USA, 9–11 December 1968; pp. 757–764. [Google Scholar]
- Bention, S. Selected PapersonThree-Dimensional Displays; SPEOptical Engineeting Press: Belingham, WA, USA, 2001; Volume 4, pp. 446–458. [Google Scholar]
- Holliman, N.S.; Dodgson, N.A.; Favalora, G.E.; Pockett, L. Three-Dimensional Displays: A Review and Applications Analysis. IEEE Trans. Broadcast. 2011, 57, 362–371. [Google Scholar] [CrossRef]
- Szeliski, R. Computer Vision: Algorithms and Applications; Springer Science & Business Media: Berlin, Germany, 2010. [Google Scholar]
- Zhang, Z. A flexible new technique for camera calibration. IEEE Trans. Pattern Anal. Mach. Intell. 2000, 22, 1330–1334. [Google Scholar] [CrossRef] [Green Version]
- Garrido-Jurado, S.; Muñoz-Salinas, R.; Madrid-Cuevas, F.; Marín-Jiménez, M. Automatic generation and detection of highly reliable fiducial markers under occlusion. Pattern Recognit. 2014, 47, 2280–2292. [Google Scholar] [CrossRef]
- Prince, S.J. Computer Vision: Models, Learning, and Inference; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Doughty, M.; Ghugre, N.R. Head-Mounted Display-Based Augmented Reality for Image-Guided Media Delivery to the Heart: A Preliminary Investigation of Perceptual Accuracy. J. Imaging 2022, 8, 33. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Review of the augmented reality systems for shoulder rehabilitation. Information 2019, 10, 154. [Google Scholar] [CrossRef] [Green Version]
- Singh, G.; Ellis, S.R.; Swan, J.E. The Effect of Focal Distance, Age, and Brightness on Near-Field Augmented Reality Depth Matching. IEEE Trans. Vis. Comput. Graph. 2020, 26, 1385–1398. [Google Scholar] [CrossRef] [Green Version]
- Hua, H. Enabling Focus Cues in Head-Mounted Displays. Proc. IEEE 2017, 105, 805–824. [Google Scholar] [CrossRef]
- Koulieris, G.A.; Bui, B.; Banks, M.S.; Drettakis, G. Accommodation and comfort in head-mounted displays. ACM Trans. Graph. 2017, 36, 1–11. [Google Scholar] [CrossRef]
- Cutting, J.E.; Vishton, P.M. Chapter 3—Perceiving Layout and Knowing Distances: The Integration, Relative Potency, and Contextual Use of Different Information about Depth. In Perception of Space and Motion; Epstein, W., Rogers, S., Eds.; Handbook of Perception and Cognition; Academic Press: Cambridge, MA, USA, 1995; pp. 69–117. [Google Scholar] [CrossRef]
- Teittinen, M. Depth Cues in the Human Visual System. The Encyclopedia of Virtual Environments. 1993, Volume 1. Available online: http://www.hitl.washington.edu/projects/knowledge_base/virtual-worlds/EVE/III.A.1.c.DepthCues.html (accessed on 23 March 2022).
- Lee, S.; Hua, H. Effects of Configuration of Optical Combiner on Near-Field Depth Perception in Optical See-Through Head-Mounted Displays. IEEE Trans. Vis. Comput. Graph. 2016, 22, 1432–1441. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.D.; Earl, R. Human Factors of Stereoscopic 3D Displays; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Kress, B.C.; Cummings, W.J. 11-1: Invited Paper: Towards the Ultimate Mixed Reality Experience: HoloLens Display Architecture Choices. SID Symp. Dig. Tech. Pap. 2017, 48, 127–131. [Google Scholar] [CrossRef]
- Ungureanu, D.; Bogo, F.; Galliani, S.; Sama, P.; Duan, X.; Meekhof, C.; Stühmer, J.; Cashman, T.J.; Tekin, B.; Schönberger, J.L.; et al. HoloLens 2 Research Mode as a Tool for Computer Vision Research. arXiv 2020, arXiv:2008.11239. [Google Scholar]
- Kersten-Oertel, M.; Jannin, P.; Collins, D.L. DVV: A Taxonomy for Mixed Reality Visualization in Image Guided Surgery. IEEE Trans. Vis. Comput. Graph. 2012, 18, 332–352. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, J.; Liebmann, F.; Hoch, A.; Snedeker, J.G.; Farshad, M.; Rahm, S.; Zingg, P.O.; Fürnstahl, P. Augmented Reality Based Surgical Navigation of Complex Pelvic Osteotomies—A Feasibility Study on Cadavers. Appl. Sci. 2021, 11, 1228. [Google Scholar] [CrossRef]
- Dennler, C.; Bauer, D.E.; Scheibler, A.G.; Spirig, J.; Götschi, T.; Fürnstahl, P.; Farshad, M. Augmented reality in the operating room: A clinical feasibility study. BMC Musculoskelet. Disord. 2021, 22, 451. [Google Scholar] [CrossRef]
- Farshad, M.; Fürnstahl, P.; Spirig, J.M. First in man in-situ augmented reality pedicle screw navigation. N. Am. Spine Soc. J. (NASSJ) 2021, 6, 100065. [Google Scholar] [CrossRef]
- Gu, W.; Shah, K.; Knopf, J.; Navab, N.; Unberath, M. Feasibility of image-based augmented reality guidance of total shoulder arthroplasty using microsoft HoloLens 1. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2021, 9, 261–270. [Google Scholar] [CrossRef]
- Teatini, A.; Kumar, R.P.; Elle, O.J.; Wiig, O. Mixed reality as a novel tool for diagnostic and surgical navigation in orthopaedics. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 407–414. [Google Scholar] [CrossRef]
- Spirig, J.M.; Roner, S.; Liebmann, F.; Fürnstahl, P.; Farshad, M. Augmented reality-navigated pedicle screw placement: A cadaveric pilot study. Eur. Spine J. 2021, 30, 3731–3737. [Google Scholar] [CrossRef] [PubMed]
- Schlueter-Brust, K.; Henckel, J.; Katinakis, F.; Buken, C.; Opt-Eynde, J.; Pofahl, T.; Rodriguez y Baena, F.; Tatti, F. Augmented-Reality-Assisted K-Wire Placement for Glenoid Component Positioning in Reversed Shoulder Arthroplasty: A Proof-of-Concept Study. J. Pers. Med. 2021, 11, 777. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.N.; Hu, L.H.; Soh, H.Y.; Yu, Y.; Zhang, W.B.; Peng, X. Accuracy of Mixed Reality Combined With Surgical Navigation Assisted Oral and Maxillofacial Tumor Resection. Front. Oncol. 2021, 11, 715484. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Li, C.; Tu, P.; Ahmed, A.; Ji, T.; Chen, X. Development and Application of Digital Maxillofacial Surgery System Based on Mixed Reality Technology. Front. Surg. 2022, 8, 719985. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Liu, K.; Lin, L.; Wang, X.; Xie, L. Use of augmented reality navigation to optimise the surgical management of craniofacial fibrous dysplasia. Br. J. Oral Maxillofac. Surg. 2022, 60, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, H.; Tatti, F.; y Baena, F.R. Augmented reality in robotic assisted orthopaedic surgery: A pilot study. J. Biomed. Informat. 2021, 120, 103841. [Google Scholar] [CrossRef]
- Stewart, C.L.; Fong, A.; Payyavula, G.; DiMaio, S.; Lafaro, K.; Tallmon, K.; Wren, S.; Sorger, J.; Fong, Y. Study on augmented reality for robotic surgery bedside assistants. J. Robot. Surg. 2021, 1–8. [Google Scholar] [CrossRef]
- Lin, Z.; Gao, A.; Ai, X.; Gao, H.; Fu, Y.; Chen, W.; Yang, G.Z. ARei: Augmented-Reality-Assisted Touchless Teleoperated Robot for Endoluminal Intervention. IEEE/ASME Trans. Mechatronics 2021, 1–11. [Google Scholar] [CrossRef]
- Gasques, D.; Johnson, J.G.; Sharkey, T.; Feng, Y.; Wang, R.; Xu, Z.R.; Zavala, E.; Zhang, Y.; Xie, W.; Zhang, X.; et al. ARTEMIS: A Collaborative Mixed-Reality System for Immersive Surgical Telementoring. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems. Association for Computing Machinery, CHI ’21, Yokohama, Japan, 8–13 May 2021; pp. 1–14. [Google Scholar] [CrossRef]
- Rai, A.T.; Deib, G.; Smith, D.; Boo, S. Teleproctoring for Neurovascular Procedures: Demonstration of Concept Using Optical See-Through Head-Mounted Display, Interactive Mixed Reality, and Virtual Space Sharing—A Critical Need Highlighted by the COVID-19 Pandemic. Am. J. Neuroradiol. 2021, 42, 1109–1115. [Google Scholar] [CrossRef]
- Gsaxner, C.; Li, J.; Pepe, A.; Schmalstieg, D.; Egger, J. Inside-Out Instrument Tracking for Surgical Navigation in Augmented Reality. In Proceedings of the 27th ACM Symposium on Virtual Reality Software and Technology. Association for Computing Machinery, VRST ’21, Osaka, Japan, 8–10 December 2021; pp. 1–11. [Google Scholar] [CrossRef]
- Zhang, F.; Zhang, S.; Sun, L.; Zhan, W.; Sun, L. Research on registration and navigation technology of augmented reality for ex-vivo hepatectomy. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 147–155. [Google Scholar] [CrossRef]
- Ivan, M.E.; Eichberg, D.G.; Di, L.; Shah, A.H.; Luther, E.M.; Lu, V.M.; Komotar, R.J.; Urakov, T.M. Augmented reality head-mounted display–based incision planning in cranial neurosurgery: A prospective pilot study. Neurosurg. Focus 2021, 51, E3. [Google Scholar] [CrossRef] [PubMed]
- Fick, T.; van Doormaal, J.; Hoving, E.; Regli, L.; van Doormaal, T. Holographic patient tracking after bed movement for augmented reality neuronavigation using a head-mounted display. Acta Neurochir. 2021, 163, 879–884. [Google Scholar] [CrossRef]
- Kunz, C.; Hlaváč, M.; Schneider, M.; Pala, A.; Henrich, P.; Jickeli, B.; Wörn, H.; Hein, B.; Wirtz, R.; Mathis-Ullrich, F. Autonomous Planning and Intraoperative Augmented Reality Navigation for Neurosurgery. IEEE Trans. Med. Robot. Bionics 2021, 3, 738–749. [Google Scholar] [CrossRef]
- Qi, Z.; Li, Y.; Xu, X.; Zhang, J.; Li, F.; Gan, Z.; Xiong, R.; Wang, Q.; Zhang, S.; Chen, X. Holographic mixed-reality neuronavigation with a head-mounted device: Technical feasibility and clinical application. Neurosurg. Focus 2021, 51, E22. [Google Scholar] [CrossRef] [PubMed]
- Condino, S.; Montemurro, N.; Cattari, N.; D’Amato, R.; Thomale, U.; Ferrari, V.; Cutolo, F. Evaluation of a Wearable AR Platform for Guiding Complex Craniotomies in Neurosurgery. Ann. Biomed. Eng. 2021, 49, 2590–2605. [Google Scholar] [CrossRef] [PubMed]
- Uhl, C.; Hatzl, J.; Meisenbacher, K.; Zimmer, L.; Hartmann, N.; Böckler, D. Mixed-Reality-Assisted Puncture of the Common Femoral Artery in a Phantom Model. J. Imaging 2022, 8, 47. [Google Scholar] [CrossRef]
- Li, R.; Tong, Y.; Yang, T.; Guo, J.; Si, W.; Zhang, Y.; Klein, R.; Heng, P.A. Towards quantitative and intuitive percutaneous tumor puncture via augmented virtual reality. Comput. Med. Imaging Graph. 2021, 90, 101905. [Google Scholar] [CrossRef]
- Liu, Y.; Azimi, E.; Davé, N.; Qiu, C.; Yang, R.; Kazanzides, P. Augmented Reality Assisted Orbital Floor Reconstruction. In Proceedings of the 2021 IEEE International Conference on Intelligent Reality (ICIR), Piscataway, NJ, USA, 12–13 May 2021; pp. 25–30. [Google Scholar] [CrossRef]
- Tarutani, K.; Takaki, H.; Igeta, M.; Fujiwara, M.; Okamura, A.; Horio, F.; Toudou, Y.; Nakajima, S.; Kagawa, K.; Tanooka, M.; et al. Development and Accuracy Evaluation of Augmented Reality-based Patient Positioning System in Radiotherapy: A Phantom Study. In Vivo 2021, 35, 2081–2087. [Google Scholar] [CrossRef]
- Johnson, P.B.; Jackson, A.; Saki, M.; Feldman, E.; Bradley, J. Patient posture correction and alignment using mixed reality visualization and the HoloLens 2. Med. Phys. 2022, 49, 15–22. [Google Scholar] [CrossRef]
- Kitagawa, M.; Sugimoto, M.; Haruta, H.; Umezawa, A.; Kurokawa, Y. Intraoperative holography navigation using a mixed-reality wearable computer during laparoscopic cholecystectomy. Surgery 2021, 171, 1006–1013. [Google Scholar] [CrossRef]
- Heinrich, F.; Huettl, F.; Schmidt, G.; Paschold, M.; Kneist, W.; Huber, T.; Hansen, C. HoloPointer: A virtual augmented reality pointer for laparoscopic surgery training. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, V.M.; Krivtsov, A.M.; Strelkov, S.V.; Kalakutskiy, N.V.; Yaremenko, A.I.; Petropavlovskaya, M.Y.; Portnova, M.N.; Lukina, O.V.; Litvinov, A.P. Intraoperative Use of Mixed Reality Technology in Median Neck and Branchial Cyst Excision. Future Internet 2021, 13, 214. [Google Scholar] [CrossRef]
- Gsaxner, C.; Pepe, A.; Li, J.; Ibrahimpasic, U.; Wallner, J.; Schmalstieg, D.; Egger, J. Augmented Reality for Head and Neck Carcinoma Imaging: Description and Feasibility of an Instant Calibration, Markerless Approach. Comput. Methods Programs Biomed. 2021, 200, 105854. [Google Scholar] [CrossRef]
- von Atzigen, M.; Liebmann, F.; Hoch, A.; Miguel Spirig, J.; Farshad, M.; Snedeker, J.; Fürnstahl, P. Marker-free surgical navigation of rod bending using a stereo neural network and augmented reality in spinal fusion. Med. Image Anal. 2022, 77, 102365. [Google Scholar] [CrossRef]
- Hu, X.; Baena, F.R.y.; Cutolo, F. Head-Mounted Augmented Reality Platform for Markerless Orthopaedic Navigation. IEEE J. Biomed. Health Informat. 2022, 26, 910–921. [Google Scholar] [CrossRef]
- Velazco-Garcia, J.D.; Navkar, N.V.; Balakrishnan, S.; Younes, G.; Abi-Nahed, J.; Al-Rumaihi, K.; Darweesh, A.; Elakkad, M.S.M.; Al-Ansari, A.; Christoforou, E.G.; et al. Evaluation of how users interface with holographic augmented reality surgical scenes: Interactive planning MR-Guided prostate biopsies. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, e2290. [Google Scholar] [CrossRef]
- Nousiainen, K.; Mäkelä, T. Measuring geometric accuracy in magnetic resonance imaging with 3D-printed phantom and nonrigid image registration. Magn. Reson. Mater. Phys. Biol. Med. 2020, 33, 401–410. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Ha, J.; Yoon, S.; Tae Sohn, Y.; Seo, J.; Chul Koh, J.; Lee, D. Augmented Reality Assisted Surgical Navigation System for Epidural Needle Intervention. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine Biology Society (EMBC), Mexico City, Mexico, 1–5 November 2021; pp. 4705–4708, ISSN 2694-0604. [Google Scholar] [CrossRef]
- Johnson, A.A.; Reidler, J.S.; Speier, W.; Fuerst, B.; Wang, J.; Osgood, G.M. Visualization of Fluoroscopic Imaging in Orthopedic Surgery: Head-Mounted Display vs Conventional Monitor. Surg. Innov. 2021, 29, 353–359. [Google Scholar] [CrossRef]
- Tu, P.; Gao, Y.; Lungu, A.J.; Li, D.; Wang, H.; Chen, X. Augmented reality based navigation for distal interlocking of intramedullary nails utilizing Microsoft HoloLens 2. Comput. Biol. Med. 2021, 133, 104402. [Google Scholar] [CrossRef]
- Cattari, N.; Condino, S.; Cutolo, F.; Ferrari, M.; Ferrari, V. In Situ Visualization for 3D Ultrasound-Guided Interventions with Augmented Reality Headset. Bioengineering 2021, 8, 131. [Google Scholar] [CrossRef]
- Frisk, H.; Lindqvist, E.; Persson, O.; Weinzierl, J.; Bruetzel, L.K.; Cewe, P.; Burström, G.; Edström, E.; Elmi-Terander, A. Feasibility and Accuracy of Thoracolumbar Pedicle Screw Placement Using an Augmented Reality Head Mounted Device. Sensors 2022, 22, 522. [Google Scholar] [CrossRef]
- Puladi, B.; Ooms, M.; Bellgardt, M.; Cesov, M.; Lipprandt, M.; Raith, S.; Peters, F.; Möhlhenrich, S.C.; Prescher, A.; Hölzle, F.; et al. Augmented Reality-Based Surgery on the Human Cadaver Using a New Generation of Optical Head-Mounted Displays: Development and Feasibility Study. JMIR Serious Games 2022, 10, e34781. [Google Scholar] [CrossRef]
- Kimmel, S.; Cobus, V.; Heuten, W. opticARe—Augmented Reality Mobile Patient Monitoring in Intensive Care Units. In Proceedings of the 27th ACM Symposium on Virtual Reality Software and Technology, Osaka, Japan, 8–10 December 2021; ACM: New York, NY, USA, 2021; pp. 1–11. [Google Scholar] [CrossRef]
- Lee, S.; Jung, H.; Lee, E.; Jung, Y.; Kim, S.T. A Preliminary Work: Mixed Reality-Integrated Computer-Aided Surgical Navigation System for Paranasal Sinus Surgery Using Microsoft HoloLens 2. In Computer Graphics International Conference; Magnenat-Thalmann, N., Interrante, V., Thalmann, D., Papagiannakis, G., Sheng, B., Kim, J., Gavrilova, M., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Manhattan, NYC, USA, 2021; pp. 633–641. [Google Scholar] [CrossRef]
- Kriechling, P.; Loucas, R.; Loucas, M.; Casari, F.; Fürnstahl, P.; Wieser, K. Augmented reality through head-mounted display for navigation of baseplate component placement in reverse total shoulder arthroplasty: A cadaveric study. Arch. Orthop. Trauma Surg. 2021, 1–7. [Google Scholar] [CrossRef]
- Fischer, M.; Leuze, C.; Perkins, S.; Rosenberg, J.; Daniel, B.; Martin-Gomez, A. Evaluation of Different Visualization Techniques for Perception-Based Alignment in Medical AR. In Proceedings of the 2020 IEEE International Symposium on Mixed and Augmented Reality Adjunct (ISMAR-Adjunct), Recife, Brazil, 9–13 November 2020; pp. 45–50. [Google Scholar] [CrossRef]
- Carbone, M.; Cutolo, F.; Condino, S.; Cercenelli, L.; D’Amato, R.; Badiali, G.; Ferrari, V. Architecture of a Hybrid Video/Optical See-through Head-Mounted Display-Based Augmented Reality Surgical Navigation Platform. Information 2022, 13, 81. [Google Scholar] [CrossRef]
- Ma, X.; Song, C.; Qian, L.; Liu, W.; Chiu, P.W.; Li, Z. Augmented Reality Assisted Autonomous View Adjustment of a 6-DOF Robotic Stereo Flexible Endoscope. IEEE Trans. Med. Robot. Bionics 2022, 4, 356–367. [Google Scholar] [CrossRef]
- Nguyen, T.; Plishker, W.; Matisoff, A.; Sharma, K.; Shekhar, R. HoloUS: Augmented reality visualization of live ultrasound images using HoloLens for ultrasound-guided procedures. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 385–391. [Google Scholar] [CrossRef]
- Tu, P.; Qin, C.; Guo, Y.; Li, D.; Lungu, A.J.; Wang, H.; Chen, X. Ultrasound image guided and mixed reality-based surgical system with real-time soft tissue deformation computing for robotic cervical pedicle screw placement. IEEE Trans. Biomed. Eng. 2022. [Google Scholar] [CrossRef]
- Olson, E. AprilTag: A robust and flexible visual fiducial system. In Proceedings of the 2011 IEEE International Conference on Robotics and Automation, Shanghai, China, 9–13 May 2011; pp. 3400–3407. [Google Scholar]
- Yanni, D.S.; Ozgur, B.M.; Louis, R.G.; Shekhtman, Y.; Iyer, R.R.; Boddapati, V.; Iyer, A.; Patel, P.D.; Jani, R.; Cummock, M.; et al. Real-time navigation guidance with intraoperative CT imaging for pedicle screw placement using an augmented reality head-mounted display: A proof-of-concept study. Neurosurg. Focus 2021, 51, E11. [Google Scholar] [CrossRef]
- Condino, S.; Cutolo, F.; Cattari, N.; Colangeli, S.; Parchi, P.D.; Piazza, R.; Ruinato, A.D.; Capanna, R.; Ferrari, V. Hybrid simulation and planning platform for cryosurgery with Microsoft Hololens. Sensors 2021, 21, 4450. [Google Scholar] [CrossRef]
- Majak, M.; Żuk, M.; Świątek Najwer, E.; Popek, M.; Pietruski, P. Augmented reality visualization for aiding biopsy procedure according to computed tomography based virtual plan. Acta Bioeng. Biomech. 2021, 23, 81–89. [Google Scholar] [CrossRef]
- Zhou, Z.; Jiang, S.; Yang, Z.; Xu, B.; Jiang, B. Surgical navigation system for brachytherapy based on mixed reality using a novel stereo registration method. Virtual Real. 2021, 25, 975–984. [Google Scholar] [CrossRef]
- Gu, W.; Shah, K.; Knopf, J.; Josewski, C.; Unberath, M. A calibration-free workflow for image-based mixed reality navigation of total shoulder arthroplasty. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2021, 10, 243–251. [Google Scholar] [CrossRef]
- Dennler, C.; Safa, N.A.; Bauer, D.E.; Wanivenhaus, F.; Liebmann, F.; Götschi, T.; Farshad, M. Augmented Reality Navigated Sacral-Alar-Iliac Screw Insertion. Int. J. Spine Surg. 2021, 15, 161–168. [Google Scholar] [CrossRef]
- Kriechling, P.; Roner, S.; Liebmann, F.; Casari, F.; Fürnstahl, P.; Wieser, K. Augmented reality for base plate component placement in reverse total shoulder arthroplasty: A feasibility study. Arch. Orthop. Trauma Surg. 2021, 141, 1447–1453. [Google Scholar] [CrossRef]
- Liu, K.; Gao, Y.; Abdelrehem, A.; Zhang, L.; Chen, X.; Xie, L.; Wang, X. Augmented reality navigation method for recontouring surgery of craniofacial fibrous dysplasia. Sci. Rep. 2021, 11, 10043. [Google Scholar] [CrossRef]
- Liu, X.; Sun, J.; Zheng, M.; Cui, X. Application of Mixed Reality Using Optical See-Through Head-Mounted Displays in Transforaminal Percutaneous Endoscopic Lumbar Discectomy. Biomed Res. Int. 2021, 2021, e9717184. [Google Scholar] [CrossRef]
- Rae, E.; Lasso, A.; Holden, M.S.; Morin, E.; Levy, R.; Fichtinger, G. Neurosurgical burr hole placement using the Microsoft HoloLens. In Proceedings of the Medical Imaging 2018: Image-Guided Procedures, Robotic Interventions, and Modeling, Houston, TX, USA, 10–15 February 2018; International Society for Optics and Photonics: Bellingham, WA, USA, 2018; 10576, p. 105760T. [Google Scholar]
- Center for Devices and Radiological Health. Applying Human Factors and Usability Engineering to Medical Devices; FDA: Silver Spring, MD, USA, 2016. [Google Scholar]
- Fitzpatrick, J.M. The role of registration in accurate surgical guidance. Proc. Inst. Mech. Eng. Part J. Eng. Med. 2010, 224, 607–622. [Google Scholar] [CrossRef] [Green Version]
- Sielhorst, T.; Bichlmeier, C.; Heining, S.M.; Navab, N. Depth perception—A major issue in medical AR: Evaluation study by twenty surgeons. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Berlin/Heidelberg, Germany, 2006; pp. 364–372. [Google Scholar]
- Yeo, C.T.; MacDonald, A.; Ungi, T.; Lasso, A.; Jalink, D.; Zevin, B.; Fichtinger, G.; Nanji, S. Utility of 3D reconstruction of 2D liver computed tomography/magnetic resonance images as a surgical planning tool for residents in liver resection surgery. J. Surg. Educ. 2018, 75, 792–797. [Google Scholar] [CrossRef]
- Pelanis, E.; Kumar, R.P.; Aghayan, D.L.; Palomar, R.; Fretland, Å.A.; Brun, H.; Elle, O.J.; Edwin, B. Use of mixed reality for improved spatial understanding of liver anatomy. Minim. Invasive Ther. Allied Technol. 2020, 29, 154–160. [Google Scholar] [CrossRef]
- Shibata, T.; Kim, J.; Hoffman, D.M.; Banks, M.S. The zone of comfort: Predicting visual discomfort with stereo displays. J. Vis. 2011, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Hasson, Y.; Tekin, B.; Bogo, F.; Laptev, I.; Pollefeys, M.; Schmid, C. Leveraging photometric consistency over time for sparsely supervised hand-object reconstruction. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 14–19 June 2020; pp. 571–580. [Google Scholar]
- Hein, J.; Seibold, M.; Bogo, F.; Farshad, M.; Pollefeys, M.; Fürnstahl, P.; Navab, N. Towards markerless surgical tool and hand pose estimation. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Doughty, M.; Ghugre, N.R. HMD-EgoPose: Head-mounted display-based egocentric marker-less tool and hand pose estimation for augmented surgical guidance. Int. J. Comput. Assist. Radiol. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Twinanda, A.P.; Shehata, S.; Mutter, D.; Marescaux, J.; De Mathelin, M.; Padoy, N. Endonet: A deep architecture for recognition tasks on laparoscopic videos. IEEE Trans. Med. Imaging 2016, 36, 86–97. [Google Scholar] [CrossRef] [Green Version]
- Doughty, M.; Singh, K.; Ghugre, N.R. SurgeonAssist-Net: Towards Context-Aware Head-Mounted Display-Based Augmented Reality for Surgical Guidance. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; Springer: Berlin/Heidelberg, Germany, 2021; pp. 667–677. [Google Scholar]
Figure 1.
The continuum proposed by Milgram and Kishino [1] describing the interactions between reality and virtuality in creating augmented reality experiences. Reproduced without modification from Wikimedia Commons (source: https://commons.wikimedia.org/wiki/File:Virtuality_continuum_2-en.svg, (accessed on 23 March 2022) licensed under: https://creativecommons.org/licenses/by-sa/4.0/deed.en (accessed on accessed on 23 March 2022).
Figure 1.
The continuum proposed by Milgram and Kishino [1] describing the interactions between reality and virtuality in creating augmented reality experiences. Reproduced without modification from Wikimedia Commons (source: https://commons.wikimedia.org/wiki/File:Virtuality_continuum_2-en.svg, (accessed on 23 March 2022) licensed under: https://creativecommons.org/licenses/by-sa/4.0/deed.en (accessed on accessed on 23 March 2022).

Figure 2.
A simplified image representation of video see-through (a) and optical see-through (b) head-mounted displays (HMDs). Video see-through HMDs use an opaque video display to present virtual content combined with video of the real world. Real world video is typically captured by front-facing red-green-blue cameras on the front of the HMD. Optical see-through HMDs make use of a transparent optical combiner to merge virtual content, projected into the field of view of the wearer, with a view of the real world.
Figure 2.
A simplified image representation of video see-through (a) and optical see-through (b) head-mounted displays (HMDs). Video see-through HMDs use an opaque video display to present virtual content combined with video of the real world. Real world video is typically captured by front-facing red-green-blue cameras on the front of the HMD. Optical see-through HMDs make use of a transparent optical combiner to merge virtual content, projected into the field of view of the wearer, with a view of the real world.

Figure 3.
Images of the prominent commercially available optical see-through head-mounted displays. (a) The Google Glass 2 Enterprise Edition with on-board computing (Google, Mountain View, CA, USA). (b) The Microsoft HoloLens 2 headset with on-board computing (Microsoft, Redmond, WA, USA). (c) The Magic Leap 1 headset with a separate computing pad and controllers (Magic Leap, Plantation, FL, USA).
Figure 3.
Images of the prominent commercially available optical see-through head-mounted displays. (a) The Google Glass 2 Enterprise Edition with on-board computing (Google, Mountain View, CA, USA). (b) The Microsoft HoloLens 2 headset with on-board computing (Microsoft, Redmond, WA, USA). (c) The Magic Leap 1 headset with a separate computing pad and controllers (Magic Leap, Plantation, FL, USA).

Figure 4.
Depiction of the fundamentals of marker-based tracking. The intrinsic camera parameters serve to project three-dimensional (3D) content in the camera coordinate system to its two-dimensional (2D) representation on the camera image plane by perspective projection. The extrinsic parameters relate the position and orientation of the world coordinate frame to the camera coordinate frame. Combined, the intrinsic and extrinsic camera parameters allow the relation of 3D points in the world to 2D points on the camera image plane and enable marker-based tracking and precise augmentation of virtual content.
Figure 4.
Depiction of the fundamentals of marker-based tracking. The intrinsic camera parameters serve to project three-dimensional (3D) content in the camera coordinate system to its two-dimensional (2D) representation on the camera image plane by perspective projection. The extrinsic parameters relate the position and orientation of the world coordinate frame to the camera coordinate frame. Combined, the intrinsic and extrinsic camera parameters allow the relation of 3D points in the world to 2D points on the camera image plane and enable marker-based tracking and precise augmentation of virtual content.

Figure 5.
Search strategy of our systematic review.

Figure 6.
Article distribution per year of the conducted literature review from 2014 to 2022 (Q1). We have included the count provided by Birlo et al. for the years 2014 to 2020 [6] in blue with our contributions in green. As the review was conducted in the first quarter of 2022, an estimate of the full-year article publication count was arrived at by multiplying the count by four.
Figure 6.
Article distribution per year of the conducted literature review from 2014 to 2022 (Q1). We have included the count provided by Birlo et al. for the years 2014 to 2020 [6] in blue with our contributions in green. As the review was conducted in the first quarter of 2022, an estimate of the full-year article publication count was arrived at by multiplying the count by four.

Figure 7.
A taxonomy of the required components of an effective augmented reality based navigation solution for image guided surgery. Preoperative (preop.) data, such as magnetic resonance imaging (MRI) and computed tomography (CT), along with intraoperative (intraop.) data, such as ultrasound (US) and fluoroscopy (FL), are indicated. In the view category, the display device for visualization of virtual content is included, these could be optical see-through head-mounted displays (OST-HMDs) or video see-through head-mounted displays (VST-HMDs) for example. Our taxonomy is modified from the description provided by Kersten-Oertel et al. [44].
Figure 7.
A taxonomy of the required components of an effective augmented reality based navigation solution for image guided surgery. Preoperative (preop.) data, such as magnetic resonance imaging (MRI) and computed tomography (CT), along with intraoperative (intraop.) data, such as ultrasound (US) and fluoroscopy (FL), are indicated. In the view category, the display device for visualization of virtual content is included, these could be optical see-through head-mounted displays (OST-HMDs) or video see-through head-mounted displays (VST-HMDs) for example. Our taxonomy is modified from the description provided by Kersten-Oertel et al. [44].

Figure 8.
Distribution of the 57 articles included in the review based on the surgical speciality discussed.
Figure 8.
Distribution of the 57 articles included in the review based on the surgical speciality discussed.

Figure 9.
Distribution of the 57 articles included in the review based on the display device used.

Figure 10.
Demonstration of the difference between direct overlay of virtual content and adjacent overlay of virtual content. Direct overlay will include virtual content which is directly superimposed with the patient anatomy (a). Adjacent overlay involves the placement of virtual content next to the patient to improve data accessibility (b).
Figure 10.
Demonstration of the difference between direct overlay of virtual content and adjacent overlay of virtual content. Direct overlay will include virtual content which is directly superimposed with the patient anatomy (a). Adjacent overlay involves the placement of virtual content next to the patient to improve data accessibility (b).

Figure 11.
Distribution of the 57 articles included in the review based on the reported human factors related considerations. Human factors considerations included risk of error (ROE), spatial awareness (SPWR), ease of use (EOU), perception (PER), ergonomics (ERGO), attention shift (ATS), interaction challenges (INT), mental mapping (MM), context (CTXT), hand-eye coordination (HE), and occlusion (OCCL).
Figure 11.
Distribution of the 57 articles included in the review based on the reported human factors related considerations. Human factors considerations included risk of error (ROE), spatial awareness (SPWR), ease of use (EOU), perception (PER), ergonomics (ERGO), attention shift (ATS), interaction challenges (INT), mental mapping (MM), context (CTXT), hand-eye coordination (HE), and occlusion (OCCL).


{kind=link}
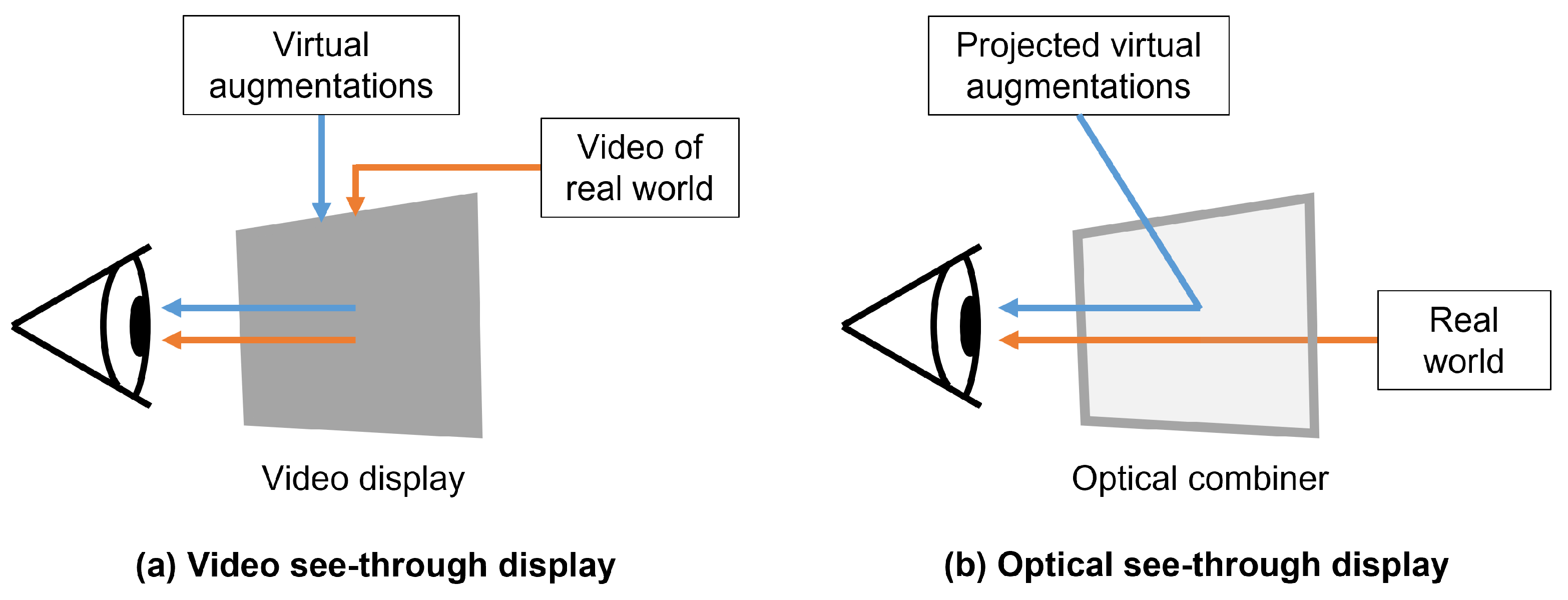{kind=link}
{kind=link}
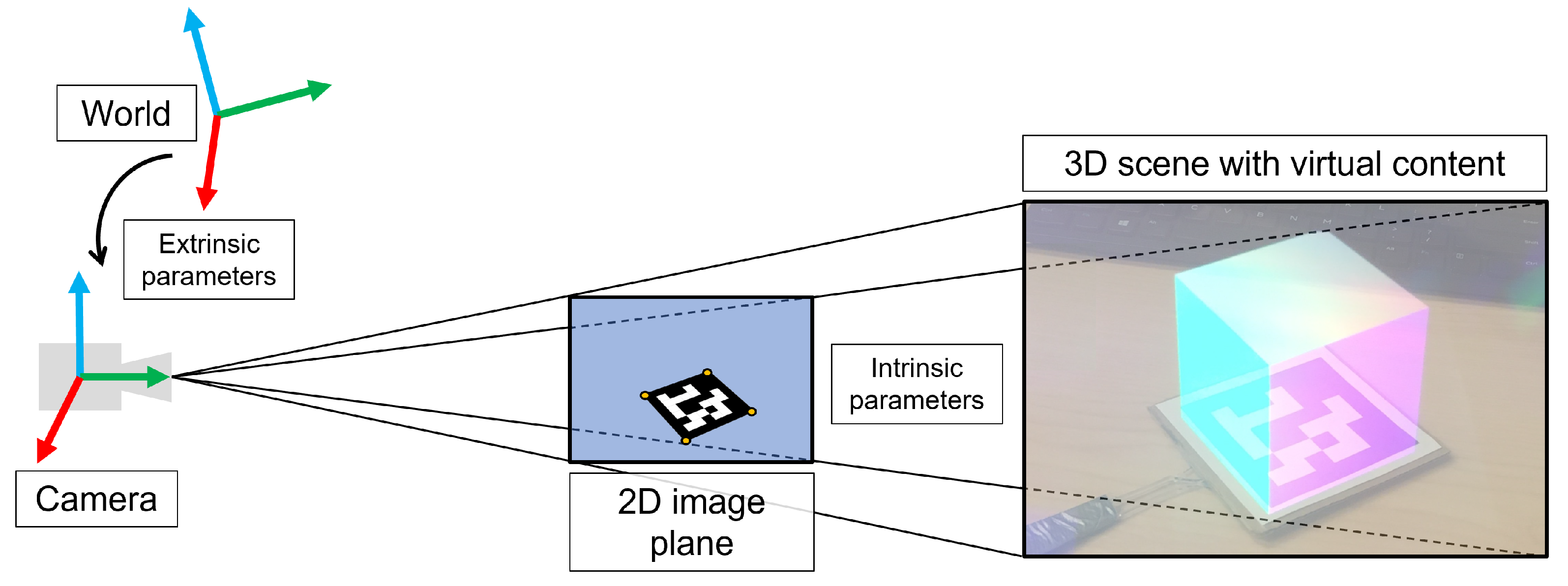{kind=link}
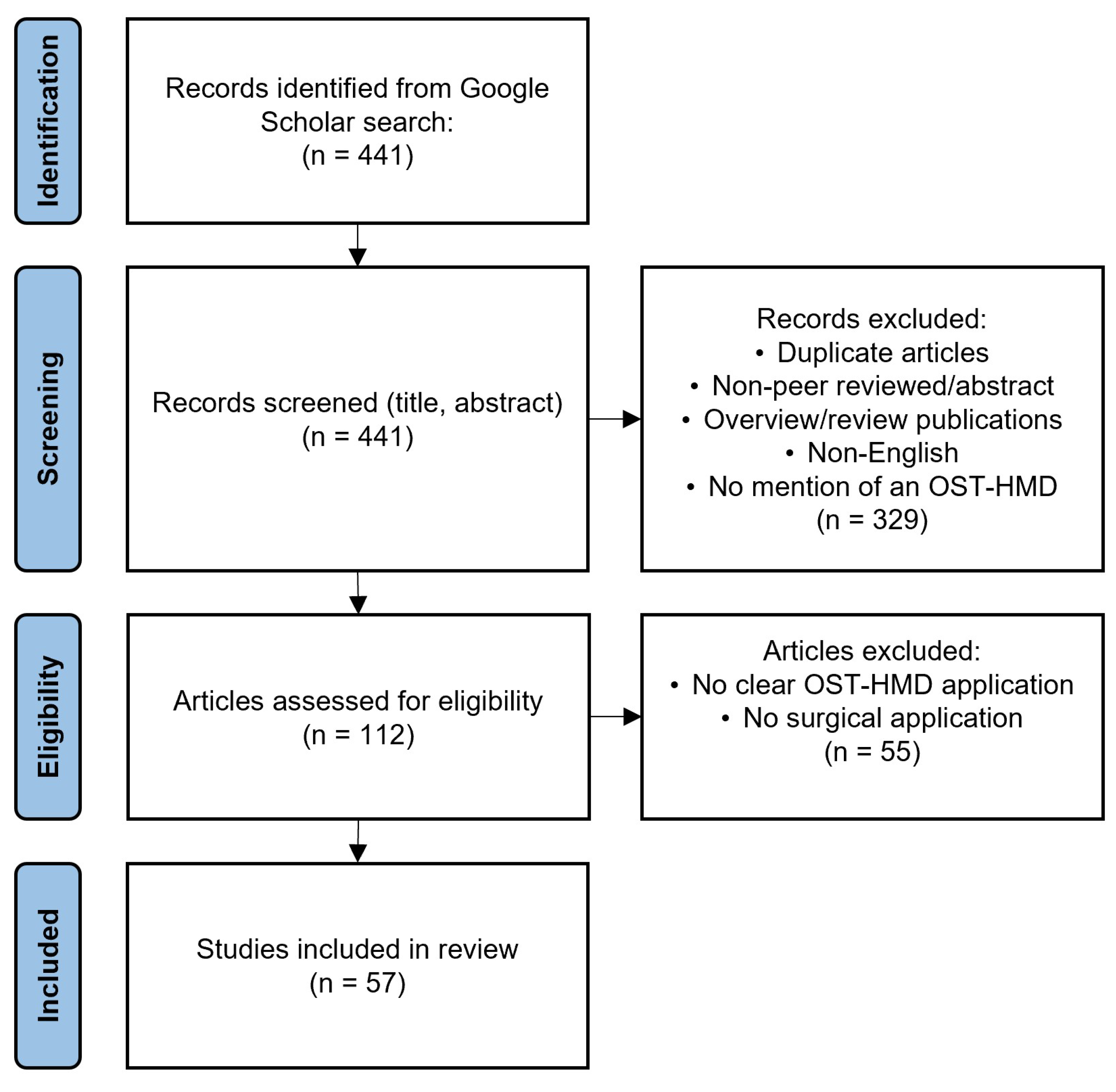{kind=link}
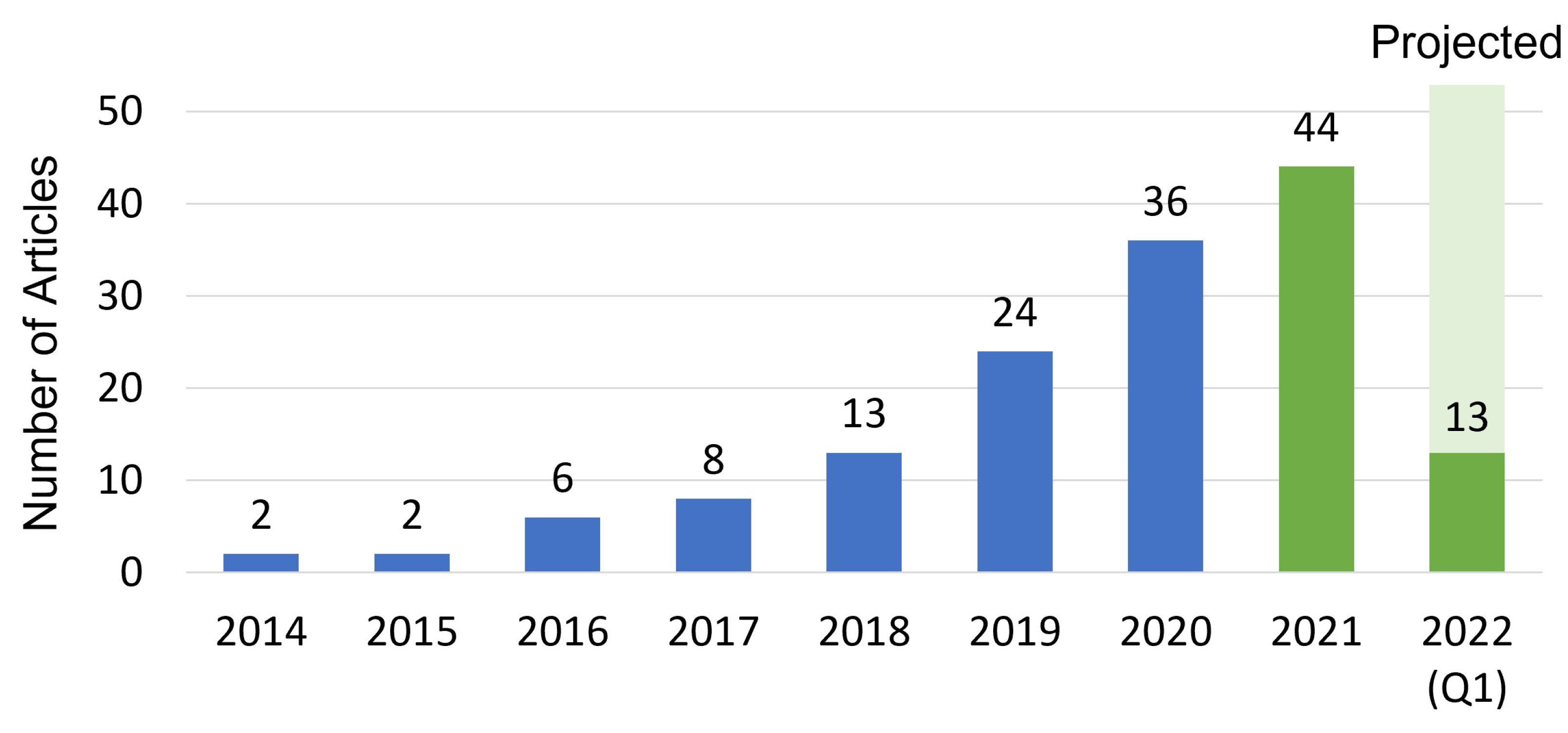{kind=link}
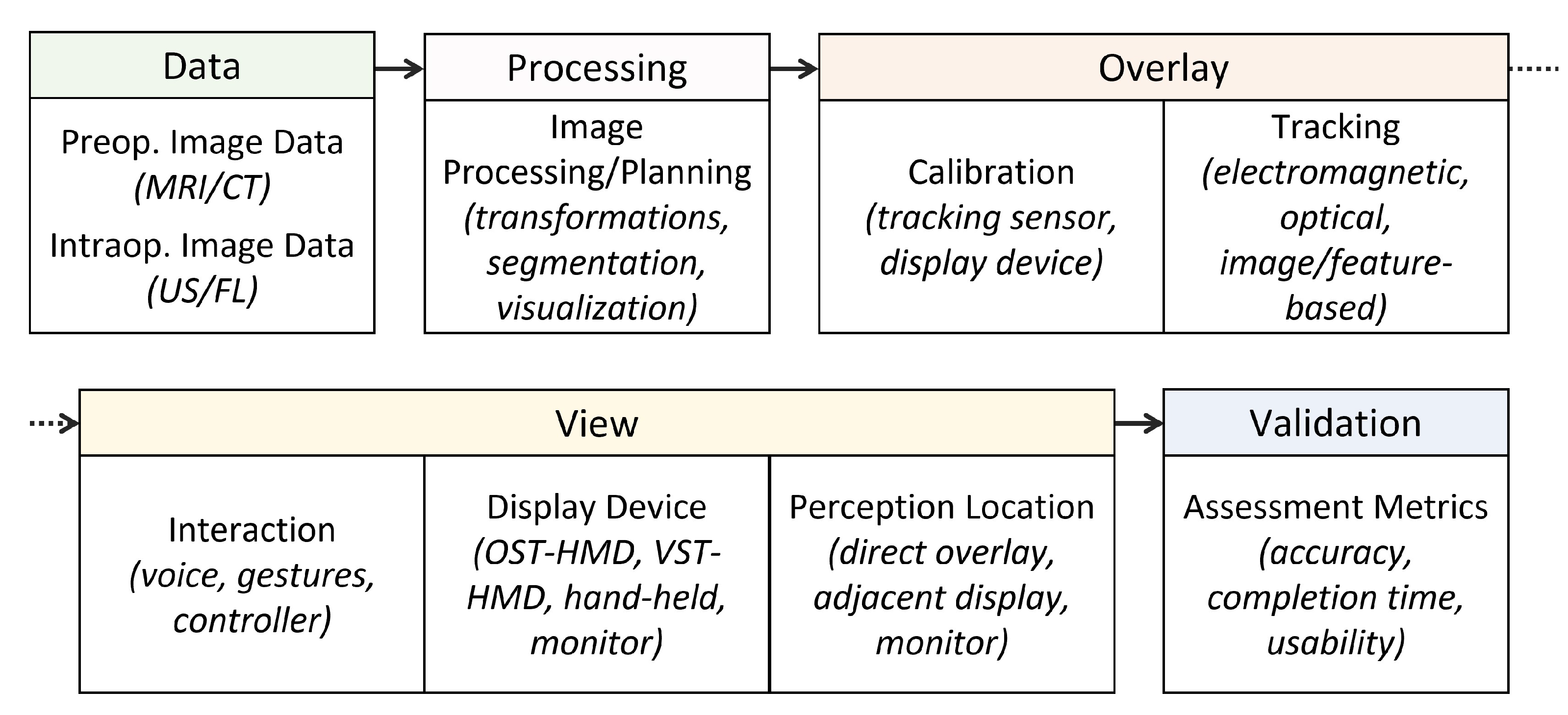{kind=link}
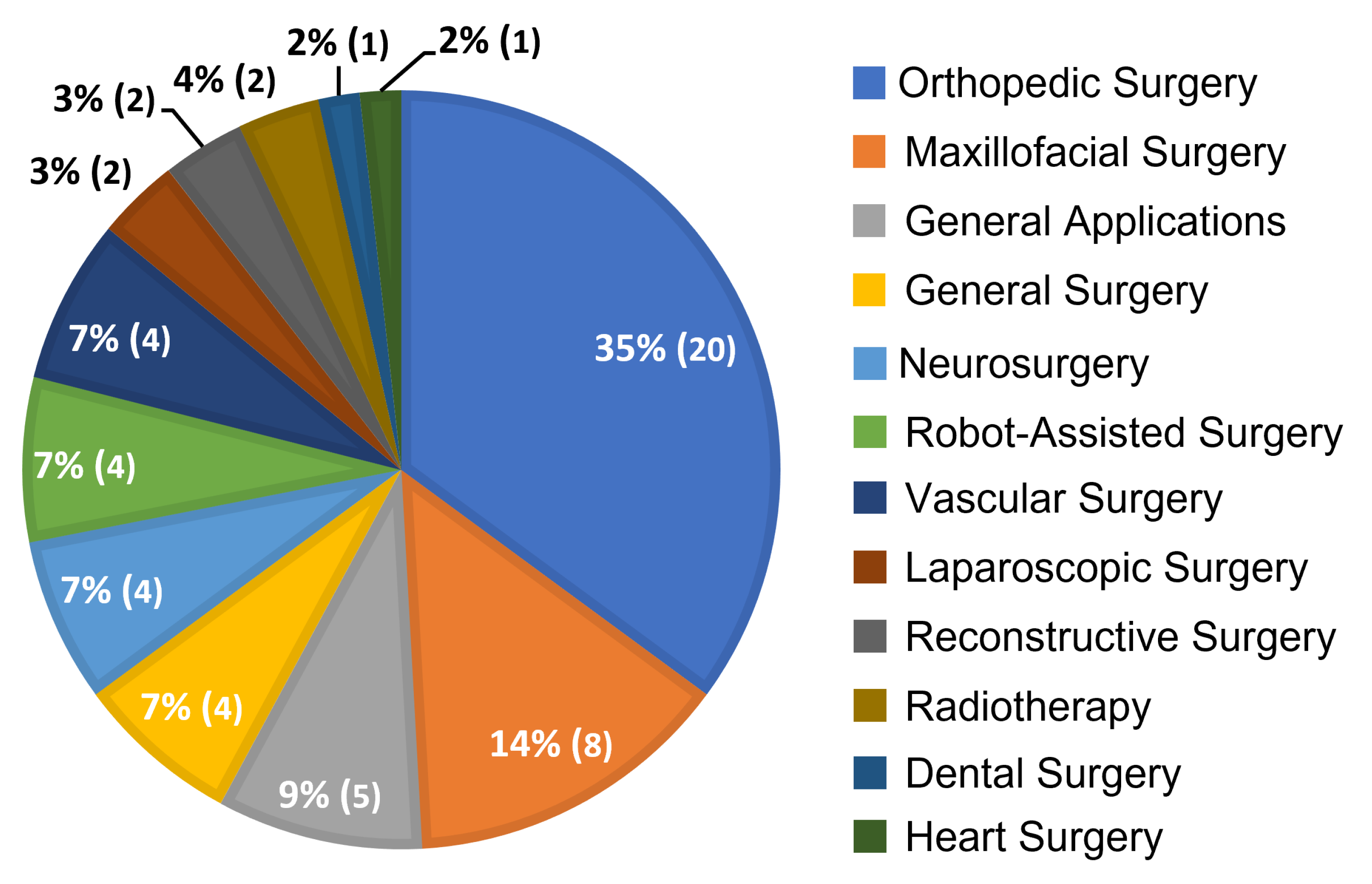{kind=link}
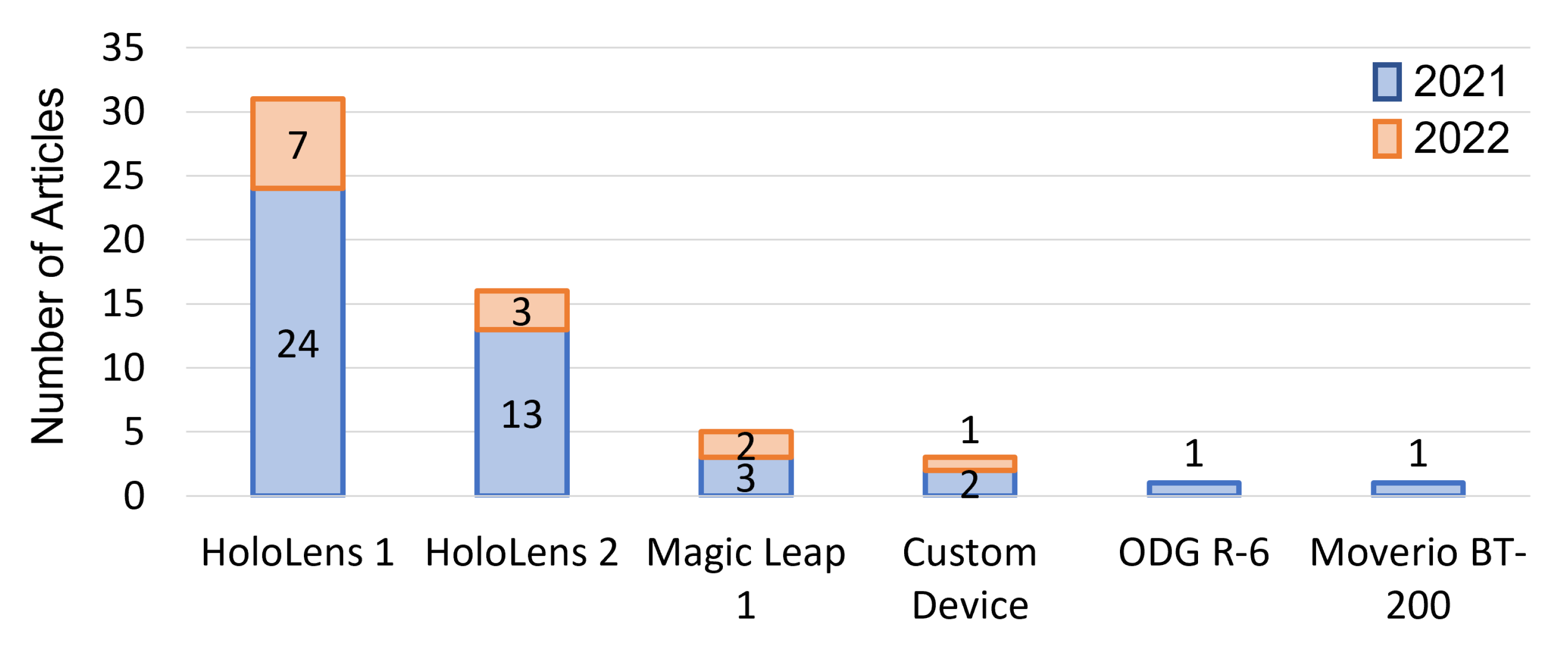{kind=link}
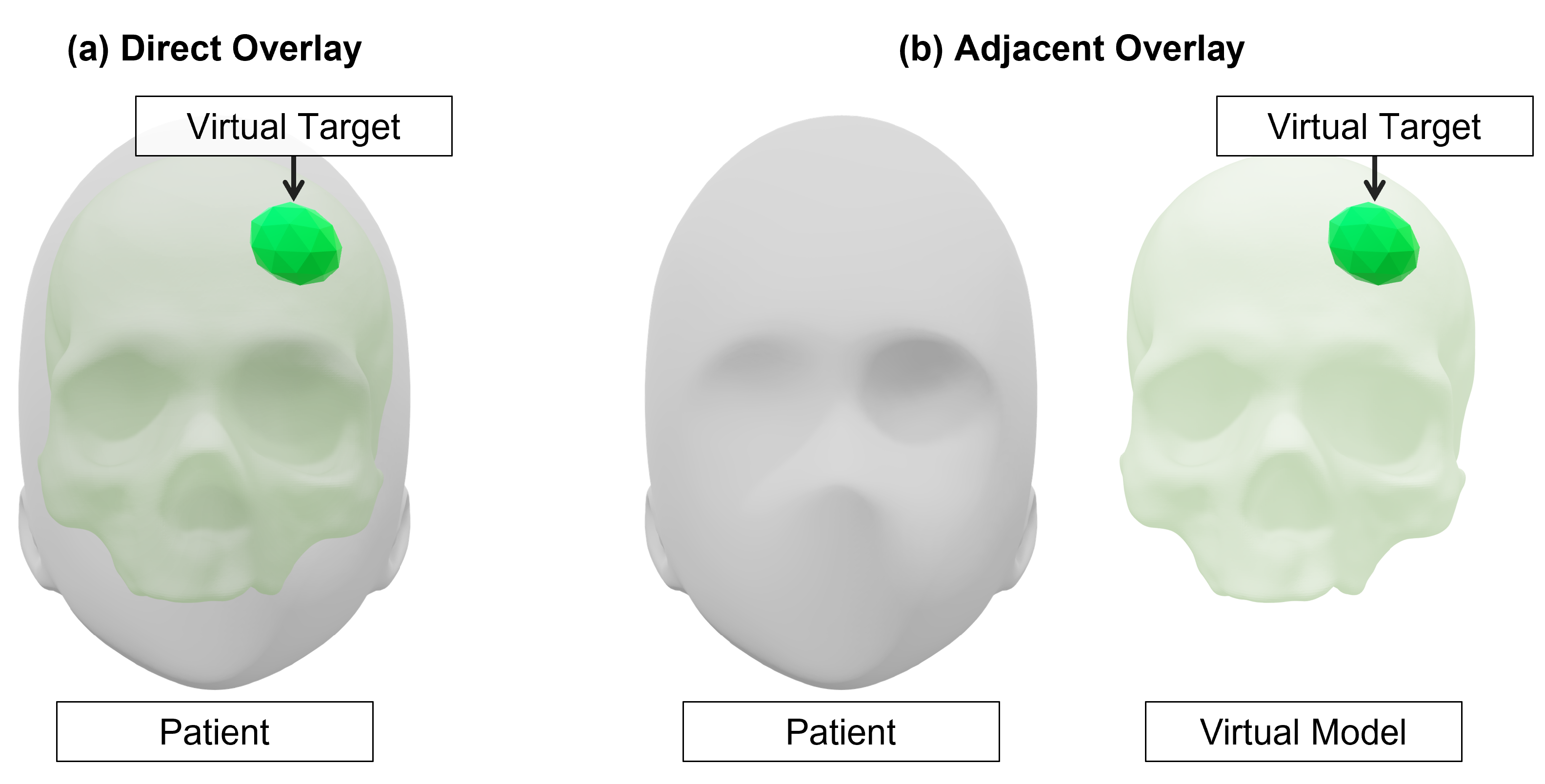{kind=link}
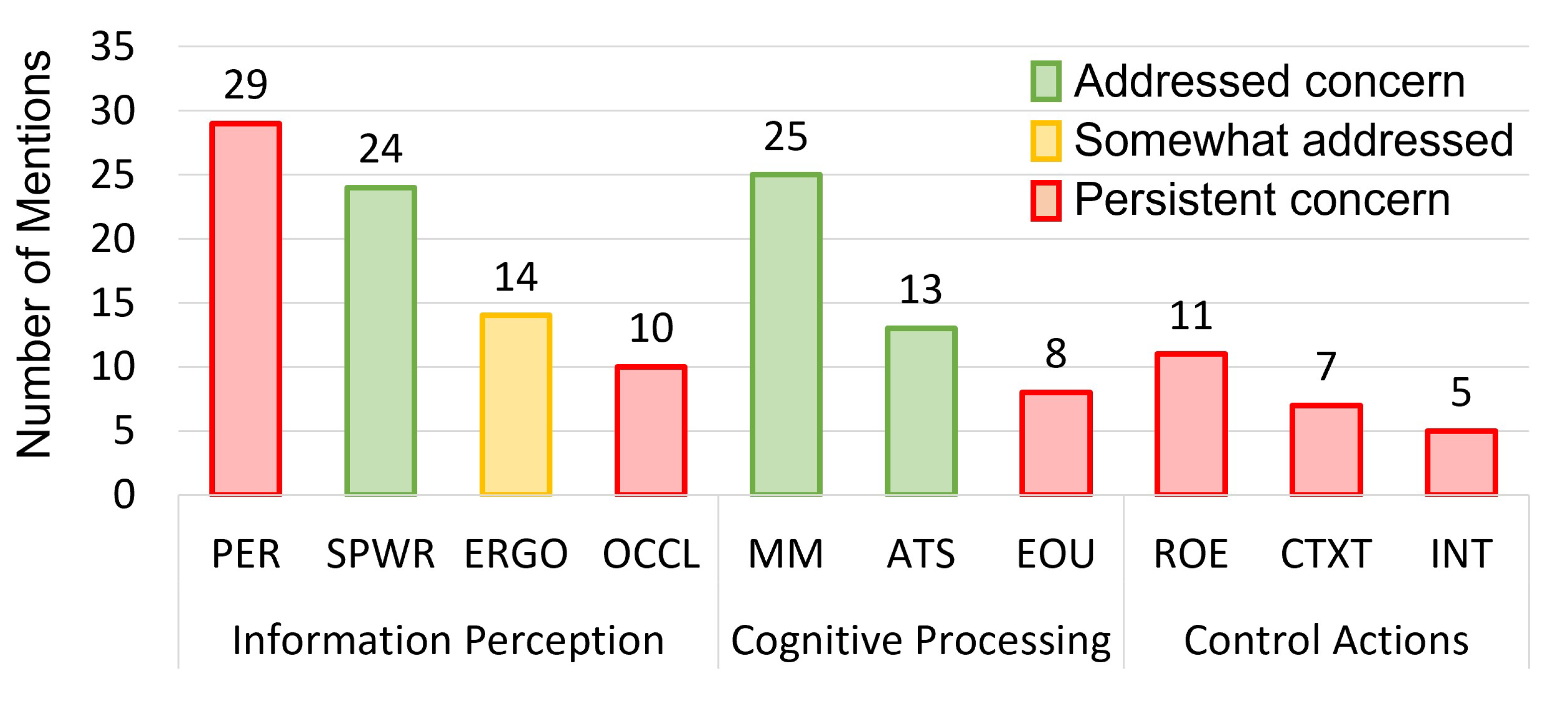{kind=link}
Table 1.
Summary of technical specifications for commercially available optical see-through head-mounted displays.
Table 1.
Summary of technical specifications for commercially available optical see-through head-mounted displays.
| Specifications | Google Glass 2 | HoloLens 1 | HoloLens 2 | Magic Leap 1 | Magic Leap 2 |
|---|---|---|---|---|---|
| Optics | Beam Splitter | Waveguide | Waveguide | Waveguide | Waveguide |
| Resolution | px | px | px | px | px |
| Field of View | diagonal | ||||
| Focal Planes | Single Fixed | Single Fixed | Single Fixed | Two Fixed | Single Fixed |
| Computing | On-board | On-board | On-board | External pad | External pad |
| SLAM | 6DoF | 6DoF | 6DoF | 6DoF | 6DoF |
| Eye Tracking | No | No | Yes | Yes | Yes |
| Weight | 46 g | 579 g | 566 g | 345 g | 260 g |
| Design | Glasses-like | Hat-like | Hat-like | Glasses-like | Glasses-like |
| Interaction | Touchpad | Head, hand, voice | Hand, eye, voice | Controller | Eye, controller |
| Release Date | 2019 | 2016 | 2019 | 2018 | 2022 |
| Price | $999 | $3000 | $3500 | $2295 | $3299 |
| Status | Available | Discontinued | Available | Available | Upcoming |
Table 2.
Papers categorized by the data type they employed. Some articles included a combination of preoperative and intraoperative data.
Table 2.
Papers categorized by the data type they employed. Some articles included a combination of preoperative and intraoperative data.
| Data: Preoperative or Intraoperative | Number of Articles |
|---|---|
| Preoperative | |
| Computed Tomography (CT) | 34 |
| Magnetic Resonance Imaging (MRI) | 7 |
| CT and/or MRI | 6 |
| Prerecorded Videos | 1 |
| Intraoperative | |
| Fluoroscopy | 4 |
| Ultrasound | 3 |
| Telestrations/Virtual Arrows and Annotations | 3 |
| Cone Beam CT | 3 |
| Endoscope Video | 2 |
| Patient Sensors/Monitoring Equipment | 1 |
| Simulated Intraoperative Data | 1 |
Table 3.
Papers categorized by the data processing type used. Some articles included a combination of processing types, such as volume and surface rendered models.
Table 3.
Papers categorized by the data processing type used. Some articles included a combination of processing types, such as volume and surface rendered models.
| Processing | Number of Articles |
|---|---|
| Three-Dimensional | |
| Surface Models | 39 |
| Planning Information | 8 |
| Raw Data | 5 |
| Volume Models | 4 |
| Printed Models | 3 |
| Two-Dimensional | |
| Telestrations | 4 |
| Raw Data | 3 |
Table 4.
Papers categorized by the overlay type used. External trackers (surgical navigation suites) were used in conjunction with an optical see-through head-mounted display to co-locate the headset with relevant tracked surgical tools in frame. We indicate the frequency of commercial tracking system usage and the type of tracking marker used.
Table 4.
Papers categorized by the overlay type used. External trackers (surgical navigation suites) were used in conjunction with an optical see-through head-mounted display to co-locate the headset with relevant tracked surgical tools in frame. We indicate the frequency of commercial tracking system usage and the type of tracking marker used.
| Overlay | Count | Tracking Marker | Count |
|---|---|---|---|
| External Tracker | External Markers | ||
| Northern Digital Inc. Polaris | 7 | Retroreflective Spheres | 11 |
| Northern Digital Inc. EM/Aurora | 3 | Electromagnetic | 3 |
| ClaroNav MicronTracker | 2 | Visible | 2 |
| Optitrack | 1 | ||
| Medtronic SteathStation | 1 | ||
| OST-HMD Camera (RGB/Infrared) | Optical Markers | ||
| HoloLens 1 | 19 | Vuforia | 10 |
| HoloLens 2 | 10 | ArUco | 9 |
| Custom | 3 | Custom | 4 |
| Magic Leap 1 | 1 | Retroreflective Spheres | 2 |
| OST-HMD Display Calibration | QR-Code | 2 | |
| SPAAM/similar | 2 | Marker-Less | 2 |
| AprilTag | 1 | ||
| Manual Placement | |||
| Surgeon | 8 | ||
| Other | 3 |
Table 5.
Papers categorized by the view type used. Interaction types included voice (VO), gesture (GE), gaze (GA), keyboard (KB), head pose (HP), pointer (PO), and controller (CNT). Display devices included the HoloLens 1 (HL1), HoloLens 2 (HL2), and Magic Leap One (ML1). Perception location included direct overlay (DO) or adjacent overlay (AO). Not applicable (N/A) methods are indicated.
Table 5.
Papers categorized by the view type used. Interaction types included voice (VO), gesture (GE), gaze (GA), keyboard (KB), head pose (HP), pointer (PO), and controller (CNT). Display devices included the HoloLens 1 (HL1), HoloLens 2 (HL2), and Magic Leap One (ML1). Perception location included direct overlay (DO) or adjacent overlay (AO). Not applicable (N/A) methods are indicated.
| View | Interaction | Display Device | Perception Location |
|---|---|---|---|
| Ackermann et al., 2021 [45] | N/A | HL1 | DO |
| Cattari et al., 2021 [83] | N/A | Custom | DO |
| Condino et al., 2021 [66] | N/A | Custom | DO |
| Condino et al., 2021 [96] | VO, GE | HL1 | DO |
| Dennler et al., 2021 [46] | VO, GE | HL1 | AO |
| Dennler et al., 2021 [100] | N/A | HL1 | DO |
| Farshad et al., 2021 [47] | VO, GE | HL2 | DO |
| Fick et al., 2021 [63] | VO, GE | HL1 | DO |
| Gao et al., 2021 [54] | VO | HL1 | DO |
| Gasques et al., 2021 [58] | VO, GE, PO | HL1 | DO |
| Gsaxner et al., 2021 [60] | N/A | HL2 | DO |
| Gsaxner et al., 2021 [75] | GA, GE | HL2 | DO |
| Gu et al., 2021 [99] | GA, GE | HL2 | DO |
| Gu et al., 2021 [48] | GE | HL1 | DO |
| Heinrich et al., 2021 [73] | VO, GE | HL1 | DO |
| Iqbal et al., 2021 [55] | N/A | HL1 | AO |
| Ivan et al., 2021 [62] | GE | HL1 | DO |
| Ivanov et al., 2021 [74] | GE | HL2 | DO |
| Johnson et al., 2021 [81] | N/A | ODG R-6 | AO |
| Kimmel et al., 2021 [86] | VO, GE | HL1 | AO |
| Kitagawa et al., 2021 [72] | N/A | HL2 | AO |
| Kriechling et al., 2021 [88] | VO, GE | HL1 | DO |
| Kriechling et al., 2021 [101] | VO, GE | HL1 | DO |
| Kunz et al., 2021 [64] | GE | HL1 | DO |
| Lee et al., 2021 [87] | N/A | HL2 | DO |
| Li et al., 2021 [68] | N/A | HL1 | DO |
| Lim et al., 2021 [80] | GE | HL2 | DO |
| Lin et al., 2021 [57] | GE | ML1 | DO |
| Liu et al., 2021 [102] | VO | HL1 | AO |
| Liu et al., 2021 [103] | N/A | HL2 | DO |
| Liu et al., 2021 [69] | N/A | HL1 | DO |
| Majak et al., 2021 [97] | N/A | Moverio BT-200 | DO |
| Qi et al., 2021 [65] | GE | HL2 | DO |
| Rai et al., 2021 [59] | CNT | ML1 | DO |
| Schlueter-Brust et al., 2021 [51] | GE | HL2 | DO |
| Spirig et al., 2021 [50] | VO, GE | HL1 | DO |
| Stewart et al., 2021 [56] | VO, GE | HL1 | AO |
| Tang et al., 2021 [52] | GE | HL1 | AO |
| Tarutani et al., 2021 [70] | GE | HL2 | AO |
| Teatini et al., 2021 [49] | GE | HL1 | DO |
| Tu et al., 2021 [82] | VO, GE | HL2 | DO |
| Velazco-Garcia et al., 2021 [78] | VO, GE | HL1 | AO |
| Yanni et al., 2021 [95] | CNT | ML1 | DO |
| Zhou et al., 2021 [98] | VO, GE | HL1 | DO |
| Carbone et al., 2022 [90] | N/A | Custom | DO |
| Doughty et al., 2022 [33] | GE | HL2 | DO |
| Frisk et al., 2022 [84] | CNT | ML1 | DO |
| Hu et al., 2022 [77] | KB | HL1 | DO |
| Johnson et al., 2022 [71] | VC | HL2 | DO |
| Ma et al., 2022 [91] | HP | HL1 | DO |
| Nguyen et al., 2022 [92] | VO | HL1 | DO |
| Puladi et al., 2022 [85] | GE | HL1 | DO |
| Tu et al., 2022 [93] | GE | HL2 | DO |
| Uhl et al., 2022 [67] | CNT | ML1 | DO |
| Von Atzigen et al., 2022 [76] | VO | HL1 | DO |
| Yang et al., 2022 [53] | VO, GE | HL1 | DO |
| Zhang et al., 2022 [61] | N/A | HL1 | DO |
Table 6.
Papers categorized by the validation type employed. Models for evaluation included phantom models (PHA), cadaver models (CAD), animals (ANI), and patients (PAT). Human factors considerations included risk of error (ROE), spatial awareness (SPWR), ease of use (EOU), perception (PER), ergonomics (ERGO), attention shift (ATS), interaction challenges (INT), mental mapping (MM), context (CTXT), hand-eye coordination (HE), and occlusion (OCCL). Not applicable (N/A) methods are indicated.
Table 6.
Papers categorized by the validation type employed. Models for evaluation included phantom models (PHA), cadaver models (CAD), animals (ANI), and patients (PAT). Human factors considerations included risk of error (ROE), spatial awareness (SPWR), ease of use (EOU), perception (PER), ergonomics (ERGO), attention shift (ATS), interaction challenges (INT), mental mapping (MM), context (CTXT), hand-eye coordination (HE), and occlusion (OCCL). Not applicable (N/A) methods are indicated.
| Validation | Evaluation | Accuracy | Human Factors |
|---|---|---|---|
| Ackermann et al., 2021 [45] | CAD | mm RMS, | ROE, SPWR, EOU |
| Cattari et al., 2021 [83] | PHA | mm | PER, ERGO, ATS, MM, CTXT |
| Condino et al., 2021 [66] | PHA | mm | ATS, PER, SPWR, CTXT, INT |
| Condino et al., 2021 [96] | PHA, PAT | N/A | SPWR, MM, PER |
| Dennler et al., 2021 [46] | PAT | N/A | ERGO, SPWR, ATS, PER |
| Dennler et al., 2021 [100] | PHA | mm entry, | ATS, ROE |
| Farshad et al., 2021 [47] | PAT | mm entry, | ATS, ROE, ERGO, PER |
| Fick et al., 2021 [63] | PAT | mm | MM, ATS, SPWR |
| Gao et al., 2021 [54] | PHA | SPWR, MM, PER | |
| Gasques et al., 2021 [58] | PHA, CAD | N/A | ROE, PER, CTXT |
| Gsaxner et al., 2021 [60] | PHA | mm RMS | PER, INT, CTXT, SPWR |
| Gsaxner et al., 2021 [75] | PHA | N/A | EOU, PER, MM |
| Gu et al., 2021 [99] | PHA | mm, | PER, MM, SPWR, OCCL, CTXT |
| Gu et al., 2021 [48] | PHA | mm, | OCCL, PER |
| Heinrich et al., 2021 [73] | PHA | N/A | PER, HE |
| Iqbal et al., 2021 [55] | PAT | Surface Roughness | EOU, ERGO, PER, MM, SPWR |
| Ivan et al., 2021 [62] | PAT | Trace Overlap | ERGO, SPWR |
| Ivanov et al., 2021 [74] | PAT | mm | MM, PER |
| Johnson et al., 2021 [81] | PHA | N/A | ERGO, EOU |
| Kimmel et al., 2021 [86] | PAT | N/A | CTXT |
| Kitagawa et al., 2021 [72] | PAT | N/A | SPWR, EOU |
| Kriechling et al., 2021 [88] | CAD | mm | N/A |
| Kriechling et al., 2021 [101] | CAD | mm | N/A |
| Kunz et al., 2021 [64] | PHA | mm | CTXT, PER, ERGO |
| Lee et al., 2021 [87] | PHA | N/A | PER, INT, SPWR |
| Li et al., 2021 [68] | PHA, ANI | mm | PER, INT, SPWR |
| Lim et al., 2021 [80] | PHA | N/A | N/A |
| Lin et al., 2021 [57] | PHA | mm | CTXT |
| Liu et al., 2021 [102] | PAT | mm | SPWR, MM |
| Liu et al., 2021 [103] | PAT | Radiation Exposure | ERGO, EOU |
| Liu et al., 2021 [69] | PHA | mm | CTXT, PER |
| Majak et al., 2021 [97] | PHA | mm | MM, ATS, SPWR |
| Qi et al., 2021 [65] | PAT | mm | MM, SPWR, ROE |
| Rai et al., 2021 [59] | PAT | N/A | SPWR, EOU |
| Schlueter-Brust et al., 2021 [51] | PHA | 3 mm | OCCL, PER |
| Spirig et al., 2021 [50] | CAD | mm | MM, ATS, SPWR |
| Stewart et al., 2021 [56] | PHA | N/A | ATS, ERGO |
| Tang et al., 2021 [52] | PAT | N/A | HE, SPWR, MM, PER |
| Tarutani et al., 2021 [70] | PHA | mm | ROE, SPWR |
| Teatini et al., 2021 [49] | PHA | mm | SPWR, MM, PER, HE, ROE |
| Tu et al., 2021 [82] | PHA, CAD | mm | MM, OCCL, HE, PER, ERGO |
| Velazco-Garcia et al., 2021 [78] | PHA | N/A | MM, CTXT, SPWR |
| Yanni et al., 2021 [95] | PHA | N/A | ERGO, MM, PER |
| Zhou et al., 2021 [98] | PHA, ANI | mm | OCCL, INT, ROE |
| Carbone et al., 2021 [90] | PHA, PAT | mm | ROE, OCCL, PER, ERGO |
| Doughty et al., 2022 [33] | PHA, ANI | mm | PER, MM, OCCL, CTXT, ATS |
| Frisk et al., 2022 [84] | PHA | mm | MM, ATS |
| Hu et al., 2022 [77] | PHA | mm | OCCL, PER |
| Johnson et al., 2022 [71] | PHA | mm | PER, MM, ERGO |
| Ma et al., 2022 [91] | PHA | N/A | OCCL, ERGO, EOU |
| Nguyen et al., 2022 [92] | PHA | N/A | HE, MM |
| Puladi et al., 2022 [85] | CAD | mm | MM, SPWR, PER, OCCL |
| Tu et al., 2022 [93] | PHA | mm | MM, HE, PER, ROE |
| Uhl et al., 2022 [67] | PHA | mm | MM, ATS |
| Von Atzigen et al., 2022 [76] | PHA | mm | ATS |
| Yang et al., 2022 [53] | PAT | mm | SPWR, MM |
| Zhang et al., 2022 [61] | CAD | mm | MM, ROE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Doughty, M.; Ghugre, N.R.; Wright, G.A. Augmenting Performance: A Systematic Review of Optical See-Through Head-Mounted Displays in Surgery. J. Imaging 2022, 8, 203. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8070203
AMA Style
Doughty M, Ghugre NR, Wright GA. Augmenting Performance: A Systematic Review of Optical See-Through Head-Mounted Displays in Surgery. Journal of Imaging. 2022; 8(7):203. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8070203
Chicago/Turabian StyleDoughty, Mitchell, Nilesh R. Ghugre, and Graham A. Wright. 2022. "Augmenting Performance: A Systematic Review of Optical See-Through Head-Mounted Displays in Surgery" Journal of Imaging 8, no. 7: 203. https://0-doi-org.brum.beds.ac.uk/10.3390/jimaging8070203
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.