Sandblasted and Acid Etched Titanium Dental Implant Surfaces Systematic Review and Confocal Microscopy Evaluation

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Material and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
- What are the surface characteristics of sandblasted and acid etched dental implants?
2.3. Information Sources
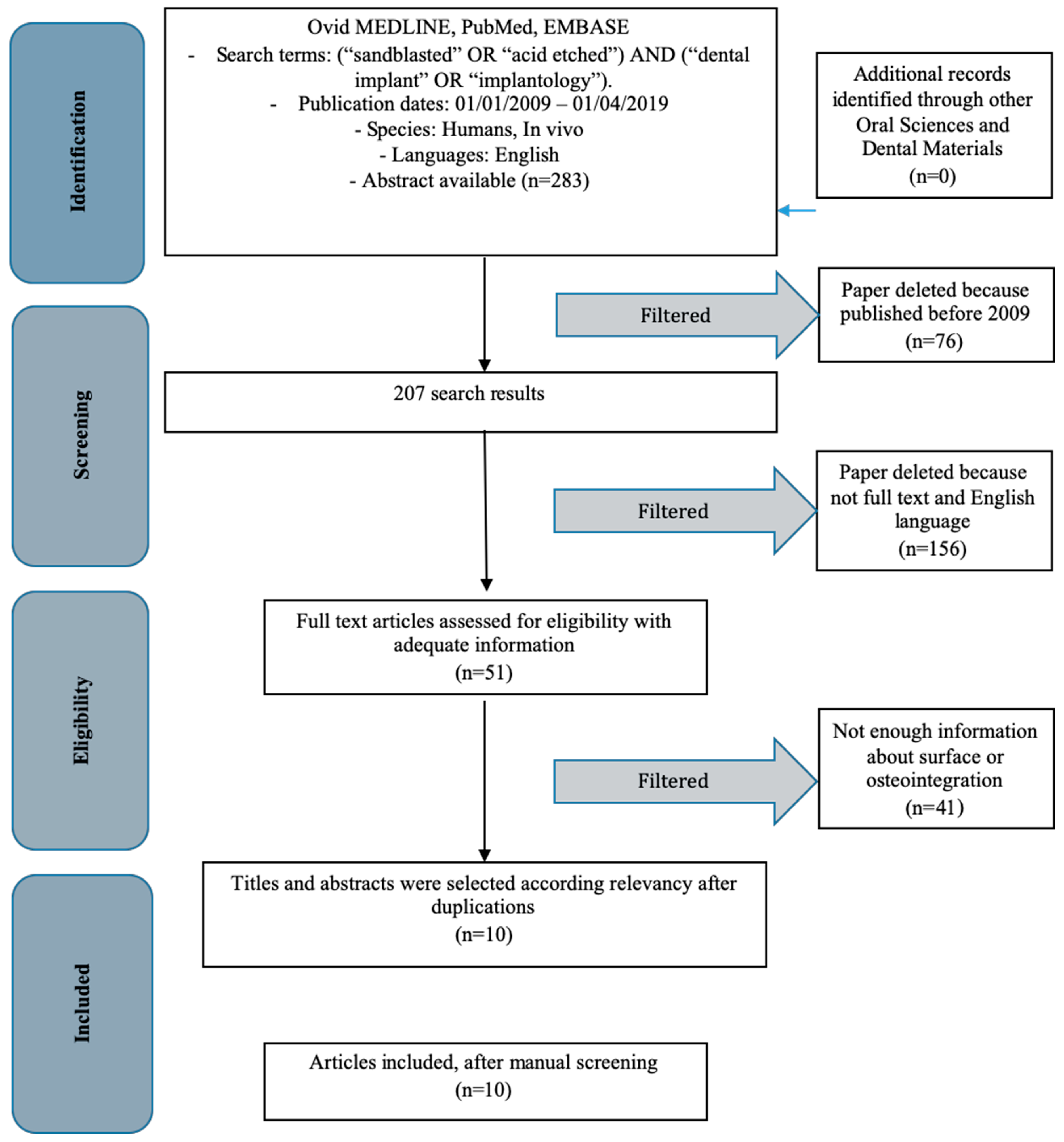
2.4. Search
- (“sandblasted” OR “acid etched”) AND (“dental implant” OR “implantology”)
2.5. Selection of Studies
2.6. Study Selection
- All randomized clinical trials about the use of SA implant surfaces on humans;
- Clinical follow up about SA implant surface use on humans; and
- All confocal studies on SA surfaces.
- Studies involving patients with other specific diseases, immunologic disorders, or other oral risk-related systemic conditions;
- Not enough information regarding the selected topic; or
- No access to the title and abstract in the English language.
2.7. Data Collection Process
- Author (Year)—Authors and year of publication;
- Sample Size—Size of sample evaluated;
- Torque—Implant positioning torque nm (Newton/meter);
- Follow up—Implant follow up period (maximum value);
- Statistic—Statistical results; and
- Type of Parameters evaluated—Evaluated parameters about the implant.
2.8. Data Items
2.9. Risk of Bias Assessment
2.10. Implantology and Different Surfaces
- Sandblasting: the bombardment of titanium surfaces with granules of variable diameter of oxides (titanium dioxide, aluminum oxide, zirconium dioxide and silicon carbide)
- Acid etching: carried out with sulfuric, hydrofluoric or hydrochloric acid according to different protocols.
- Combination of sandblasting and acid etching (SA)
- Oxidation in a galvanic bath
- Elettroerosion (EDM)
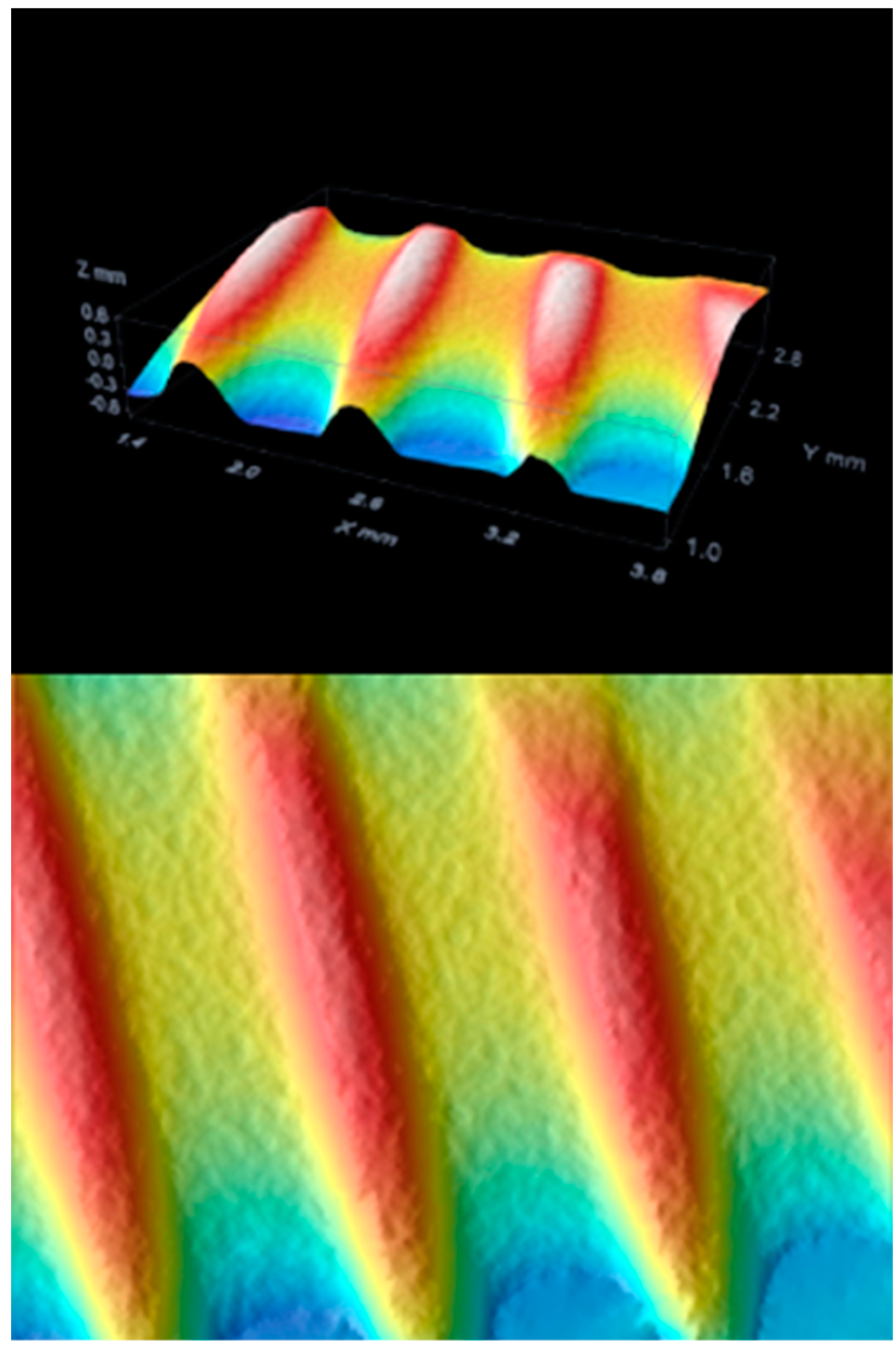
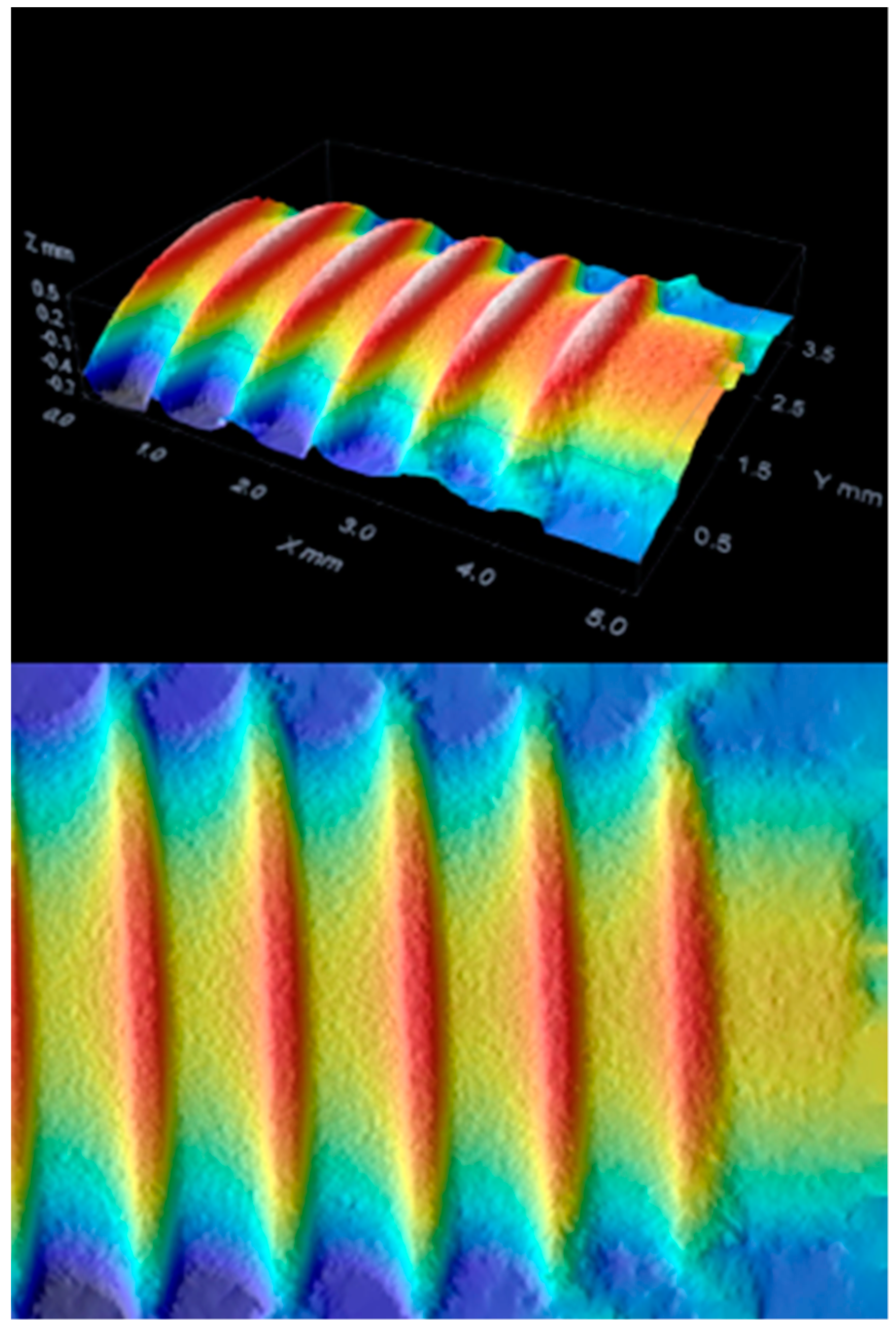
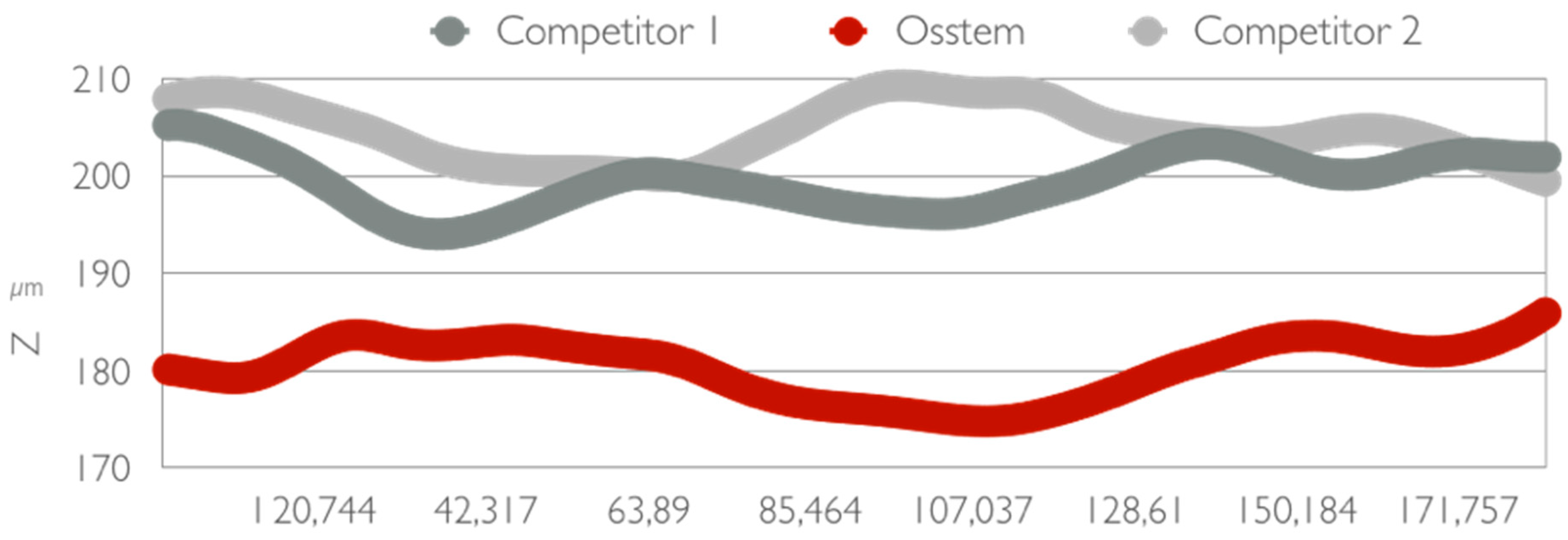
2.11. 3D Confocal Microscopy
2.12. Risk of Bias across Studies
3. Results
3.1. Inclusion Study Flow
3.2. Study Characteristics and Summary Measures
- Bone to implant contact (BIC)
- Bone Density
- Implant or prosthetic failures
- Soft tissue signs
- Histological or histomorphological evaluation
- RFA
- Region of interest (ROI) percentage
3.3. Risk of Bias within Studies
3.4. Results of Individual Studies and Synthesis of Results
3.5. Additional Analysis
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BIC | Bone to implant contact; |
| BD | Bone area; |
| ROI | Reactive oxygen species; |
| CG | Control group; |
| TG | Test group; |
| SA | Sandblasted acid etched surface; |
| MSA | Modified SA; |
| Ti | Titanium; |
| EDM | Electroerosion; |
| RFA | Radiofrequency analysis; |
| FEM | Finite Element Method. |
References
- Wirsching, K.; Lehle, K.; Jacob, P.; Gleich, O.; Strutz, J.; Kwok, P. Influence of Surface Processing on the Biocompatibility of Titanium. Materials 2011, 4, 1238–1248. [Google Scholar] [CrossRef]
- Traini, T.; Murmura, G.; Sinjari, B.; Perfetti, G.; Scarano, A.; D’Arcangelo, C.; Caputi, S. The Surface Anodization of Titanium Dental Implants Improves Blood Clot Formation Followed by Osseointegration. Coatings 2018, 8, 252. [Google Scholar] [CrossRef]
- Terada, C.; Komasa, S.; Kusumoto, T.; Kawazoe, T.; Okazaki, J. Effect of Amelogenin Coating of a Nano-Modified Titanium Surface on Bioactivity. Int. J. Mol. Sci. 2018, 19, 1274. [Google Scholar] [CrossRef]
- Di Salle, A.; Spagnuolo, G.; Conte, R.; Procino, A.; Peluso, G.; Rengo, C. Effects of various prophylactic procedures on titanium surfaces and biofilm formation. J. Periodontal Implant Sci. 2018, 48, 373–382. [Google Scholar] [CrossRef]
- Shi, X.; Xu, L.; Wang, Q.; Sunarso; Xu, L. Hydrothermal Sterilization Improves Initial Osteoblast Responses on Sandpaper-Polished Titanium. Materials 2017, 10, 812. [Google Scholar] [CrossRef]
- Mandracci, P.; Mussano, F.; Rivolo, P.; Carossa, S. Surface Treatments and Functional Coatings for Biocompatibility Improvement and Bacterial Adhesion Reduction in Dental Implantology. Coatings 2016, 6, 7. [Google Scholar] [CrossRef]
- Lan, T.H.; Pan, C.Y.; Liu, P.H.; Chou, M. Fracture Resistance of Monolithic Zirconia Crowns in Implant Prostheses in Patients with Bruxism. Materials 2019, 12, 1623. [Google Scholar] [CrossRef] [PubMed]
- De Lima Cavalcanti, J.H.; Matos, P.C.; Depes de Gouvêa, C.V.; Carvalho, W.; Calvo-Guirado, J.L.; Aragoneses, J.M.; Pérez-Díaz, L.; Gehrke, S.A. In Vitro Assessment of the Functional Dynamics of Titanium with Surface Coating of Hydroxyapatite Nanoparticles. Materials 2019, 12, 840. [Google Scholar] [CrossRef] [PubMed]
- Chiang, H.-J.; Chou, H.-H.; Ou, K.-L.; Sugiatno, E.; Ruslin, M.; Waris, R.A.; Huang, C.-F.; Liu, C.-M.; Peng, P.-W. Evaluation of Surface Characteristics and Hemocompatibility on the Oxygen Plasma-Modified Biomedical Titanium. Metals 2018, 8, 513. [Google Scholar] [CrossRef]
- Cicciu, M.; Fiorillo, L.; Herford, A.S.; Crimi, S.; Bianchi, A.; D’Amico, C.; Laino, L.; Cervino, G. Bioactive Titanium Surfaces: Interactions of Eukaryotic and Prokaryotic Cells of Nano Devices Applied to Dental Practice. Biomedicines 2019, 7, 12. [Google Scholar] [CrossRef]
- Jung, J.H.; Kim, S.Y.; Yi, Y.J.; Lee, B.K.; Kim, Y.K. Hydroxyapatite-coated implant: Clinical prognosis assessment via a retrospective follow-up study for the average of 3 years. J. Adv. Prosthodont. 2018, 10, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Kaluderovic, M.R.; Schreckenbach, J.P.; Graf, H.L. Titanium dental implant surfaces obtained by anodic spark deposition—From the past to the future. Mater. Sci Eng. C Mater. Biol. Appl. 2016, 69, 1429–1441. [Google Scholar] [CrossRef]
- Kim, S.B.; Kim, Y.K.; Kim, S.G.; Oh, J.S.; Kim, B.H. Comparative Study of the Early Loading of Resorbable Blasting Media and Sandblasting with Large-grit and Acid-etching Surface Implants: A Retrospective Cohort Study. Maxillofac. Plast Reconstr. Surg. 2014, 36, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.G.; Yun, P.Y.; Park, H.S.; Shim, J.S.; Hwang, J.W.; Kim, Y.K. Effect of loading time on the survival rate of anodic oxidized implants: Prospective multicenter study. J. Adv. Prosthodont. 2012, 4, 18–23. [Google Scholar] [CrossRef]
- Pae, A.; Kim, S.S.; Kim, H.S.; Woo, Y.H. Osteoblast-like cell attachment and proliferation on turned, blasted, and anodized titanium surfaces. Int. J. Oral Maxillofac. Implants 2011, 26, 475–481. [Google Scholar]
- Jung, S.W.; Son, M.K.; Chung, C.H.; Kim, H.J. Abrasion of abutment screw coated with TiN. J. Adv. Prosthodont 2009, 1, 102–106. [Google Scholar] [CrossRef]
- Whiting, P.; Savovic, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. Recenti Prog. Med. 2018, 109, 421–431. [Google Scholar] [CrossRef]
- Coburn, K.M.; Vevea, J.L. Publication bias as a function of study characteristics. Psychol. Methods 2015, 20, 310–330. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Mansournia, M.A.; Higgins, J.P.; Sterne, J.A.; Hernan, M.A. Biases in Randomized Trials: A Conversation Between Trialists and Epidemiologists. Epidemiology 2017, 28, 54–59. [Google Scholar] [CrossRef]
- Savovic, J.; Turner, R.M.; Mawdsley, D.; Jones, H.E.; Beynon, R.; Higgins, J.P.T.; Sterne, J.A.C. Association Between Risk-of-Bias Assessments and Results of Randomized Trials in Cochrane Reviews: The ROBES Meta-Epidemiologic Study. Am. J. Epidemiol. 2018, 187, 1113–1122. [Google Scholar] [CrossRef]
- Bachelet, V.C.; Pardo-Hernandez, H. Quality of reporting and risk of bias of randomized clinical trials published in Spanish and Latin American journals. Medwave 2019, 19, 7573. [Google Scholar] [CrossRef]
- Zielinski, R.; Kozakiewicz, M.; Swiniarski, J. Comparison of Titanium and Bioresorbable Plates in "A" Shape Plate Properties-Finite Element Analysis. Materials 2019, 12, 1110. [Google Scholar] [CrossRef]
- Szafranska, A.; Antolak-Dudka, A.; Baranowski, P.; Bogusz, P.; Zasada, D.; Malachowski, J.; Czujko, T. Identification of Mechanical Properties for Titanium Alloy Ti-6Al-4V Produced Using LENS Technology. Materials 2019, 12, 886. [Google Scholar] [CrossRef]
- Singh, G.; Pruncu, C.I.; Gupta, M.K.; Mia, M.; Khan, A.M.; Jamil, M.; Pimenov, D.Y.; Sen, B.; Sharma, V.S. Investigations of Machining Characteristics in the Upgraded MQL-Assisted Turning of Pure Titanium Alloys Using Evolutionary Algorithms. Materials 2019, 12, 999. [Google Scholar] [CrossRef]
- Li, T.; Ding, D.; Li, N. Anodic Fabrication of Ti-Ni-Si-O Nanostructures on Ti10Ni5Si Alloy. Materials 2019, 12, 1315. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Cavalcanti de Lima, J.H.; Rodriguez, F.; Calvo-Guirado, J.L.; Aramburu Junior, J.; Perez-Diaz, L.; Mazon, P.; Aragoneses, J.M.; De Aza, P.N. Microgrooves and Microrugosities in Titanium Implant Surfaces: An In Vitro and In Vivo Evaluation. Materials 2019, 12, 1287. [Google Scholar] [CrossRef]
- El-Bagoury, N.; Ahmed, S.I.; Ahmed Abu Ali, O.; El-Hadad, S.; Fallatah, A.M.; Mersal, G.A.M.; A Amin, M. The Influence of Microstructure on the Passive Layer Chemistry and Corrosion Resistance for Some Titanium-Based Alloys. Materials 2019, 12, 1233. [Google Scholar] [CrossRef]
- Mohseni, E.; Tang, W.; Wang, S. Investigation of the Role of Nano-Titanium on Corrosion and Thermal Performance of Structural Concrete with Macro-Encapsulated PCM. Molecules 2019, 24, 1360. [Google Scholar] [CrossRef]
- Soto-Penaloza, D.; Caneva, M.; Vina-Almunia, J.; Martin-de-Llano, J.J.; Penarrocha-Oltra, D.; Penarrocha-Diago, M. Bone-Healing Pattern on the Surface of Titanium Implants at Cortical and Marrow Compartments in Two Topographic Sites: An Experimental Study in Rabbits. Materials 2018, 12, 85. [Google Scholar] [CrossRef]
- Sinjari, B.; D’Addazio, G.; Bozzi, M.; Celletti, R.; Traini, T.; Mavriqi, L.; Caputi, S. Comparison of a Novel Ultrasonic Scaler Tip vs. Conventional Design on a Titanium Surface. Materials 2018, 11, 2345. [Google Scholar] [CrossRef]
- Marenzi, G.; Impero, F.; Scherillo, F.; Sammartino, J.C.; Squillace, A.; Spagnuolo, G. Effect of Different Surface Treatments on Titanium Dental Implant Micro-Morphology. Materials 2019, 12, 733. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.H.; Song, E.S.; Ju, K.W.; Lee, J.H.; Kim, M.Y.; Lim, D.; Kim, B. Finite Element Analysis of Novel Separable Fixture for Easy Retrievement in Case with Peri-Implantitis. Materials 2019, 12, 235. [Google Scholar] [CrossRef]
- Ganbold, B.; Kim, S.K.; Heo, S.J.; Koak, J.Y.; Lee, Z.H.; Cho, J. Osteoclastogenesis Behavior of Zirconia for Dental Implant. Materials 2019, 12, 732. [Google Scholar] [CrossRef]
- Cicciu, M.; Cervino, G.; Milone, D.; Risitano, G. FEM Analysis of Dental Implant-Abutment Interface Overdenture Components and Parametric Evaluation of Equator((R)) and Locator((R)) Prosthodontics Attachments. Materials 2019, 12, 592. [Google Scholar] [CrossRef] [PubMed]
- Cicciu, M.; Cervino, G.; Milone, D.; Risitano, G. FEM Investigation of the Stress Distribution over Mandibular Bone Due to Screwed Overdenture Positioned on Dental Implants. Materials 2018, 11, 1512. [Google Scholar] [CrossRef]
- Chang, J.Z.; Tsai, P.I.; Kuo, M.Y.; Sun, J.S.; Chen, S.Y.; Shen, H.H. Augmentation of DMLS Biomimetic Dental Implants with Weight-Bearing Strut to Balance of Biologic and Mechanical Demands: From Bench to Animal. Materials 2019, 12, 164. [Google Scholar] [CrossRef] [PubMed]
- Brizuela, A.; Herrero-Climent, M.; Rios-Carrasco, E.; Rios-Santos, J.V.; Perez, R.A.; Manero, J.M.; Gil Mur, J. Influence of the Elastic Modulus on the Osseointegration of Dental Implants. Materials 2019, 12, 980. [Google Scholar] [CrossRef] [PubMed]
- Bae, E.B.; Yoo, J.H.; Jeong, S.I.; Kim, M.S.; Lim, Y.M.; Ahn, J.J.; Lee, J.J.; Lee, S.H.; Kim, H.J.; Huh, J.B. Effect of Titanium Implants Coated with Radiation-Crosslinked Collagen on Stability and Osseointegration in Rat Tibia. Materials 2018, 11, 2520. [Google Scholar] [CrossRef]
- Alsaeedi, R.; Ozdemir, Z. Evaluation of Chemical Mechanical Polishing-Based Surface Modification on 3D Dental Implants Compared to Alternative Methods. Materials 2018, 11, 2286. [Google Scholar] [CrossRef]
- Shemtov-Yona, K.; Rittel, D. Fatigue of Dental Implants: Facts and Fallacies. Dent. J. 2016, 4, 16. [Google Scholar] [CrossRef]
- Rahmitasari, F.; Ishida, Y.; Kurahashi, K.; Matsuda, T.; Watanabe, M.; Ichikawa, T. PEEK with Reinforced Materials and Modifications for Dental Implant Applications. Dent. J. 2017, 5, 35. [Google Scholar] [CrossRef]
- Nejem Wakim, R.; Namour, M.; Nguyen, H.V.; Peremans, A.; Zeinoun, T.; Vanheusden, A.; Rompen, E.; Nammour, S. Decontamination of Dental Implant Surfaces by the Er:YAG Laser Beam: A Comparative in Vitro Study of Various Protocols. Dent. J. 2018, 6, 66. [Google Scholar] [CrossRef]
- Cao, X.-Y.; Tian, N.; Dong, X.; Cheng, C.-K. Implant Coating Manufactured by Micro-Arc Oxidation and Dip Coating in Resorbable Polylactide for Antimicrobial Applications in Orthopedics. Coatings 2019, 9, 284. [Google Scholar] [CrossRef]
- Variola, F.; Brunski, J.B.; Orsini, G.; Tambasco de Oliveira, P.; Wazen, R.; Nanci, A. Nanoscale surface modifications of medically relevant metals: State-of-the art and perspectives. Nanoscale 2011, 3, 335–353. [Google Scholar] [CrossRef]
- Wazen, R.M.; Currey, J.A.; Guo, H.; Brunski, J.B.; Helms, J.A.; Nanci, A. Micromotion-induced strain fields influence early stages of repair at bone-implant interfaces. Acta Biomater. 2013, 9, 6663–6674. [Google Scholar] [CrossRef]
- Guadarrama Bello, D.; Fouillen, A.; Badia, A.; Nanci, A. A nanoporous titanium surface promotes the maturation of focal adhesions and formation of filopodia with distinctive nanoscale protrusions by osteogenic cells. Acta Biomater. 2017, 60, 339–349. [Google Scholar] [CrossRef]
- Rodriguez-Contreras, A.; Guadarrama Bello, D.; Flynn, S.; Variola, F.; Wuest, J.D.; Nanci, A. Chemical nanocavitation of surfaces to enhance the utility of stainless steel as a medical material. Colloids Surf. B Biointerfaces 2018, 161, 677–687. [Google Scholar] [CrossRef]
- Bueno Rde, B.; Adachi, P.; Castro-Raucci, L.M.; Rosa, A.L.; Nanci, A.; Oliveira, P.T. Oxidative nanopatterning of titanium surfaces promotes production and extracellular accumulation of osteopontin. Braz. Dent. J. 2011, 22, 179–184. [Google Scholar] [CrossRef]
- Maia, L.P.; Reino, D.M.; Muglia, V.A.; Almeida, A.L.; Nanci, A.; Wazen, R.M.; de Oliveira, P.T.; Palioto, D.B.; Novaes, A.B., Jr. Influence of periodontal tissue thickness on buccal plate remodelling on immediate implants with xenograft. J. Clin. Periodontol. 2015, 42, 590–598. [Google Scholar] [CrossRef]
- Variola, F.; Zalzal, S.F.; Leduc, A.; Barbeau, J.; Nanci, A. Oxidative nanopatterning of titanium generates mesoporous surfaces with antimicrobial properties. Int. J. Nanomedicine 2014, 9, 2319–2325. [Google Scholar] [CrossRef]
- Ariganello, M.B.; Guadarrama Bello, D.; Rodriguez-Contreras, A.; Sadeghi, S.; Isola, G.; Variola, F.; Nanci, A. Surface nanocavitation of titanium modulates macrophage activity. Int. J. Nanomedicine 2018, 13, 8297–8308. [Google Scholar] [CrossRef]
- Maturi, F.E.; Sabio, R.M.; Silva, R.R.; Lahoud, M.G.; Meneguin, A.B.; Valente, G.T.; Caface, R.A.; Leite, I.S.; Inada, N.M.; Ribeiro, S.J.L. Luminescent Mesoporous Silica Nanohybrid Based on Drug Derivative Terbium Complex. Materials 2019, 12, 933. [Google Scholar] [CrossRef]
- Garcia, J.C.; Sanz Lobera, A.; Maresca, P.; Pareja, T.F.; Wang, C. Some Considerations about the Use of Contact and Confocal Microscopy Methods in Surface Texture Measurement. Materials 2018, 11, 1484. [Google Scholar] [CrossRef]
- Schmitt, C.M.; Koepple, M.; Moest, T.; Neumann, K.; Weisel, T.; Schlegel, K.A. In vivo evaluation of biofunctionalized implant surfaces with a synthetic peptide (P-15) and its impact on osseointegration. A preclinical animal study. Clin. Oral Implants Res. 2016, 27, 1339–1348. [Google Scholar] [CrossRef]
- Novellino, M.M.; Sesma, N.; Zanardi, P.R.; Lagana, D.C. Resonance frequency analysis of dental implants placed at the posterior maxilla varying the surface treatment only: A randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 770–775. [Google Scholar] [CrossRef] [Green Version]
- Mangano, C.; Shibli, J.A.; Pires, J.T.; Luongo, G.; Piattelli, A.; Iezzi, G. Early Bone Formation around Immediately Loaded Transitional Implants Inserted in the Human Posterior Maxilla: The Effects of Fixture Design and Surface. BioMed Res. Int. 2017, 2017, 4152506. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Felice, P.; Loi, I.; Viola, P.; Ferri, V.; Leone, M.; Esposito, M. Machined versus roughened immediately loaded and finally restored single implants inserted flapless: Preliminary 6-month data from a split- mouth randomised controlled trial. Eur. J. Oral Implantol. 2016, 9, 155–163. [Google Scholar]
- Schwarz, F.; Mihatovic, I.; Becker, J.; Bormann, K.H.; Keeve, P.L.; Friedmann, A. Histological evaluation of different abutments in the posterior maxilla and mandible: An experimental study in humans. J. Clin. Periodontol. 2013, 40, 807–815. [Google Scholar] [CrossRef]
- Corvino, V.; Iezzi, G.; Trubiani, O.; Traini, T.; Piattelli, M. Histological and histomorphometric evaluation of implant with nanometer scale and oxidized surface. In vitro and in vivo study. J. Biol. Regul. Homeost. Agents 2012, 26, 19–28. [Google Scholar]
- Karabuda, Z.C.; Abdel-Haq J Fau - Arisan, V.; Arisan, V. Stability, marginal bone loss and survival of standard and modified sand-blasted, acid-etched implants in bilateral edentulous spaces: A prospective 15-month evaluation. Clin. Oral. Implants Res. 2011, 22, 840–849. [Google Scholar] [CrossRef]
- D’Avila, S.; Dos Reis, L.D.; Piattelli, A.; Aguiar, K.C.; De Faveri, M.; Borges, F.L.; Shibli, J.A. Impact of smoking on human bone apposition at different dental implant surfaces: A histologic study in type IV bone. J. Oral Implantol. 2010, 36, 85–90. [Google Scholar] [CrossRef]
- Shibli, J.A.; Grassi, S.; Piattelli, A.; Pecora, G.E.; Ferrari, D.S.; Onuma, T.; Iezzi, G. Histomorphometric evaluation of bioceramic molecular impregnated and dual acid-etched implant surfaces in the human posterior maxilla. Clin. Implant. Dent. Relat. Res. 2012, 12, 281–288. [Google Scholar] [CrossRef]
- Khang, W.; Feldman, S.; Hawley, C.E.; Gunsolley, J. A multi-center study comparing dual acid-etched and machined-surfaced implants in various bone qualities. J. Periodontol. 2001, 72, 1384–1390. [Google Scholar] [CrossRef]
- Menezes, H.H.M.; Naves, M.M.; Costa, H.L.; Barbosa, T.P.; Ferreira, J.A.; Magalhães, D.; Martinez, E.F. Effect of Surgical Installation of Dental Implants on Surface Topography and Its Influence on Osteoblast Proliferation. Int. J. Dent. 2018, 2018, 4089274. [Google Scholar] [CrossRef]
- Kim, Y.K.; Kim, B.S.; Yun, P.Y.; Mun, S.U.; Yi, Y.J.; Kim, S.G.; Jeong, K.I. The seven-year cumulative survival rate of Osstem implants. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Jeong, M.A.; Kim, S.G.; Kim, Y.K.; Oh, H.K.; Cho, Y.S.; Kim, W.C.; Oh, J.S. A multicenter prospective study in type IV bone of a single type of implant. Implant. Dent. 2012, 21, 330–334. [Google Scholar] [CrossRef]
- Kim, Y.K.; Lee, J.H.; Lee, J.Y.; Yi, Y.J. A randomized controlled clinical trial of two types of tapered implants on immediate loading in the posterior maxilla and mandible. Int J. Oral Maxillofac Implants 2013, 28, 1602–1611. [Google Scholar] [CrossRef]
- Kim, Y.K.; Ahn, K.J.; Yun, P.Y.; Kim, M.; Yang, H.S.; Yi, Y.J.; Bae, J.H. Effect of loading time on marginal bone loss around hydroxyapatite-coated implants. J. Korean Assoc. Oral Maxillofac Surg 2013, 39, 161–167. [Google Scholar] [CrossRef]
- Osman, M.S.; Ziada, H.M.; Abubakr, N.H.; Suliman, A.M. Implant impression accuracy of parallel and non-parallel implants: A comparative in-vitro analysis of open and closed tray techniques. Int J. Implant. Dent. 2019, 5, 4. [Google Scholar] [CrossRef]
- Tallarico, M.; Caneva, M.; Baldini, N.; Gatti, F.; Duvina, M.; Billi, M.; Iannello, G.; Piacentini, G.; Meloni, S.M.; Cicciu, M. Patient-centered rehabilitation of single, partial, and complete edentulism with cemented- or screw-retained fixed dental prosthesis: The First Osstem Advanced Dental Implant Research and Education Center Consensus Conference 2017. Eur J. Dent. 2018, 12, 617–626. [Google Scholar]
- Tallarico, M.; Xhanari, E.; Pisano, M.; Gatti, F.; Meloni, S.M. Molar replacement with 7 mm-wide diameter implants: To place the implant immediately or to wait 4 months after socket preservation? 1 year after loading results from a randomised controlled trial. Eur J. Oral Implantol. 2017, 10, 169–178. [Google Scholar]
- Tallarico, M.; Xhanari, E.; Pisano, M.; De Riu, G.; Tullio, A.; Meloni, S.M. Single post-extractive ultra-wide 7 mm-diameter implants versus implants placed in molar healed sites after socket preservation for molar replacement: 6-month post-loading results from a randomised controlled trial. Eur J. Oral Implantol. 2016, 9, 263–275. [Google Scholar]
- Sui, X.; Wei, H.; Wang, D.; Han, Y.; Deng, J.; Wang, Y.; Wang, J.; Yang, J. Experimental research on the relationship between fit accuracy and fracture resistance of zirconia abutments. J. Dent. 2014, 42, 1353–1359. [Google Scholar] [CrossRef]
- Jo, J.Y.; Yang, D.S.; Huh, J.B.; Heo, J.C.; Yun, M.J.; Jeong, C.M. Influence of abutment materials on the implant-abutment joint stability in internal conical connection type implant systems. J. Adv. Prosthodont 2014, 6, 491–497. [Google Scholar] [CrossRef]
- Yang, J.; Wang, K.; Liu, G.; Wang, D. Fracture resistance of inter-joined zirconia abutment of dental implant system with injection molding technique. Clin. Oral Implants Res. 2013, 24, 1247–1250. [Google Scholar] [CrossRef]
- Huang, J.S.; Zhao, J.J.; Liu, Q.; Liu, T.T. Clinical research of immediate restoration implant with mini-implants in edentulous space. Hua Xi Kou Qiang Yi Xue Za Zhi 2010, 28, 412–416. [Google Scholar]
- Jo, S.H.; Kim, K.I.; Seo, J.M.; Song, K.Y.; Park, J.M.; Ahn, S.G. Effect of impression coping and implant angulation on the accuracy of implant impressions: An in vitro study. J. Adv. Prosthodont 2010, 2, 128–133. [Google Scholar] [CrossRef]
- Park, Y.H.; Jung, U.W.; Kim, C.S.; Choi, S.H.; Cho, K.S.; Lee, J.S. Resonance Frequency Analysis of Tapered Implants Placed at Maxillary Posterior Sites After Lateral Sinus Augmentation: A 1.5-year Follow-Up Prospective Study. Implant. Dent. 2019, 28, 62–67. [Google Scholar] [CrossRef]
- Yassin Alsabbagh, A.; Alsabbagh, M.M.; Darjazini Nahas, B.; Rajih, S. Comparison of three different methods of internal sinus lifting for elevation heights of 7 mm: An ex vivo study. Int J. Implant. Dent. 2017, 3, 40. [Google Scholar] [CrossRef]
- Kim, Y.K.; Yun, P.Y.; Kim, S.G.; Kim, B.S.; Ong, J.L. Evaluation of sinus bone resorption and marginal bone loss after sinus bone grafting and implant placement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2009, 107, 21–28. [Google Scholar] [CrossRef]
- Kim, Y.K.; Kim, S.G.; Park, J.Y.; Yi, Y.J.; Bae, J.H. Comparison of clinical outcomes of sinus bone graft with simultaneous implant placement: 4-month and 6-month final prosthetic loading. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2011, 111, 164–169. [Google Scholar] [CrossRef]
- Yoo, J.M.; Ben Amara, H.; Kim, M.K.; Song, J.D.; Koo, K.T. Oral tissue response to soft tissue expanders prior to bone augmentation: In vitro analysis and histological study in dogs. J. Periodontal Implant Sci. 2018, 48, 152–163. [Google Scholar] [CrossRef]
- Kim, S.K.; Kim, S.W.; Kim, K.W. Effect on bone formation of the autogenous tooth graft in the treatment of peri-implant vertical bone defects in the minipigs. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 2. [Google Scholar] [CrossRef]
- Kang, E.J.; Kim, S.K.; Eom, T.G.; Choi, K.O.; Lee, T.H. Evaluation of the osteogenic activity of the BMP-2 mimetic peptide, PEP7, in vitro and in vivo. Int. J. Oral Maxillofac. Implants 2013, 28, 749–756. [Google Scholar] [CrossRef]
- Oliver, R. Flapless dental implant surgery may improve hard and soft tissue outcomes. J. Evid. Based Dent. Pract. 2012, 12, 87–88. [Google Scholar] [CrossRef]
- Li, Z.R.; Liu, Z.H.; Xu, S.; Xiao, H.J.; Zhou, W.J. The application of guided bone regeneration technique in the restoration of maxillary lateral incisor with bone defect. Shanghai Kou Qiang Yi Xue 2012, 21, 190–193. [Google Scholar]
- Huang, H.; Xu, Z.; Shao, X.; Wismeijer, D.; Sun, P.; Wang, J.; Wu, G. Multivariate linear regression analysis to identify general factors for quantitative predictions of implant stability quotient values. PLoS ONE 2017, 12, e0187010. [Google Scholar] [CrossRef]
- Eom, T.G.; Kim, H.W.; Jeon, G.R.; Yun, M.J.; Huh, J.B.; Jeong, C.M. Effects of Different Implant Osteotomy Preparation Sizes on Implant Stability and Bone Response in the Minipig Mandible. Int J. Oral Maxillofac. Implants 2016, 31, 997–1006. [Google Scholar] [CrossRef]
- Park, J.C.; Ha, S.R.; Kim, S.M.; Kim, M.J.; Lee, J.B.; Lee, J.H. A randomized clinical 1-year trial comparing two types of non-submerged dental implants. Clin. Oral Implants Res. 2010, 21, 228–236. [Google Scholar] [CrossRef]
- Hong, J.; Lim, Y.J.; Park, S.O. Quantitative biomechanical analysis of the influence of the cortical bone and implant length on primary stability. Clin. Oral Implants Res. 2012, 23, 1193–1197. [Google Scholar] [CrossRef]
- Bansal, J.; Kedige, S.; Bansal, A.; Anand, S. A relaxed implant bed: Implants placed after two weeks of osteotomy with immediate loading: A one year clinical trial. J. Oral Implantol. 2012, 38, 155–164. [Google Scholar] [CrossRef]
- Cervino, G.; Romeo, U.; Lauritano, F.; Bramanti, E.; Fiorillo, L.; D’Amico, C.; Milone, D.; Laino, L.; Campolongo, F.; Rapisarda, S.; et al. Fem and Von Mises Analysis of OSSTEM (r) Dental Implant Structural Components: Evaluation of Different Direction Dynamic Loads. Open Dent. J. 2018, 12, 219–229. [Google Scholar] [CrossRef]
- Herekar, M.; Sethi, M.; Prithviraj, D.R.; Bhat, K.; Fernandes, A.; Patil, V. A Clinical Study Evaluating Changes in the Microbial Flora Around Dental Implants During Various Stages of Implant Restoration. Implant. Dent. 2015, 24, 527–532. [Google Scholar] [CrossRef]
- Kim, J.R.; Kim, S.H.; Kim, I.R.; Park, B.S.; Kim, Y.D. Low-level laser therapy affects osseointegration in titanium implants: Resonance frequency, removal torque, and histomorphometric analysis in rabbits. J. Korean Assoc. Oral Maxillofac. Surg. 2016, 42, 2–8. [Google Scholar] [CrossRef]
- Namgoong, H.; Kim, M.D.; Ku, Y.; Rhyu, I.C.; Lee, Y.M.; Seol, Y.J.; Gu, H.J.; Susin, C.; Wikesjo, U.M.; Koo, K.T. Bone reconstruction after surgical treatment of experimental peri-implantitis defects at a sandblasted/acid-etched hydroxyapatite-coated implant: An experimental study in the dog. J. Clin. Periodontol. 2015, 42, 960–966. [Google Scholar] [CrossRef]
- Jeon, W.J.; Kim, S.G.; Lim, S.C.; Ong, J.L.; Oh, D.S. Histomorphometric evaluation of immediately loaded SSII implants of different surface treatments in a dog model. J. Biomed. Mater. Res. A 2009, 90, 396–400. [Google Scholar] [CrossRef]
- Moon, S.Y.; Kim, S.G.; Lim, S.C.; Ong, J.L. Histologic and histomorphometric evaluation of early and immediately loaded implants in the dog mandible. J. Biomed. Mater. Res. A 2008, 86, 1122–1127. [Google Scholar] [CrossRef]
- Duncan, W.J.; Lee, M.H.; Dovban, A.S.; Hendra, N.; Ershadi, S.; Rumende, H. Anodization increases early integration of Osstem implants in sheep femurs. Ann. R. Australas. Coll. Dent. Surg. 2008, 19, 152–156. [Google Scholar]
- Bramanti, E.; Cervino, G.; Lauritano, F.; Fiorillo, L.; D’Amico, C.; Sambataro, S.; Denaro, D.; Fama, F.; Ierardo, G.; Polimeni, A.; et al. FEM and Von Mises Analysis on Prosthetic Crowns Structural Elements: Evaluation of Different Applied Materials. Sci. World J. 2017, 2017, 1029574. [Google Scholar] [CrossRef]
- Cicciu, M.; Bramanti, E.; Matacena, G.; Guglielmino, E.; Risitano, G. FEM evaluation of cemented-retained versus screw-retained dental implant single-tooth crown prosthesis. Int. J. Clin. Exp. Med. 2014, 7, 817–825. [Google Scholar] [PubMed]
- Cicciù, M.; Cervino, G.; Bramanti, E.; Lauritano, F.; Gudice, G.L.; Scappaticci, L.; Rapparini, A.; Guglielmino, E.; Risitano, G. FEM analysis of mandibular prosthetic overdenture supported by dental implants: Evaluation of different retention methods. Comput. Math. Methods Med. 2015, 2015, 943839. [Google Scholar]
- Cicciu, M.; Cervino, G.; Herford, A.S.; Fama, F.; Bramanti, E.; Fiorillo, L.; Lauritano, F.; Sambataro, S.; Troiano, G.; Laino, L. Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review. Mar. Drugs 2018, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Maridati, P.; Stoffella, E.; Speroni, S.; Cicciu, M.; Maiorana, C. Alveolar antral artery isolation during sinus lift procedure with the double window technique. Open Dent. J. 2014, 8, 95–103. [Google Scholar] [CrossRef]
- Beretta, M.; Cicciù, M.; Bramanti, E.; Maiorana, C. Schneider membrane elevation in presence of sinus septa: Anatomic features and surgical management. Int. J. Dent. 2012, 2012, 261905. [Google Scholar] [CrossRef]
- Rancitelli, D.; Borgonovo, A.E.; Cicciù, M.; Re, D.; Rizza, F.; Frigo, A.C.; Maiorana, C. Maxillary sinus septa and anatomic correlation with the Schneiderian membrane. J. Craniofac. Surg. 2015, 26, 1394–1398. [Google Scholar] [CrossRef]
- Poli, P.P.; Beretta, M.; Cicciù, M.; Maiorana, C. Alveolar ridge augmentation with titanium mesh. A retrospective clinical study. Open Dent. J. 2014, 8, 148–158. [Google Scholar] [CrossRef]
- Lo Giudice, G.; Iannello, G.; Terranova, A.; Lo Giudice, R.; Pantaleo, G.; Cicciù, M. Transcrestal sinus lift procedure approaching atrophic maxillary ridge: A 60-month clinical and radiological follow-up evaluation. Int. J. Dent. 2015, 2015, 261652. [Google Scholar] [CrossRef]
- Herford, A.S.; Cicciù, M.; Eftimie, L.F.; Miller, M.; Signorino, F.; Famà, F.; Cervino, G.; Lo Giudice, G.; Bramanti, E.; Lauritano, F.; et al. rhBMP-2 applied as support of distraction osteogenesis: A split-mouth histological study over nonhuman primates mandibles. Int. J. Clin. Exp. Med. 2016, 9, 17187–17194. [Google Scholar]
- Crimi, S.; Fiorillo, L.; Bianchi, A.; D’Amico, C.; Amoroso, G.; Gorassini, F.; Mastroieni, R.; Marino, S.; Scoglio, C.; Catalano, F.; et al. Herpes Virus, Oral Clinical Signs and QoL: Systematic Review of Recent Data. Viruses 2019, 11, 463. [Google Scholar] [CrossRef]
- Lo Giudice, G.; Cutroneo, G.; Centofanti, A.; Artemisia, A.; Bramanti, E.; Militi, A.; Cicciù, M. Dentin morphology of root canal surface: A quantitative evaluation based on a scanning electronic microscopy study. Biomed. Res. Int. 2015, 2015, 164065. [Google Scholar] [CrossRef]
- De Jesus, R.N.R.; Carrilho, E.; Antunes, P.V.; Ramalho, A.; Moura, C.C.G.; Stavropoulos, A.; Zanetta-Barbosa, D. Interfacial biomechanical properties of a dual acid-etched versus a chemically modified hydrophilic dual acid-etched implant surface: An experimental study in Beagles. Int J. Implant. Dent. 2018, 4, 28. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Romeo, U.; Bianchi, A.; Crimi, S.; Laino, L. Molecular Biomarkers Related to Oral Carcinoma: Clinical Trial Outcome Evaluation in a Literature Review. Dis. Markers 2019, 2019, 11. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Laino, L.; Herford, A.S.; Lauritano, F.; Giudice, G.L.; Fama, F.; Santoro, R.; Troiano, G.; Iannello, G.; et al. Oral Health Impact Profile in Celiac Patients: Analysis of Recent Findings in a Literature Review. Gastroenterol. Res. Pract. 2018, 2018, 7848735. [Google Scholar] [CrossRef]
- Laino, L.; Cicciù, M.; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Surgical Risk on Patients with Coagulopathies: Guidelines on Hemophiliac Patients for Oro-Maxillofacial Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1386. [Google Scholar] [CrossRef]
- Fiorillo, L.; De Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Campagna, P.; Herford, A.S.; Laino, L.; Cicciù, M. Oral and Psychological Alterations in Haemophiliac Patients. Biomedicines 2019, 7, 33. [Google Scholar] [CrossRef]
- Cervino, G.; Terranova, A.; Briguglio, F.; De Stefano, R.; Famà, F.; D’Amico, C.; Amoroso, G.; Marino, S.; Gorassini, F.; Mastroieni, R.; et al. Diabetes: Oral health related quality of life and oral alterations. BioMed Res. Int. 2019, 2019, 5907195. [Google Scholar] [CrossRef]
- Ghadimi, K.; Levy, J.H.; Welsby, I.J. Perioperative management of the bleeding patient. Br. J. Anaesth. 2016, 117, 18–30. [Google Scholar] [CrossRef]
- Simurda, T.; Stanciakova, L.; Stasko, J.; Dobrotova, M.; Kubisz, P. Yes or no for secondary prophylaxis in afibrinogenemia? Blood Coagul. Fibrinolysis 2015, 26, 978–980. [Google Scholar] [CrossRef]
- Williams, B.; Indresano, A.T.; O’Ryan, F. Venous thromboembolism in oral and maxillofacial surgery: A review of the literature. J. Oral maxillof. Surg. 2011, 69, 840–844. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Monte, I.P.; De Stefano, R.; Laino, L.; Crimi, S.; Bianchi, A.; Herford, A.S.; Biondi, A.; Cicciù, M. Advances in Antiplatelet Therapy for Dentofacial Surgery Patients: Focus on Past and Present Strategies. Materials 2019, 12, 1524. [Google Scholar] [CrossRef]
- Rullo, R.; Scalzone, P.; Laino, L.; Russo, A.; Festa, V.M.; Fiorillo, L.; Cicciu, M. Solitary Plasmacytoma of the Mandible: Early Diagnosis and Surgical Management. J. Craniofac. Surg. 2019. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Matarese, G.; Ramaglia, L.; Fiorillo, L.; Cervino, G.; Lauritano, F.; Isola, G. Implantology and Periodontal Disease: The Panacea to Problem Solving? Open Dent. J. 2017, 11, 460–465. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cervino, G.; Herford, A.; Lauritano, F.; D’Amico, C.; Lo Giudice, R.; Cicciù, M. Interferon Crevicular Fluid Profile and Correlation with Periodontal Disease and Wound Healing: A Systemic Review of Recent Data. Int J. Mol. Sci 2018, 19, 1908. [Google Scholar] [CrossRef]
- Troiano, G.; Laino, L.; Cicciu, M.; Cervino, G.; Fiorillo, L.; D’Amico, C.; Zhurakivska, K.; Lo Muzio, L. Comparison of Two Routes of Administration of Dexamethasone to Reduce the Postoperative Sequelae After Third Molar Surgery: A Systematic Review and Meta-Analysis. Open Dent. J. 2018, 12, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Lo Giudice, R.; Puleio, F.; Rizzo, D.; Alibrandi, A.; Lo Giudice, G.; Centofanti, A.; Fiorillo, L.; Di Mauro, D.; Nicita, F. Comparative investigation of cutting devices on bone blocks: An SEM morphological analysis. Appl. Sci. 2019, 9, 1908. [Google Scholar] [CrossRef]
- Cervino, G.; Cicciù, M.; Biondi, A.; Bocchieri, S.; Herford, A.S.; Laino, L.; Fiorillo, L. Antibiotic Prophylaxis on Third Molar Extraction: Systematic Review of Recent Data. Antibiotics 2019, 8, 53. [Google Scholar] [CrossRef]
- Stacchi, C.; Berton, F.; Fiorillo, L.; Nicolin, V.; Lombardi, T.; Cicciù, M.; Di Lenarda, R. Fresh frozen allogeneic bone block in maxillary sinus floor elevation: Histomorphometric analysis of a bone specimen retrieved 15 years after grafting procedure. Appl. Sci. 2019, 9, 1119. [Google Scholar] [CrossRef]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Camurri Piloni, A.; Fiorillo, L.; Di Lenarda, R.; Stacchi, C. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. Biomed. Res. Int. 2018, 2018, 9352130. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Arzukanyan, A.V.; Spagnuolo, G.; Cicciu, M. Dental Restorative Digital Workflow: Digital Smile Design from Aesthetic to Function. Dent. J. 2019, 7, 30. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Herford, A.; Laino, L.; Troiano, G.; Amoroso, G.; Cicciù, M. Alginate Materials and Dental Impression Technique: A Current State of the Art and Application to Dental Practice. Mar. Drugs 2018, 17, 18. [Google Scholar] [CrossRef]
- Cervino, G.; Fiorillo, L.; Spagnuolo, G.; Bramanti, E.; Laino, L.; Lauritano, F.; Cicciù, M. Interface between MTA and Dental Bonding Agents: Scanning Electron Microscope Evaluation. J. Int Soc. Prev. Community Dent. 2017, 7, 64–68. [Google Scholar]
- Isola, G.; Ramaglia, L.; Cordasco, G.; Lucchese, A.; Fiorillo, L.; Matarese, G. The effect of a functional appliance in the management of temporomandibular joint disorders in patients with juvenile idiopathic arthritis. Minerva Stomatol. 2017, 66, 1–8. [Google Scholar]
- Isola, G.; Cicciu, M.; Fiorillo, L.; Matarese, G. Association Between Odontoma and Impacted Teeth. J. Craniofac. Surg. 2017, 28, 755–758. [Google Scholar] [CrossRef]
- Bramanti, E.; Matacena, G.; Cecchetti, F.; Arcuri, C.; Cicciù, M. Oral health-related quality of life in partially edentulous patients before and after implant therapy: A 2-year longitudinal study. ORAL Implantol. 2013, 6, 37–42. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Sample Size | Torque | Follow up | Statistic | Type of Parameters Evaluated | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| RFA Evaluation | Histologic | Histomophometric | Prothestic Failures | Implant Failures | In Vitro | |||||
| Novellino et al. (2017) [56] | 21 | 35.125 ± 4.498 | 1 y | p < 0.01 | CG: 42–81 SA | |||||
| TG: 32.5–82.5 MSA | ||||||||||
| Mangano et al. (2017) [57] | 10 | Not significant | ✔ | TG: BIC 35.9% BD 31.8 | ||||||
| CG: BIC 29.9% BD 32.5% | ||||||||||
| Schmitt et al. (2015) [55] | 10 | BIC 0.002; | ✔ | Machined | ||||||
| SA | ||||||||||
| Hydroxyapatite surface | ||||||||||
| Cannizzaro et al. (2016) [58] | 50 | >50 | 6 m | Not significant | ✔ | ✔ | ||||
| Schwarz et al. (2013) [59] | 30 | 8 w | p < 0.05 | ✔ | ||||||
| Corvino et al. (2012) [60] | 15 | 2 m | BIC p = 0.028 | ✔ | ✔ | ✔ | ||||
| Karabuda et al. (2010) [61] | 22 | CG: 25.48 | 6 w | p < 0.05 | CG: 58.21 | ✔ | ✔ | |||
| TG: 23.75 | TG: 58.15 | |||||||||
| D’Avila et al. (2010) [62] | 7 | 2 m | BIC significant | Machined: BIC 10.40% | ✔ | |||||
| Sandblasted: BIC 22.19% | ||||||||||
| Shibli et al. (2010) [63] | 10 | 2 m | BIC p < 0.05;BA not significant | ✔ | ✔ | ✔ | ||||
| Khang et al. (2001) [64] | 97 | 6 m | ✔ | ✔ | ||||||
| Osstem SA® (Seoul, South Korea) Surface Field of Study | References |
|---|---|
| Implant survival rate | [66,67] |
| Implant surface | [11,12,13,14,15,16] |
| Implant loading time | [68,69] |
| Prosthetic study | [70,71,72,73,74,75,76,77,78] |
| Maxillary sinus lifts and implant | [79,80,81,82] |
| Bone augmentation and implant | [83,84,85,86,87] |
| Implant stability | [88,89,90,91,92] |
| FEM on implant components | [93] |
| Microbial flora on implant | [94] |
| Implant studies on animals | [95,96,97,98,99] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cervino, G.; Fiorillo, L.; Iannello, G.; Santonocito, D.; Risitano, G.; Cicciù, M. Sandblasted and Acid Etched Titanium Dental Implant Surfaces Systematic Review and Confocal Microscopy Evaluation. Materials 2019, 12, 1763. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12111763
Cervino G, Fiorillo L, Iannello G, Santonocito D, Risitano G, Cicciù M. Sandblasted and Acid Etched Titanium Dental Implant Surfaces Systematic Review and Confocal Microscopy Evaluation. Materials. 2019; 12(11):1763. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12111763
Chicago/Turabian StyleCervino, Gabriele, Luca Fiorillo, Gaetano Iannello, Dario Santonocito, Giacomo Risitano, and Marco Cicciù. 2019. "Sandblasted and Acid Etched Titanium Dental Implant Surfaces Systematic Review and Confocal Microscopy Evaluation" Materials 12, no. 11: 1763. https://0-doi-org.brum.beds.ac.uk/10.3390/ma12111763