
Peri-Implant Repair Using a Modified Implant Macrogeometry in Diabetic Rats: Biomechanical and Molecular Analyses of Bone-Related Markers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
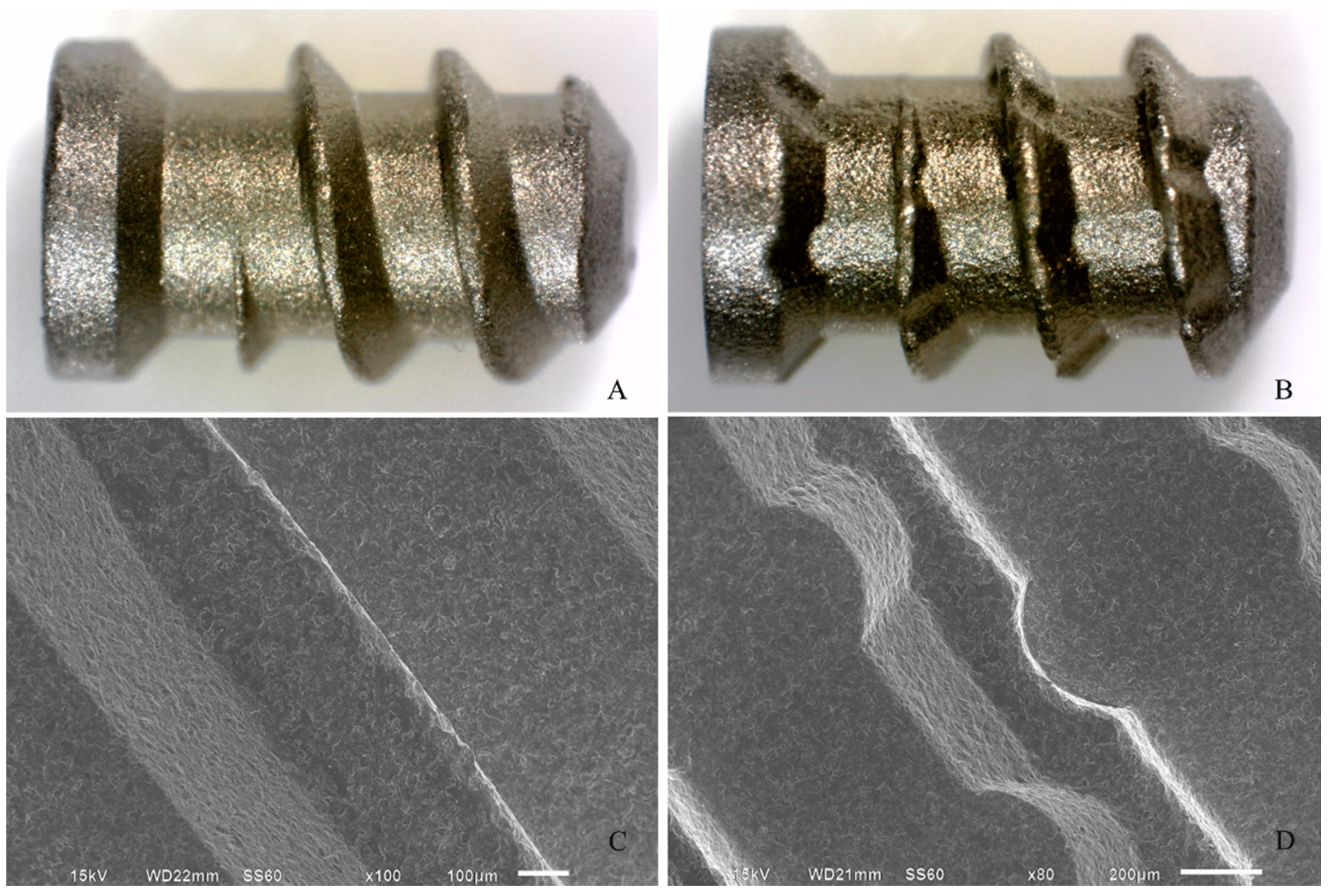
2.2. Treatment Groups
2.3. DM Induction
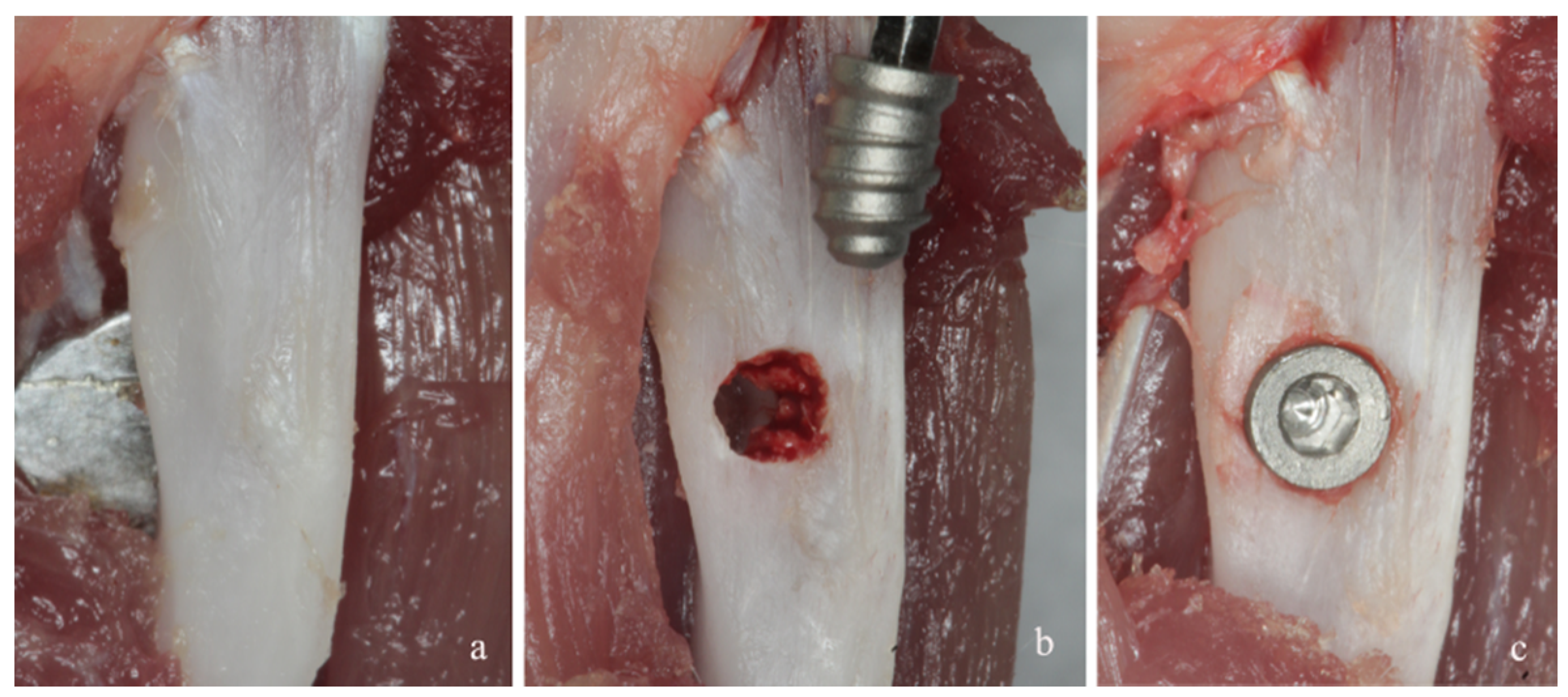
2.4. Implant Placement
2.5. Post-Operative Period
2.6. Torque-Force Evaluation for the Removal of Implants
2.7. Gene-Expression Analysis
2.8. Data Analyses
3. Results
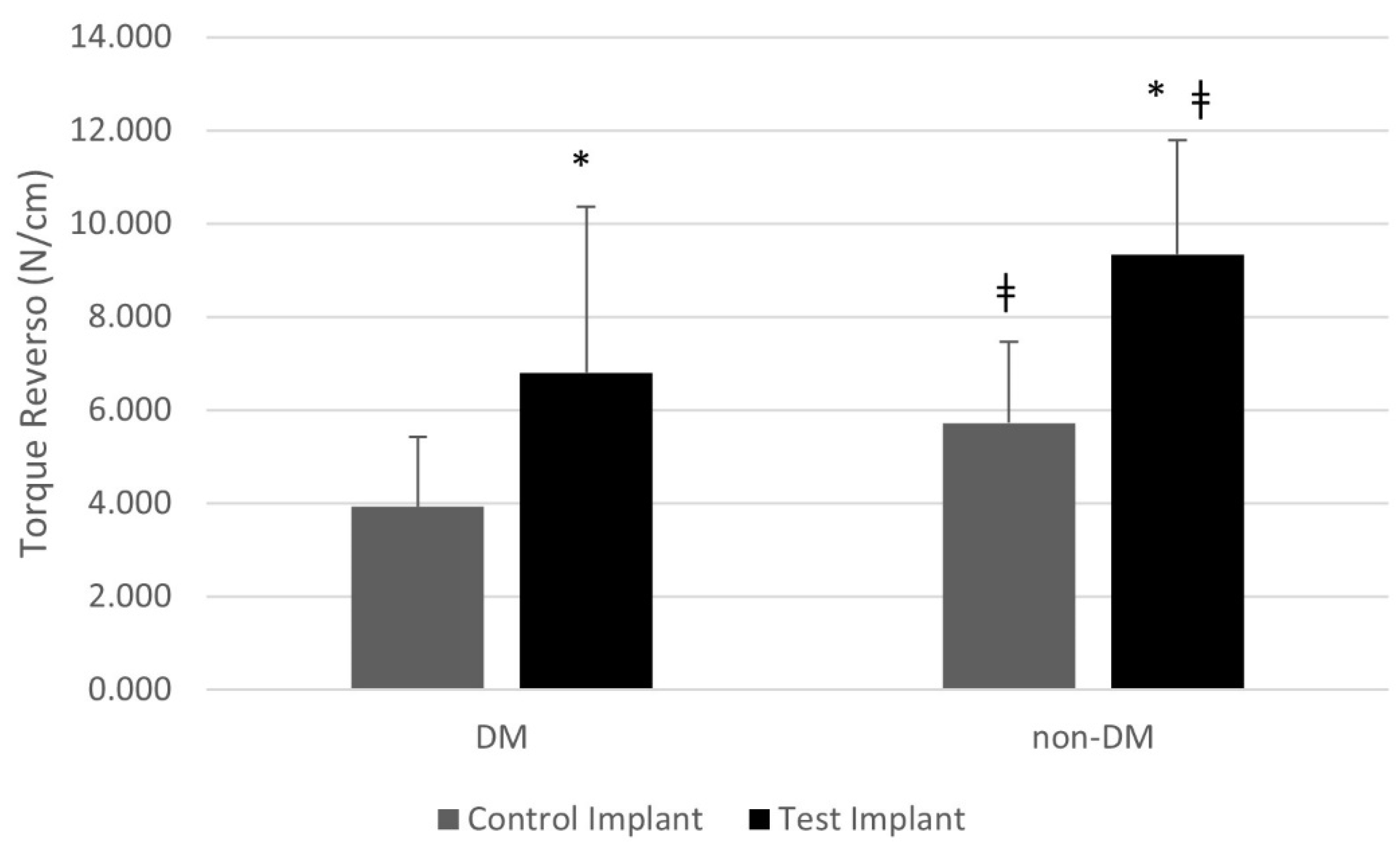
3.1. Torque-Force Evaluation
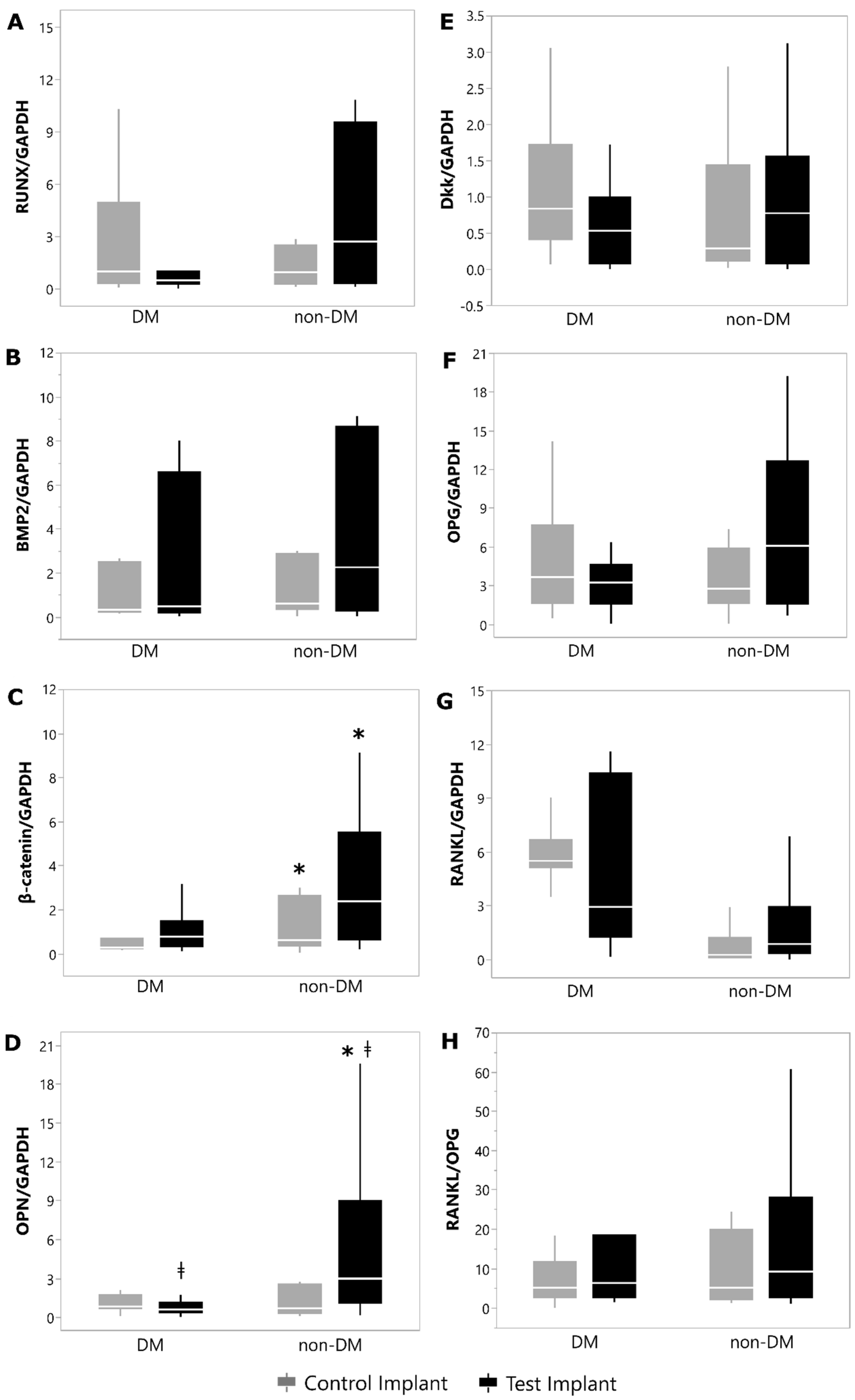
3.2. Gene-Expression Levels
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schmidt, A.M. Highlighting Diabetes Mellitus: The Epidemic Continues. Arterioscler. Thromb. Vasc. Biol. 2018, 38, e1–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Sinjari, B.; Feragalli, B.; Cornelli, U.; Belcaro, G.; Vitacolonna, E.; Santilli, M.; Rexhepi, I.; D’Addazio, G.; Zuccari, F.; Caputi, S. Artificial Saliva in Diabetic Xerostomia (ASDIX): Double Blind Trial of Aldiamed® Versus Placebo. J. Clin. Med. 2020, 9, 2196. [Google Scholar] [CrossRef]
- Verhulst, M.J.L.; Loos, B.G.; Gerdes, V.E.A.; Teeuw, W.J. Evaluating All Potential Oral Complications of Diabetes Mellitus. Front. Endocrinol. 2019, 10, 56. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.W.; Borgnakke, W.S. Periodontal disease: Associations with diabetes, glycemic control and complications. Oral Dis. 2008, 14, 191–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manouchehr-Pour, M.; Spagnuolo, P.J.; Rodman, H.M.; Bissada, N.F. Impaired neutrophil chemotaxis in diabetic patients with severe periodontitis. J. Dent. Res. 1981, 60, 729–730. [Google Scholar] [CrossRef]
- King, G.L. The role of inflammatory cytokines in diabetes and its complications. J. Periodontol. 2008, 79 (Suppl. S8), 1527–1534. [Google Scholar] [CrossRef]
- Schmidt, A.M.; Weidman, E.; Lalla, E.; Du Yan, S.; Hori, O.; Cao, R.; Brett, J.G.; Lamster, I.B. Advanced glycation endproducts (AGEs) induce oxidant stress in the gingiva: A potential mechanism underlying accelerated periodontal disease associated with diabetes. J. Periodont. Res. 1996, 31, 508–515. [Google Scholar] [CrossRef]
- Lalla, E.; Lamster, I.B.; Drury, S.; Fu, C.; Schmidt, A.M. Hyperglycemia, glycoxidation and receptor for advanced glycation endproducts: Potential mechanisms underlying diabetic complications, including diabetesassociated periodontitis. Periodontology 2000 2000, 23, 50–62. [Google Scholar] [CrossRef]
- Botero, J.E.; Yepes, F.L.; Roldán, N.; Castrillón, C.A.; Hincapie, J.P.; Ochoa, S.P.; Ospina, C.A.; Becerra, M.A.; Jaramillo, A.; Gutierrez, S.J.; et al. Tooth and periodontal clinical attachment loss are associated with hyperglycemia in patients with diabetes. J. Periodontol. 2012, 83, 1245–1250. [Google Scholar] [CrossRef]
- Sensorn, W.; Chatrchaiwiwatana, S.; Bumrerraj, S. Relationship between diabetes mellitus and tooth loss in adults residing in Ubonratchathani province, Thailand. J. Med. Assoc. Thai. 2012, 95, 1593–1605. [Google Scholar]
- Dannewitz, B.; Zeidler, A.; Hüsing, J.; Saure, D.; Pfefferle, T.; Eickholz, P.; Pretzl, B. Loss of molars in periodontally treated patients: Results 10 years and more after active periodontal therapy. J. Clin. Periodontol. 2016, 43, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Kutkut, A.; Bertoli, E.; Frazer, R.; Pinto-Sinai, G.; Hidalgo, R.F.; Studts, J. A systematic review of studies comparing conventional complete denture and implant retained overdenture. J. Prosthodont. Res. 2018, 62, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Pjetursson, B.E.; Glauser, R.; Zembic, A.; Zwahlen, M.; Lang, N.P. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin. Oral Implants Res. 2008, 19, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Barboza, E.S.; Peixoto, G.A. The impact of diabetes on dental implant failure: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 1237–1245. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors influencing early dental implant failures. J. Dent. Res. 2016, 95, 995–1002. [Google Scholar] [CrossRef]
- de Souza, J.G.; Neto, A.R.; Filho, G.S.; Dalago, H.R.; de Souza Júnior, J.M.; Bianchini, M.A. Impact of local and systemic factors on additional peri-implant bone loss. Quintessence Int. 2013, 44, 415–424. [Google Scholar]
- Enríquez-Pérez, I.A.; Galindo-Ordoñez, K.E.; Pantoja-Ortíz, C.E.; Martínez-Martínez, A.; Acosta-González, R.I.; Muñoz-Islas, E.; Jimenez-Andrade, J.M. Streptozocin-induced type-1 diabetes mellitus results in decreased density of CGRP sensory and TH sympathetic nerve fibers that are positively correlated with bone loss at the mouse femoral neck. Neurosci. Lett. 2017, 655, 28–34. [Google Scholar] [CrossRef]
- Aghaloo, T.; Pi-Anfruns, J.; Moshaverinia, A.; Sim, D.; Grogan, T.; Hadaya, D. The Effects of Systemic Diseases and Medications on Implant Osseointegration: A Systematic Review. Int. J. Oral Maxillofac. Implants 2019, 34, s35–s49. [Google Scholar] [CrossRef]
- Henderson, S.; Ibe, I.; Cahill, S.; Chung, Y.H.; Lee, F.Y. Bone Quality and Fracture-Healing in Type-1 and Type-2 Diabetes Mellitus. J. Bone Jt. Surg. Am. 2019, 101, 1399–1410. [Google Scholar] [CrossRef]
- Oates, T.W.; Dowell, S.; Robinson, M.; McMahan, C.A. Glycemic control and implant stabilization in type 2 diabetes mellitus. J. Dent. Res. 2009, 88, 367–371. [Google Scholar] [CrossRef]
- von Wilmowsky, C.; Stockmann, P.; Harsch, I.; Amann, K.; Metzler, P.; Lutz, R.; Moest, T.; Neukam, F.W.; Schlegel, K.A. Diabetes mellitus negatively affects peri-implant bone formation in the diabetic domestic pig. J. Clin. Periodontol. 2011, 38, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Ghiraldini, B.; Conte, A.; Casarin, R.C.; Casati, M.Z.; Pimentel, S.P.; Cirano, F.R.; Ribeiro, F.V. Influence of Glycemic Control on Peri-Implant Bone Healing: 12-Month Outcomes of Local Release of Bone-Related Factors and Implant Stabilization in Type 2 Diabetics. Clin. Implant. Dent. Relat. Res. 2016, 18, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Annibali, S.; Pranno, N.; Cristalli, M.P.; La Monaca, G.; Polimeni, A. Survival Analysis of Implant in Patients with Diabetes Mellitus: A Systematic Review. Implant Dent. 2016, 25, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Naujokat, H.; Kunzendorf, B.; Wiltfang, J. Dental implants and diabetes mellitus-a systematic review. Int. J. Implant. Dent. 2016, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Freitas, A.C., Jr.; Bonfante, E.A.; Giro, G.; Janal, M.N.; Coelho, P.G. The effect of implant design on insertion torque and immediate micromotion. Clin. Oral Implants Res. 2012, 23, 113–118. [Google Scholar] [CrossRef]
- Jimbo, R.; Tovar, N.; Anchieta, R.; Machado, L.S.; Marin, C.; Teixeira, H.; Coelho, P. The combined effects of undersized drilling and implant macrogeometry on bone healing around dental implants: An experimental study. Int J. Oral Maxillofac. Surg. 2014, 43, 1269–1275. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Tumedei, M.; Aramburú Júnior, J.; Treichel, T.L.; Kolerman, R.; Lepore, S.; Piattelli, A.; Iezzi, G. Histological and Histomorphometrical Evaluation of a New Implant Macrogeometry. A Sheep Study. Int. J. Environ. Res. Public Health 2020, 17, 3477. [Google Scholar] [CrossRef]
- Coelho, P.G.; Suzuki, M.; Guimaraes, M.V.; Marin, C.; Granato, R.; Gil, J.N.; Miller, R.J. Early bone healing around different implant bulk designs and surgical techniques: A study in dogs. Clin. Implant Dent. Relat. Res. 2010, 12, 202–208. [Google Scholar] [CrossRef]
- Marin, C.; Granato, R.; Suzuki, M.; Gil, J.N.; Janal, M.N.; Coelho, P.G. Histomorphologic and histomorphometric evaluation of various endosseous implant healing chamber configurations at early implantation times: A study in dogs. Clin. Oral Implants Res. 2010, 21, 577–583. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Eliers Treichel, T.L.; Pérez-Díaz, L.; Calvo-Guirado, J.L.; Aramburú Júnior, J.; Mazón, P.; de Aza, P.N. Impact of Different Titanium Implant Thread Animal Model. J. Clin. Med. 2019, 31, 6. [Google Scholar]
- Ikar, M.; Grobecker-Karl, T.; Karl, M.; Steiner, C. Mechanical stress during implant surgery and its effects on marginal bone: A literature review. Quintessence Int. 2020, 51, 142–150. [Google Scholar] [PubMed]
- Berglundh, T.; Abrahamsson, I.; Lang, N.P.; Lindhe, J. De novo alveolar bone formation adjacent to endosseous implants. Clin. Oral Implants Res. 2003, 14, 251–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implants Res. 2006, 17, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Campos, F.E.; Gomes, J.B.; Marin, C.; Teixeira, H.S.; Suzuki, M.; Witek, L.; Zanetta-Barbosa, D.; Coelho, P.G. Effect of drilling dimension on implant placement torque and early osseointegration stages: An experimental study in dogs. J. Oral Maxillofac. Surg. 2012, 70, e43–e50. [Google Scholar] [CrossRef]
- Monje, A.; Ravidà, A.; Wang, H.L.; Helms, J.A.; Brunski, J.B. Relationship between Primary/Mechanical and Secondary/Biological Implant Stability. Int. J. Oral Maxillofac. Implants 2019, 34, s7–s23. [Google Scholar] [CrossRef]
- Boissy, P.; Andersen, T.L.; Abdallah, B.M.; Kassem, M.; Plesner, T.; Delaisse’, J.M. Resveratrol inhibits myeloma cell growth, prevents osteoclast formation, and promotes osteoblast differentiation. Cancer Res. 2005, 65, 9943–9952. [Google Scholar] [CrossRef] [Green Version]
- Komori, T. Regulation of Proliferation, Differentiation and Functions of Osteoblasts by Runx2. Int. J. Mol. Sci. 2019, 20, 1694. [Google Scholar] [CrossRef] [Green Version]
- Simonet, W.; Lacey, D.; Dunstan, C.; Kelley, M.; Chang, M.-S.; Lüthy, R.; Nguyen, H.; Wooden, S.; Bennett, L.; Boone, T.; et al. Osteoprotegerin: A novel secreted protein involved in the regulation of bone density. Cell 1997, 89, 309–319. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, H.; Shima, N.; Nakagawa, N.; Yamaguchi, K.; Kinosaki, M.; Goto, M. A novel molecular mechanism modulating osteoclast differentiation and function. Bone 1999, 25, 109–113. [Google Scholar] [CrossRef]
- Gregory, C.; Singh, H.; Perry, A.S.; Prockop, D.J. The Wnt Signaling Inhibitor Dickkopf-1 Is Required for Reentry into the Cell Cycle of Human Adult Stem Cells from Bone Marrow. J. Biol. Chem. 2003, 278, 28067–28078. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, B.T.; Joiner, D.M.; Oyserman, S.M.; Sharma, P.; Goldstein, S.A.; He, X.; Hauschka, P.V. Bone mass is inversely proportional to Dkk1 levels in mice. Bone 2007, 41, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrêa, M.G.; Gomes Campos, M.L.; Marques, M.R.; Casati, M.Z.; Nociti, F.H., Jr.; Sallum, E.A. Histometric analysis of the effect of enamel matrix derivative on the healing of periodontal defects in rats with diabetes. J. Periodontol. 2013, 84, 1309–1318. [Google Scholar] [CrossRef] [PubMed]
- Kador, P.F.; O’Meara, J.D.; Blessing, K.; Marx, D.B.; Reinhardt, R.A. Efficacy of structurally diverse aldose reductase inhibitors on experimental periodontitis in rats. J. Periodontol. 2011, 82, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, F.V.; Pimentel, S.P.; Corrêa, M.G.; Bortoli, J.P.; Messora, M.R.; Casati, M.Z. Resveratrol reverses the negative effect of smoking on peri-implant repair in the tibia of rats. Clin. Oral Implants Res. 2019, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, S.P.; Casarin, R.C.; Ribeiro, F.V.; Cirano, F.R.; Rovaris, K.; Neto, F.H.; Casati, M.Z.; Haiter, F. Impact of micronutrients supplementation on bone repair around implants: microCT and counter-torque analysis in rats. J. Appl. Oral Sci. 2016, 24, 45–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conte, A.; Ghiraldini, B.; Casarin, R.; Casati, M.; Pimentel, S.; Cirano, F.; Duarte, P.; Ribeiro, F. Impact of type 2 diabetes on the gene expression of bone-related factors at sites receiving dental implants. Int. J. Oral Maxillofac. Surg. 2015, 44, 1302. [Google Scholar] [CrossRef]
- Reyes-Garcia, R.; Rozas-Moreno, P.; Lopez-Gallardo, G.; Garcia-Martin, A.; Varsavsky, M.; Avilés-Pérez, M.D.; Muñoz-Torres, M. Serum levels of bone resorption markers are decreased in patients with type 2 diabetes. Acta Diabetol. 2013, 50, 47–52. [Google Scholar] [CrossRef]
- Farr, J.N.; Drake, M.T.; Amin, S.; Melton, L.J., 3rd; McCready, L.K.; Khosla, S. In vivo assessment of bone quality in postmenopausal women with type 2 diabetes. J. Bone Miner. Res. 2014, 29, 787–795. [Google Scholar] [CrossRef]
- Camargo, W.A.; de Vries, R.; van Luijk, J.; Hoekstra, J.W.; Bronkhorst, E.M.; Jansen, J.A.; van den Beucken, J.J. Diabetes Mellitus and Bone Regeneration: A Systematic Review and Meta-Analysis of Animal Studies. Tissue Eng. Part B Rev. 2017, 23, 471–479. [Google Scholar] [CrossRef]
- Wang, L.; Hu, X.; Ma, X.; Ma, Z.; Zhang, Y.; Lu, Y.; Li, X.; Lei, W.; Feng, Y. Promotion of osteointegration under diabetic conditions by tantalum coating-based surface modification on 3-dimensional printed porous titanium implants. Colloids Surf. B Biointerfaces 2016, 148, 440–452. [Google Scholar] [CrossRef]
- Leonard, G.; Coelho, P.; Polyzois, I.; Stassen, L.; Claffey, N. A study of the bone healing kinetics of plateau versus screw root design titanium dental implants. Clin. Oral Implants Res. 2009, 20, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Jimbo, R. Osseointegration of metallic devices: Current trends based on implant hardware design. Arch. Biochem. Biophys. 2014, 561, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Dedavid, B.A.; Aramburú, J.S.; Pérez-Díaz, L.; Guirado, J.L.; Canales, P.M.; De Aza, P.N. Effect of Different Morphology of Titanium Surface on the Bone Healing in Defects Filled Only with Blood Clot: A New Animal Study Design. Biomed. Res. Int. 2018, 8, 4265474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonfante, E.; Granato, R.; Marin, C.; Suzuki, M.; Oliveira, S.R.; Giro, G.; Coelho, P.G. Early bone healing and biomechanical fixation of dual acid-etched and as-machined implants with healing chambers: An experimental study in dogs. Int. J. Oral Maxillofac. Implants 2011, 26, 75–82. [Google Scholar]
- Barros, R.R.; Novaes, A.B., Jr.; Papalexiou, V.; Souza, S.L.; Taba, M., Jr.; Palioto, D.B.; Grisi, M.F. Effect of biofunctionalized implant surface on osseointegration: A histomorphometric study in dogs. Braz. Dent. J. 2009, 20, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Meng, H.; Wang, Z.; Wang, W.; Li, W.; Wu, Q.; Lei, X.; Ouyang, X.; Liang, Z. Effect of osteopontin in regulating bone marrow mesenchymal stem cell treatment of skin wounds in diabetic mice. Diabetes Metab. Res. Rev. 2014, 30, 457–466. [Google Scholar] [CrossRef]
- Feldbrin, Z.; Omelchenko, E.; Lipkin, A.; Shargorodsky, M. Osteopontin levels in plasma, muscles, and bone in patient with non-healing diabetic foot ulcers: A new player in wound healing process? J. Diabetes Complicat. 2018, 32, 795–798. [Google Scholar] [CrossRef]
- Cirano, F.; Pimentel, S.; Casati, M.; Corrêa, M.; Pino, D.; Messora, M.; Silva, P.; Ribeiro, F. Effect of curcumin on bone tissue in the diabetic rat: Repair of peri-implant and critical-sized defects. Int. J. Oral Maxillofac. Surg. 2018, 47, 1495–1503. [Google Scholar] [CrossRef]
- Ma, R.; Wang, L.; Zhao, B.; Liu, C.; Liu, H.; Zhu, R.; Chen, B.; Li, L.; Zhao, D.; Mo, F.; et al. Diabetes Perturbs Bone Microarchitecture and Bone Strength through Regulation of Sema3A/IGF-1/β-Catenin in Rats. Cell Physiol. Biochem. 2017, 41, 55–66. [Google Scholar] [CrossRef]
- Giachelli, C.M.; Steitz, S. Osteopontin: A versatile regulator of inflammation and biomineralization. Matrix Biol. 2000, 19, 615–622. [Google Scholar] [CrossRef]
- Duvall, C.L.; Taylor, W.R.; Weiss, D.; Wojtowicz, A.M.; Guldberg, R.E. Impaired angiogenesis, early callus formation, and late stage remodeling in fracture healing of osteopontin-deficient mice. J. Bone Miner. Res. 2007, 222, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.K. Role of osteopontin in modulation of hydroxyapatite formation. Calcif. Tissue Int. 2013, 934, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Meirelles, L.; Brånemark, P.I.; Albrektsson, T.; Feng, C.; Johansson, C. Histological evaluation of bone formation adjacent to dental implants with a novel apical chamber design: Preliminary data in the rabbit model. Clin. Implant Dent. Relat. Res. 2015, 17, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Ayukawa, Y.; Takeshita, F.; Inoue, T.; Yoshinari, M.; Shimono, M.; Suetsugu, T.; Tanaka, T. An immunoelectron microscopic localization of noncollagenous bone proteins (osteocalcin and osteopontin) at the bone-titanium interface of rat tibiae. J. Biomed. Mater. Res. 1998, 41, 111–119. [Google Scholar] [CrossRef]
- Chen, Q.; Shou, P.; Zhang, L.; Xu, C.; Zheng, C.; Han, Y.; Li, W.; Huang, Y.; Zhang, X.; Shao, C.; et al. An osteopontin-integrin interaction plays a critical role in directing adipogenesis and osteogenesis by mesenchymal stem cells. Stem Cells 2014, 322, 327–337. [Google Scholar] [CrossRef] [Green Version]
- Sundar, G.; Sridharan, S.; Sundaram, R.R.; Prabhu, S.; Rao, R.; Rudresh, V. Impact of well-controlled type 2 diabetes mellitus on implant stability and bone biomarkers. Int. J. Oral Maxillofac. Implants 2019, 34, 1441–1449. [Google Scholar]
- Raheja, L.F.; Genetos, D.C.; Yellowley, C.E. Hypoxic osteocytes recruit human MSCs through an OPN/CD44-mediated pathway. Biochem. Biophys. Res. Commun. 2008, 3664, 1061–1066. [Google Scholar] [CrossRef]
- Zou, C.; Luo, Q.; Qin, J.; Shi, Y.; Yang, L.; Ju, B.; Song, G. Osteopontin promotes mesenchymal stem cell migration and lessens cell stiffness via integrin beta1, FAK, and ERK pathways. Cell Biochem. Biophys. 2013, 653, 455–462. [Google Scholar] [CrossRef]
- Natoli, R.M.; Yu, H.; Meislin, M.C.-M.; Abbasnia, P.; Roper, P.; Vuchkovska, A.; Xiao, X.; Stock, S.R.; Callaci, J.J. Alcohol exposure decreases osteopontin expression during fracture healing and osteopontin-mediated mesenchymal stem cell migration in vitro. J. Orthop. Surg. Res. 2018, 13, 101. [Google Scholar] [CrossRef] [Green Version]
- Rangaswami, H.; Bulbule, A.; Kundu, G.C. Osteopontin: Role in cell signaling and cancer progression. Trends Cell Biol. 2006, 16, 79–87. [Google Scholar] [CrossRef]
- Serrão, C.; Bastos, M.; Cruz, D.; Malta, F.; Vallim, P.; Duarte, P. Role of Metformin in Reversing the Negative Impact of Hyperglycemia on Bone Healing Around Implants Inserted in Type 2 Diabetic Rats. Int. J. Oral Maxillofac. Implants 2017, 32, 547–554. [Google Scholar] [CrossRef]
- Alkan, A.; Erdem, E.; Günhan, O.; Karasu, C. Histomorphometric evaluation of the effect of doxycycline on the healing of bone defects in experimental diabetes mellitus: A pilot study. J. Oral Maxillofac. Surg. 2002, 60, 898–904. [Google Scholar] [CrossRef]
- Yu, M.; Zhou, W.; Song, Y.; Yu, F.; Li, D.; Na, S.; Zou, G.; Zhai, M.; Xie, C. Development of mesenchymal stem cell-implant complexes by cultured cells sheet enhances osseointegration in type 2 diabetic rat model. Bone 2011, 49, 387–394. [Google Scholar] [CrossRef]
- Ajami, E.; Mahno, E.; Mendes, V.C.; Bell, S.; Moineddin, R.; Davies, J.E. Bone healing and the effect of implant surface topography on osteoconduction in hyperglycemia. Acta Biomater. 2014, 10, 394–405. [Google Scholar] [CrossRef]
- Rybaczek, T.; Tangl, S.; Dobsak, T.; Gruber, R.; Kuchler, U. The effect of parathyroid hormone on osseointegration in insulin-treated diabetic rats. Implant Dent. 2015, 24, 392–396. [Google Scholar] [CrossRef] [Green Version]
- Altug, H.A.; Tatli, U.; Coskun, A.T.; Erdogan, Ö.; Özkan, A.; Sencimen, M.; Kürkçü, M. Effects of hyperbaric oxygen treatment on implant osseointegration in experimental diabetes mellitus. J. Appl. Oral Sci. 2016, 26, e20180083. [Google Scholar] [CrossRef]
- Sinibaldi, R.; Conti, A.; Sinjari, B.; Spadone, S.; Pecci, R.; Palombo, M.; Komlev, V.S.; Ortore, M.G.; Tromba, G.; Capuani, S.; et al. Multimodal-3D imaging based on μMRI and μCT techniques bridges the gap with histology in visualization of the bone regeneration process. J. Tissue Eng. Regen. Med. 2018, 12, 750–761. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Sequence (5′–3′) | Length of qPCR Product (bp) | Amplification Profile (Temperature, Time) |
|---|---|---|---|
| Runx2 | GCCACTTACCACAGAGC | 157 | 95 °C, 10 s/56 °C, 8 s/72 °C, 7 s |
| BMP-2 | GTCCCTACTGATGATGAGTTTCTC | 170 | 95 °C, 10 s/56 °C, 8 s/72 °C, 8 s |
| OPN | CCGGATGCAATCGATAGTG | 164 | 95 °C, 10 s/56 °C, 7 s/72 °C, 8 s |
| β-catenin | ACTCTGAGAAACTTGTCCG | 172 | 95 °C, 10 s/56 °C, 8 s/72 °C, 8 s |
| Dkk1 | CGGGAATTACTGCAAAAACG | 83 | 95 °C, 9 s/59 °C, 9 s/72 °C, 9 s |
| RANKL | AGCGCTTCTCAGGAGTT | 156 | 95 °C, 5 s/55 °C, 4 s/72 °C, 6 s |
| OPG | GCAGAGAAGCACCTAGC | 168 | 95 °C, 10 s/56 °C, 8 s/72 °C, 7 s |
| GAPDH | TGAGTATGTCGTGGAGTCTACTG | 159 | 95 °C, 10 s/56 °C, 8 s/72 °C, 7 s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sant’Anna, H.R.; Casati, M.Z.; Mussi, M.C.; Cirano, F.R.; Pimentel, S.P.; Ribeiro, F.V.; Corrêa, M.G. Peri-Implant Repair Using a Modified Implant Macrogeometry in Diabetic Rats: Biomechanical and Molecular Analyses of Bone-Related Markers. Materials 2022, 15, 2317. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15062317
Sant’Anna HR, Casati MZ, Mussi MC, Cirano FR, Pimentel SP, Ribeiro FV, Corrêa MG. Peri-Implant Repair Using a Modified Implant Macrogeometry in Diabetic Rats: Biomechanical and Molecular Analyses of Bone-Related Markers. Materials. 2022; 15(6):2317. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15062317
Chicago/Turabian StyleSant’Anna, Hugo Robertson, Marcio Zaffalon Casati, Mounir Colares Mussi, Fabiano Ribeiro Cirano, Suzana Peres Pimentel, Fernanda Vieira Ribeiro, and Mônica Grazieli Corrêa. 2022. "Peri-Implant Repair Using a Modified Implant Macrogeometry in Diabetic Rats: Biomechanical and Molecular Analyses of Bone-Related Markers" Materials 15, no. 6: 2317. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15062317