Pivoting Dental Practice Management during the COVID-19 Pandemic—A Systematic Review

 , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcome and Review Question
2.2. Data Sources and Study Selection
2.3. Risk of Bias Assessment

{kind=link}
{kind=link}
| Selection | Comparability | Outcome | Overall | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study & Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Score (*) |
| Kamate S.T et al., 2020 [26] | * | * | * | * | * | * | 6 | ||||
| Schacham et al., 2020 [27] | * | * | * | * | * | * | * | 7 | |||
| Ahmed M.A et al., 2020 [28] | * | * | * | * | * | * | * | 7 | |||
| Khader Y et al., 2020 [29] | * | * | * | * | * | * | 6 | ||||
| Yang Y et al., 2020 [30] | * | * | * | * | * | * | * | * | 8 | ||
| Al Harbi et al., 2020 [31] | * | * | * | * | * | * | 6 | ||||
2.4. Statistical Analysis
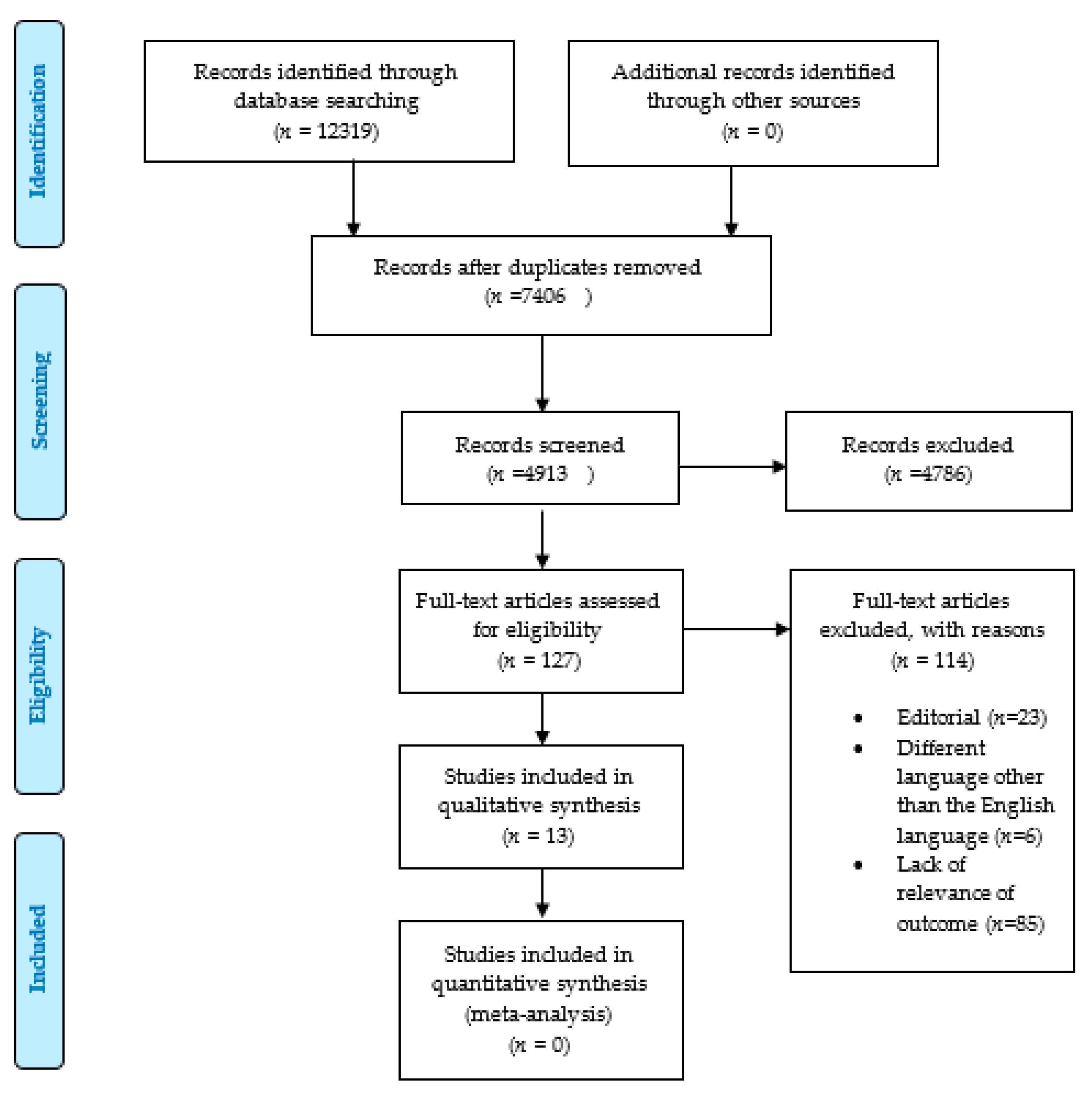
3. Results
4. Discussion
4.1. (a) Patient Triage Prior to Patient Arrival
4.2. (b) Patient Evaluation and Screening Upon Arrival
4.3. (c) Infection Control during Dental Treatment
4.4. (d) Disinfection after Treatment
4.5. Psychological Impact of COVID-19 among Dental Professionals
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lake, M.A. What we know so far: COVID-19 current clinical knowledge and research. Clin. Med. 2020, 20, 124–127. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/?gclid=Cj0KCQjwhIP6BRCMARIsALu9LfnBrJCWM-3csCkflq1Ni0GKcv-W0z7_mRrqt7ZKBvxWY2zG1NBx3GMaAsZ-EALw_wcB (accessed on 22 August 2020).
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Coronavirus Update (Live): 34,838,209 Cases and 1,033,356 Deaths from COVID-19 Virus Pandemic—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 3 October 2020).
- Duda-Chodak, A.; Lukasiewicz, M.; Zięć, G.; Florkiewicz, A.; Filipiak-Florkiewicz, A. Covid-19 pandemic and food: Present knowledge, risks, consumers fears and safety. Trends Food Sci. Technol. 2020, 105, 145–160. [Google Scholar] [CrossRef]
- Roy, S. COVID-19 pandemic: Impact of lockdown, contact and non-contact transmissions on infection dynamics. medRxiv 2020. [Google Scholar] [CrossRef]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China. Emerg. Infect. Dis. 2020, 26, 1343–1345. [Google Scholar] [CrossRef]
- Lu, C.-W.; Liu, X.-F.; Jia, Z.-F. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet 2020, 395, e39. [Google Scholar] [CrossRef] [Green Version]
- Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.-G.; Cheshmi, B. Being a front-line dentist during the Covid-19 pandemic: A literature review. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 1–9. [Google Scholar] [CrossRef]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, L.P.; Sanabria, A.; Ridge, J.A.; Ng, W.T.; De Bree, R.; Rinaldo, A.; Takes, R.; Mäkitie, A.A.; Carvalho, A.L.; Bradford, C.R.; et al. COVID -19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020, 42, 1259–1267. [Google Scholar] [CrossRef] [Green Version]
- Nicola, M.; O’Neill, N.; Sohrabi, C.; Khan, M.; Agha, M.; Agha, R. Evidence based management guideline for the COVID-19 pandemic—Review article. Int. J. Surg. 2020, 77, 206–216. [Google Scholar] [CrossRef]
- Evans, K.L.; Ewen, J.G.; Guillera-Arroita, G.; Johnson, J.A.; Penteriani, V.; Ryan, S.J.; Sollmann, R.; Gordon, I.J. Conservation in the maelstrom of Covid-19—A call to action to solve the challenges, exploit opportunities and prepare for the next pandemic. Anim. Conserv. 2020, 23, 235–238. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Li, G.; Chang, B.; Li, H.; Wang, R.; Li, G. Precautions in dentistry against the outbreak of corona virus disease. J. Infect. Public Health 2020. [Google Scholar] [CrossRef]
- Ramos-Gomez, F.; Folayan, M.; Campus, G. Global Impact of COVID-19 on Service Delivery and Vulnerable Populations’ Access to Dental Care. CAD J. 2020, 48, 507–516. [Google Scholar]
- Patil, S.; Bhandi, S.; Gambarini, G.; Seracchiani, M.; Testarelli, L.; Miccoli, G.; Di Nardo, D.; Obino, F.V.; Galli, M.; Gambarini, E. Fine Aerosols and Perceived Risk of COVID-19 among Italian Dental Practitioners: An Experimental Survey. J. Contemp. Dent. Pr. 2020, 21, 599–603. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, W.; Zhao, X.; Zhang, W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: A model of West China Hospital. Precis. Clin. Med. 2020, 3, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Gurzawska-Comis, K.; Becker, K.; Giulia, B.; Agata, G.; Schwarz, F. Recommendations for dentists during COVID-19. Clin. Oral Implant. Res. 2020, 31, 158. [Google Scholar] [CrossRef]
- Simon, L. How Will Dentistry Respond to the Coronavirus Disease 2019 (COVID-19) Pandemic? JAMA Health Forum 2020, 1, e200625. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.J. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Kamate, S.K.; Sharma, S.; Thakar, S.; Srivastava, D.; Sengupta, K.; Hadi, A.J.; Chaudhary, A.; Joshi, R.; Dhanker, K. Assessing Knowledge, Attitudes and Practices of dental practitioners regarding the COVID-19 pandemic: A multinational study. Dent. Med. Probl. 2020, 57, 11–17. [Google Scholar] [CrossRef]
- Shacham, M.; Hamama-Raz, Y.; Kolerman, R.; Mijiritsky, O.; Ben-Ezra, M.; Mijiritsky, E. COVID-19 Factors and Psychological Factors Associated with Elevated Psychological Distress among Dentists and Dental Hygienists in Israel. Int. J. Environ. Res. Public Health 2020, 17, 2900. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.A.; Jouhar, R.; Ahmed, N.; Adnan, S.; Aftab, M.; Zafar, M.S.; Khurshid, Z. Fear and Practice Modifications among Dentists to Combat Novel Coronavirus Disease (COVID-19) Outbreak. Int. J. Environ. Res. Public Health 2020, 17, 2821. [Google Scholar] [CrossRef]
- Khader, Y.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S.; Alshurman, B.A. Dentists’ Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study Among Jordanian Dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef]
- Yang, Y.; Zhou, Y.; Liu, X.; Tan, J. Health services provision of 48 public tertiary dental hospitals during the COVID-19 epidemic in China. Clin. Oral Investig. 2020, 24, 1861–1864. [Google Scholar] [CrossRef] [Green Version]
- Alharbi, A.; Alharbi, S.; Alqaidi, S. Guidelines for dental care provision during the COVID-19 pandemic. Saudi Dent. J. 2020, 32, 181–186. [Google Scholar] [CrossRef]
- Gambhir, R.S.; Dhaliwal, J.S.; Aggarwal, A.; Anand, S.; Anand, V.; Bhangu, A.K. Covid-19: A survey on knowledge, awareness and hygiene practices among dental health professionals in an Indian scenario. Rocz. Państw. Zakł. Hig. 2020, 71, 223–229. [Google Scholar]
- Cagetti, M.G.; Cairoli, J.L.; Senna, A.; Guglielmo Campus COVID-19 Outbreak in North Italy: An Overview on Dentistry. A Questionnaire Survey. Int. J. Environ. Res. Public Health 2020, 17, 3835. [Google Scholar] [CrossRef]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Sarfaraz, S.; Shabbir, J.; Mudasser, M.A.; Khurshid, Z.; Al-Quraini, A.A.A.; Abbasi, M.S.; Ratnayake, J.; Zafar, M.S. Knowledge and Attitude of Dental Practitioners Related to Disinfection during the COVID-19 Pandemic. Healthcare 2020, 8, 232. [Google Scholar] [CrossRef]
- Consolo, U.; Bellini, P.; Bencivenni, D.; Iani, C.; Checchi, V. Epidemiological Aspects and Psychological Reactions to COVID-19 of Dental Practitioners in the Northern Italy Districts of Modena and Reggio Emilia. Int. J. Environ. Res. Public Health 2020, 17, 3459. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Ge, Z.-Y.; Yang, L.-M.; Xia, J.-J.; Fu, X.-H.; Zhang, Y.-Z. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J. Zhejiang Univ. Sci. B 2020, 21, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.; Nkenke, E. Approaches to the management of patients in oral and maxillofacial surgery during COVID-19 pandemic. J. Cranio Maxillofac. Surg. 2020, 48, 521–526. [Google Scholar] [CrossRef]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus disease 19 (COVID-19): Implications for clinical dental care. J. Endodont. 2020, 46. in press. [Google Scholar]
- Izzetti, R.; Nisi, M.; Gabriele, M.; Graziani, F. COVID-19 Transmission in Dental Practice: Brief Review of Preventive Measures in Italy. J. Dent. Res. 2020, 99, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Cui, B.; Duan, X.; Zhang, P.; Zhou, X.; Yuan, Q. Saliva: Potential diagnostic value and transmission of 2019-nCoV. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection Control in Dental Practice During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef]
- Horzov, L.; Goncharuk-Khomyn, M.; Kostenko, Y.; Melnyk, V. Dental Patient Management in the Context of the COVID-19 Pandemic: Current Literature Mini-Review. Open Public Health J. 2020, 13, 459–463. [Google Scholar] [CrossRef]
- Chandy, P.E.; Nasir, M.U.; Srinivasan, S.; Klass, D.; Nicolaou, S.; Babu, S.B. Interventional radiology and COVID-19: Evidence-based measures to limit transmission. Diagn. Interv. Radiol. 2020, 26, 236–240. [Google Scholar] [CrossRef]
- Mousavi, E.; Kananizadeh, N.; Martinello, R.A.; Sherman, J.D. COVID-19 Outbreak and Hospital Air Quality: A Systematic Review of Evidence on Air Filtration and Recirculation. Environ. Sci. Technol. 2020. [Google Scholar] [CrossRef]
- Diaz, K.T.; Smaldone, G.C. Quantifying exposure risk: Surgical masks and respirators. Am. J. Infect. Control. 2010, 38, 501–508. [Google Scholar] [CrossRef]
- Fine, D.H.; Mendieta, C.; Barnett, M.L.; Furgang, D.; Meyers, R.; Olshan, A.; Vincent, J. Efficacy of Preprocedural Rinsing with an Antiseptic in Reducing Viable Bacteria in Dental Aerosols. J. Periodontol. 1992, 63, 821–824. [Google Scholar] [CrossRef]
- Harrel, S.K.; Molinari, J. Aerosols and splatter in dentistry. J. Am. Dent. Assoc. 2004, 135, 429–437. [Google Scholar] [CrossRef]
- Samaranayake, L.P.; Reid, J.; Evans, D. The efficacy of rubber dam isolation in reducing atmospheric bacterial contamination. ASDC J. Dent. Child. 1989, 56, 442–444. [Google Scholar]
- Al-Amad, S.H.; Awad, M.A.; Edher, F.M.; Shahramian, K.; Omran, T.A. The effect of rubber dam on atmospheric bacterial aerosols during restorative dentistry. J. Infect. Public Health 2017, 10, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Hu, T.; Li, G.; Zuo, Y.; Zhou, X. Risk of Hepatitis B Virus Transmission via Dental Handpieces and Evaluation of an Antisuction Device for Prevention of Transmission. Infect. Control. Hosp. Epidemiol. 2007, 28, 80–82. [Google Scholar] [CrossRef]
- Tellier, R.; Li, Y.; Cowling, B.J.; Tang, J.W. Recognition of aerosol transmission of infectious agents: A commentary. BMC Infect. Dis. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Wenzel, R.P.; Edmond, M.B. Managing SARS amidst Uncertainty. N. Engl. J. Med. 2003, 348, 1947–1948. [Google Scholar] [CrossRef]
- Dexter, F.; Parra, M.C.; Brown, J.R.; Loftus, R.W. Perioperative COVID-19 defense: An evidence-based approach for optimization of infection control and operating room management. Anesth. Analg. 2020. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, B.; Cui, W.; Dong, L.; An, N.; Ouyang, X. The effectiveness of an air cleaner in controlling droplet/aerosol particle dispersion emitted from a patient’s mouth in the indoor environment of dental clinics. J. R. Soc. Interface 2010, 7, 1105–1118. [Google Scholar] [CrossRef]
- Hallier, C.; Williams, D.W.; Potts, A.J.C.; Lewis, M.A.O. A pilot study of bioaerosol reduction using an air cleaning system during dental procedures. Br. Dent. J. 2010, 209, E14. [Google Scholar] [CrossRef]


| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Articles published after the COVID-19 outbreak (Dec 2019 onwards) | Studies published prior to COVID-19 |
| English language only | Articles not in the English language |
| Original articles and reviews | Editorials, opinions, perspective, correspondences, case reports, case series |
| Only articles published in peer-review and indexed journals | Non-peer-reviewed/nonindexed journals |
| Databases examined (PubMed, CINAHL, Scopus, Embase, Google Scholar) | Little or no focus on dental aspects |
| Keywords/Search Strings | Number of Entries Found |
|---|---|
| COVID-19 | 12,137 |
| COVID-19 and dentistry | 46 |
| Novel corona virus | 63 |
| COVID-19 and oral health | 41 |
| Dental practice and novel corona virus | 6 |
| Dental health and novel corona virus | 26 |
| Novel corona virus and dentistry | 0 |
| First Author (Date) | Type of Article | Population/Setting | Article Key Points | Recommendations/Outcomes | Limitations |
|---|---|---|---|---|---|
| Peng, et al., 2020 [31] | Review Article | Setup: Routes of 2019-nCoV transmission and control in dental practice. Context: China | Dental care environments typically bear the possibility of contamination with 2019-nCoV owing to the complexity of its practice, which requires face-to-face contact with patients. Patients and dentists can be exposed via inhalation of suspended airborne particles, indirect contact from contaminated surfaces, and direct contact with bodily fluids of infected individuals. |
| Lack of evidence for the effectiveness of chlorhexidine mouth rinse against 2019-nCoV |
| |||||
| |||||
| |||||
| |||||
| |||||
| |||||
| |||||
| Meng, L. et al., 2020 [32] | Review Article | Setup: Risk of cross-infection in dental settings. Context: China. | This study offers critical information regarding COVID-19 and nosocomial infections in dental settings. Management and guidelines for dental practitioners and students in (potentially) infected areas. |
| None |
| |||||
| |||||
| Ge, Z. et al., 2020 [33] | Review Article | Setup: Transmission and control of COVID-19 infection in dental settings via aerosol. Context: China | The article emphasizes the importance of aerosol transmission of COVID-19 in dental settings and the implementation of precautionary measures to limit its spread. |
| Distinguishing symptoms of fever and fatigue caused by dental infections from COVID-19 is merely dependent on the practitioner’s expertise. Effect of preprocedural mouth rinse against SARS-Cov-2 with oxidative agents and chlorhexidine is still unknown. |
| |||||
| |||||
| |||||
| Kamate, S.K. et al., 2020 [40] | KAP Study | Setup: 860 dental practitioners from different continents. Context: Global | The present research was conducted with the intention of evaluating the awareness, behaviors, and activities (KAP) of dental practitioners in light of the COVID-2019 pandemic. |
| A bias in social desirability. |
| Owing to the cross-sectional aspect of the sample and the sampling method used, the effect of self-selection of the part of the respondents may have arisen. Questionnaire bias. | ||||
| Yang, Y. et al., 2020 [34] | Original Article | Setup: 48 public tertiary dental hospitals. Context: China | The state of nonemergency dental care, emergency dental facilities, online consultation, and regional spread of hospitals were evaluated during the COVID-19 pandemic. |
| Within the limitation of this report, we observed significant changes in the health service provision of Chinese public tertiary hospitals during the COVID-19 epidemic. Nonetheless, more research should concentrate on the possible long-term effects that the outbreak may contribute on dental treatment. |
| |||||
| Zimerman et al., 2020 [35] | Review Article | Setup: Risk of COVID 19 risk in Oral and Maxillofacial Surgery Department. Context: Vienna | The purpose of the study is therefore to compile and address facets of the treatment of patients in oral and maxillofacial surgery during the COVID-19 pandemic. |
| Necessary investments should be made for dreadful future situations. |
| |||||
| |||||
| |||||
| Ather, A. et al., 2020 [36] | Review Article | Setup: Recommendations for clinical dental practice in COVID-19. Context: USA | The purpose of this article is to provide a summary of the epidemiology, symptoms, and mechanisms of transmission of this novel infection. Implications for clinical dental practice in response to COVID-19 have been highlighted. |
| Likelihood of treating an asymptomatic COVID-19 patient in a dental setting is high due to the large incubation period from 0 to 24 days and mild presentation of disease in some individuals. |
| |||||
| |||||
| |||||
| |||||
| |||||
| AlHarbi, A. et al., 2020 [37] | Original Article | Setup: Recommended provisions for dental care during the COVID-19 pandemic. Context: Global | This research sought to establish recommendations for the treatment of dental patients before and after the COVID-19 pandemic. |
| The recommendations established in this research are general guidance and the final decision will always be made at the discretion of the practitioner. |
| |||||
| |||||
| Khader, Y. et al., 2020 [41] | Cross-sectional study | Setup: 368 Jordanian dentists from private clinics, hospitals, and health centers. Context: Jordan | The study assessed the degree of understanding, interpretation, and attitude of COVID-19 and infection management among Jordanian dentists. |
| Low response rate, Selection bias, and sampling error limits the generalizability of the findings |
| Izzeti, R. et al., 2020 [38] | Review Article | Setup: Risk of transmission of COVID-19 in dental practice and preventive measures. Context: Italy. | There is a substantial risk of direct and indirect transmission of COVID-19 among dental practitioners and between patients when performing dental procedures with handpiece under irrigation due to generation of aerosol and surface/environmental contamination. |
| There is a lack of systemic data on the use of chlorhexidine against SARS-CoV-2. Lack of evidence, data, and unpredictable nature of this disease is affecting the adequate delivery of clinical dental care. |
| Xu, R. et al., 2020 [39] | Review Article | Setup: Role of Saliva in transmission and diagnostic tool for 2019-nCoV. Context: China | The article discusses saliva being a potential noninvasive diagnostic tool for 2019-nCoV detection and a potential transient medium for the spread of infection via short-distance droplets or sustained airborne aerosols. |
| None |
| Ahmed, et al., 2020 [42] | Cross-sectional Study | Setup: 669 dentists from 30 different countries. Context: Global | The present research measured distress and fear of infection among dentists operating during the current viral epidemic. In addition, the dentist’s information on various practice modifications in the battle against a novel coronavirus disease epidemic has been analyzed. |
| Information gathered over a concise span of time, keeping in mind the sudden effect this epidemic had on the mindset and dental professionals. Responses from all countries impacted by the outbreak were not received. Owing to the cross-sectional design of the research, we were unable to establish a cause-and-effect connection. |
| |||||
| Shacham, M. et al., 2020 [43] | Cross-sectional study | Setup: 338 Israeli dentists. Context: Israel. | The analysis examined the correlation of COVID-19 variables and psychological factors with psychological distress in dental workers during the outbreak of the COVID-19 pandemic. |
| Cross-section model, which precludes causal inferences. Low response rate. Selection bias and sampling error. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahdi, S.S.; Ahmed, Z.; Allana, R.; Peretti, A.; Amenta, F.; Nadeem Bijle, M.; Seow, L.L.; Daood, U. Pivoting Dental Practice Management during the COVID-19 Pandemic—A Systematic Review. Medicina 2020, 56, 644. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120644
Mahdi SS, Ahmed Z, Allana R, Peretti A, Amenta F, Nadeem Bijle M, Seow LL, Daood U. Pivoting Dental Practice Management during the COVID-19 Pandemic—A Systematic Review. Medicina. 2020; 56(12):644. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120644
Chicago/Turabian StyleMahdi, Syed Sarosh, Zohaib Ahmed, Raheel Allana, Alessandro Peretti, Francesco Amenta, Mohammed Nadeem Bijle, Liang Lin Seow, and Umer Daood. 2020. "Pivoting Dental Practice Management during the COVID-19 Pandemic—A Systematic Review" Medicina 56, no. 12: 644. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina56120644