
Multidisciplinary Approach to Suspected Sudden Death Caused by Arteriovenous Malformation Rupture: A Case Report


 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Circumstantial Data
2.2. Crime Scene Investigation
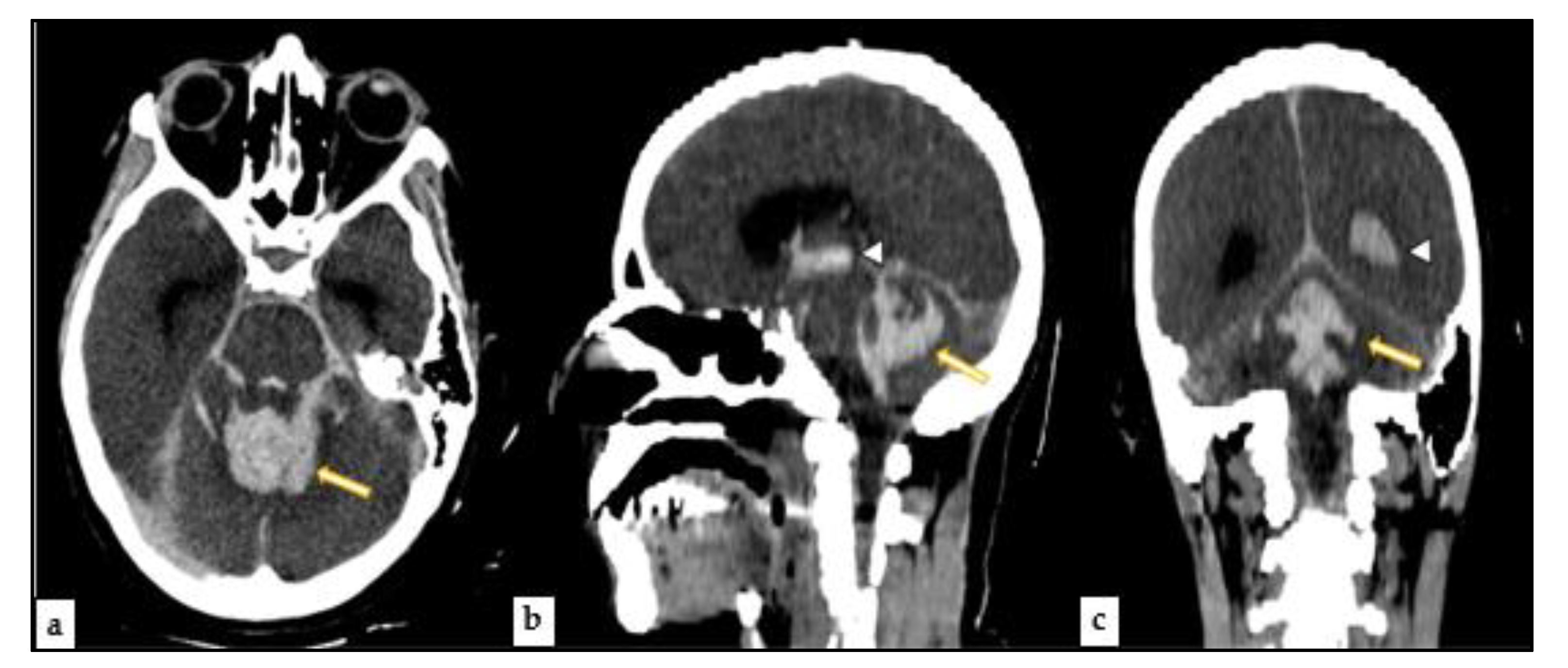
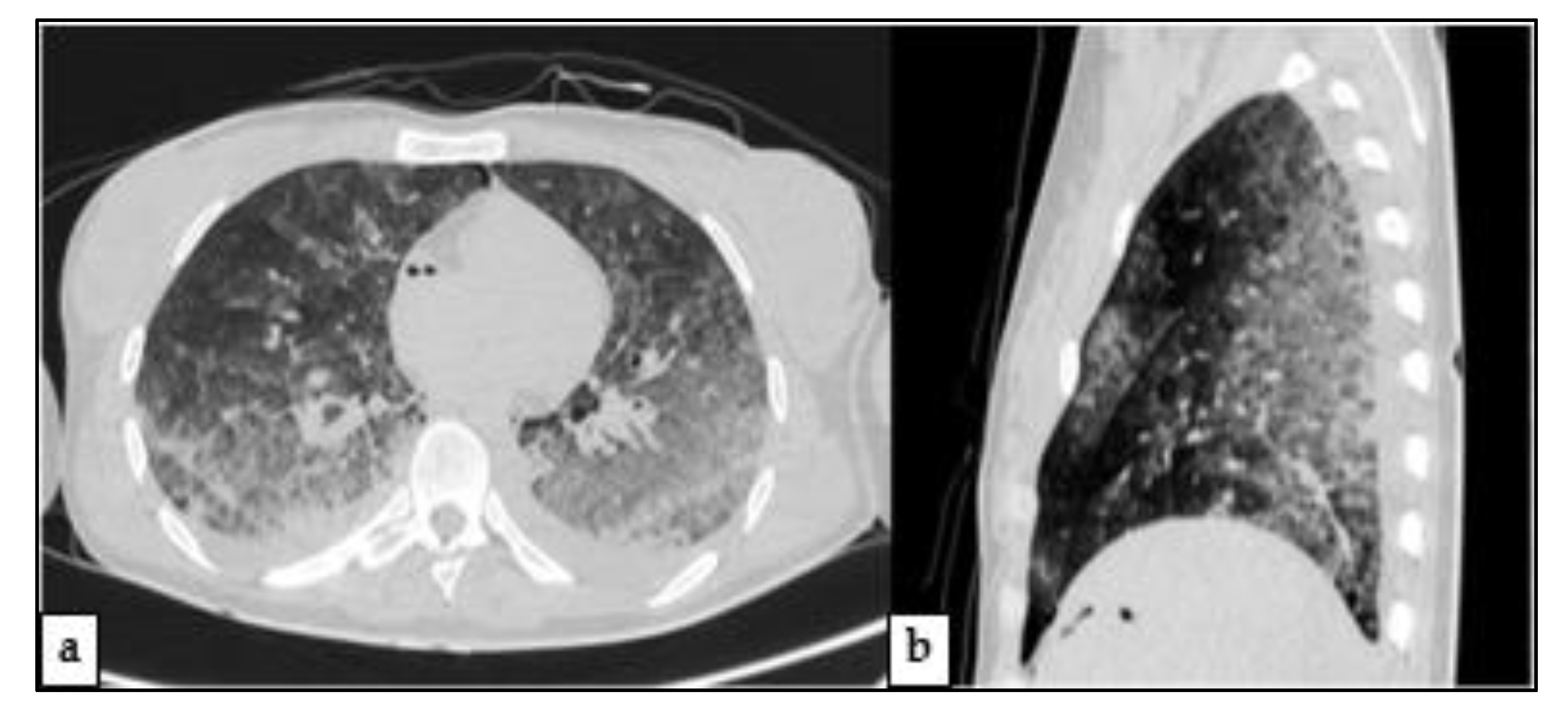
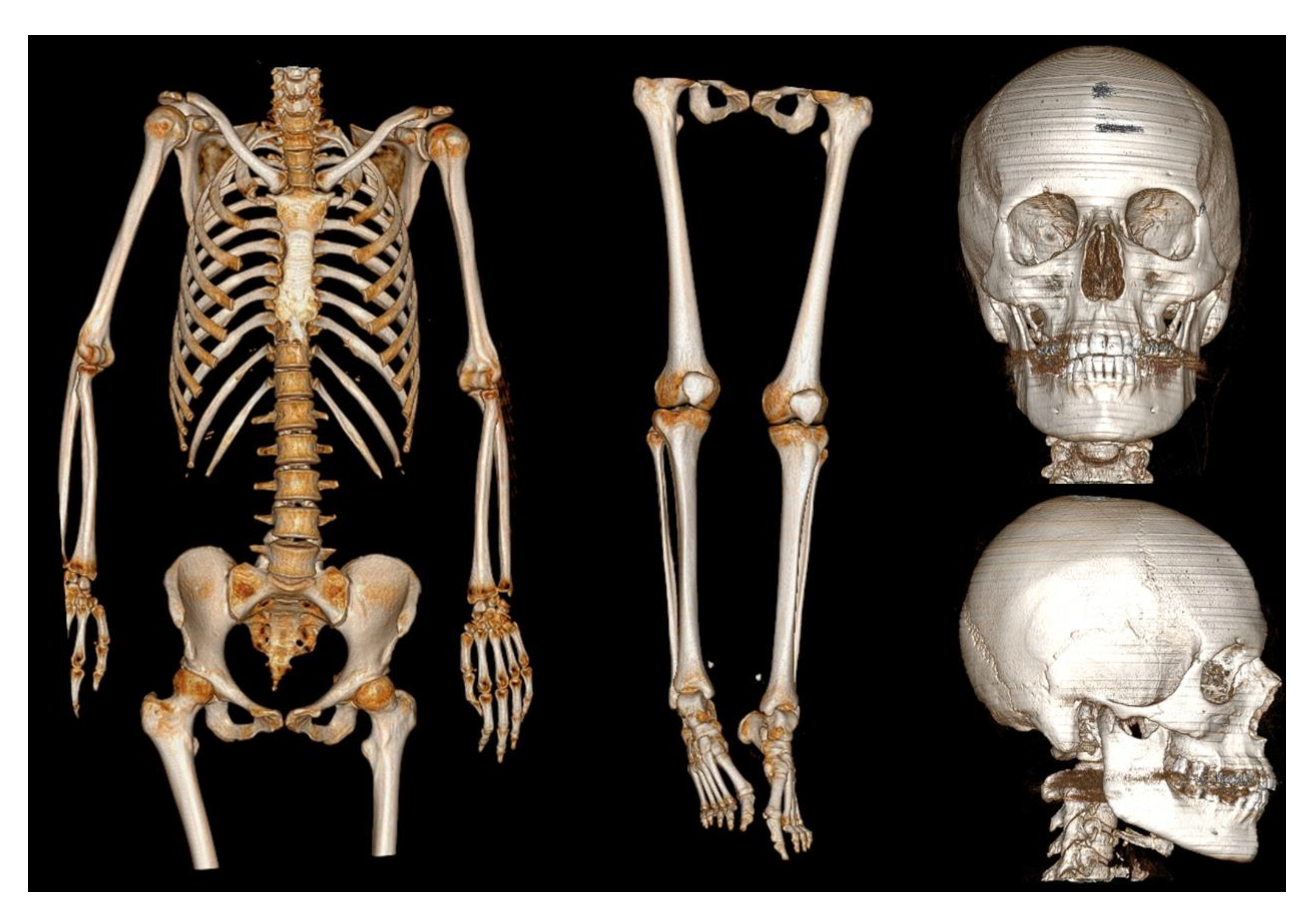
2.3. Post-Mortem Computed Tomography (PMCT)
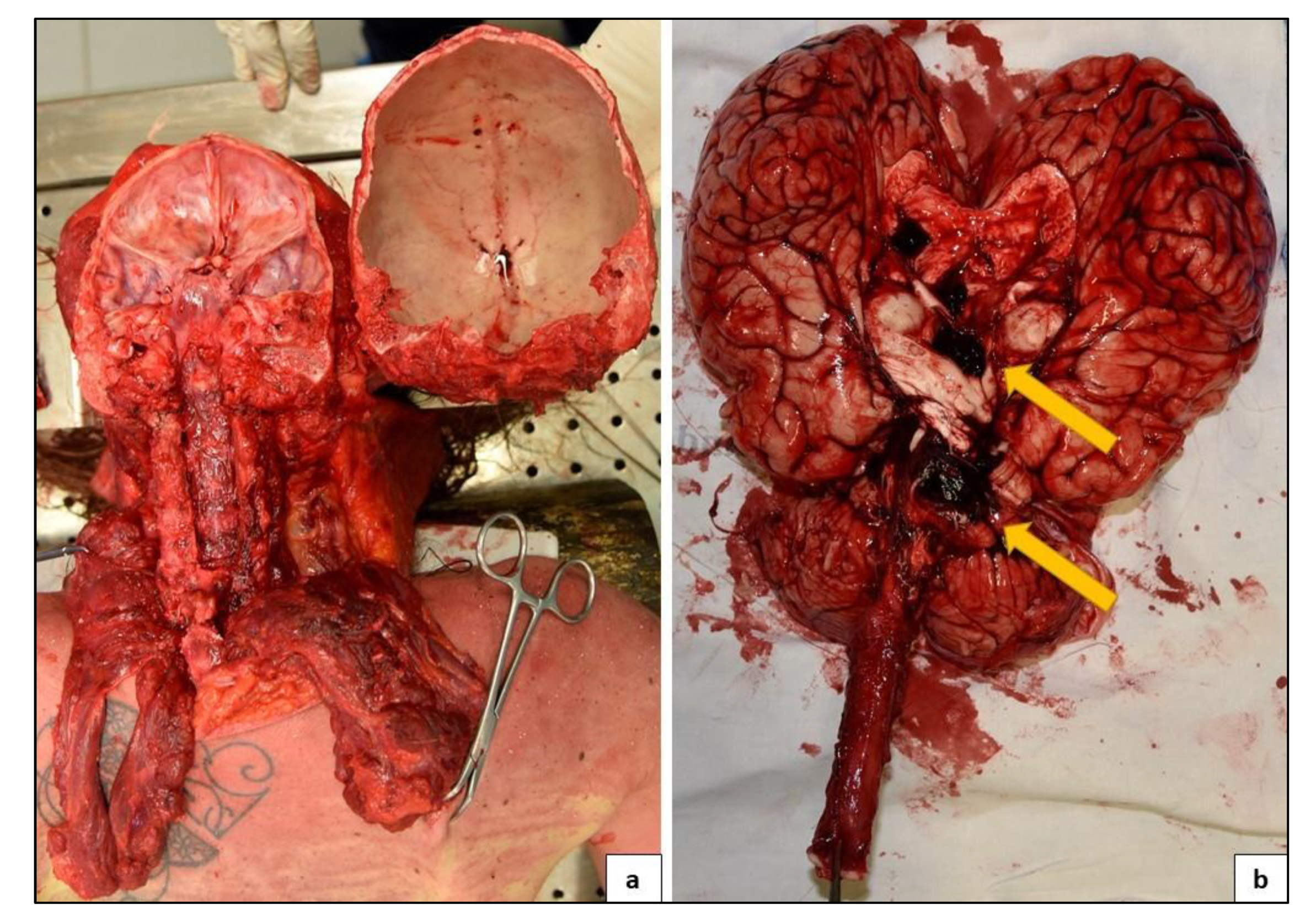
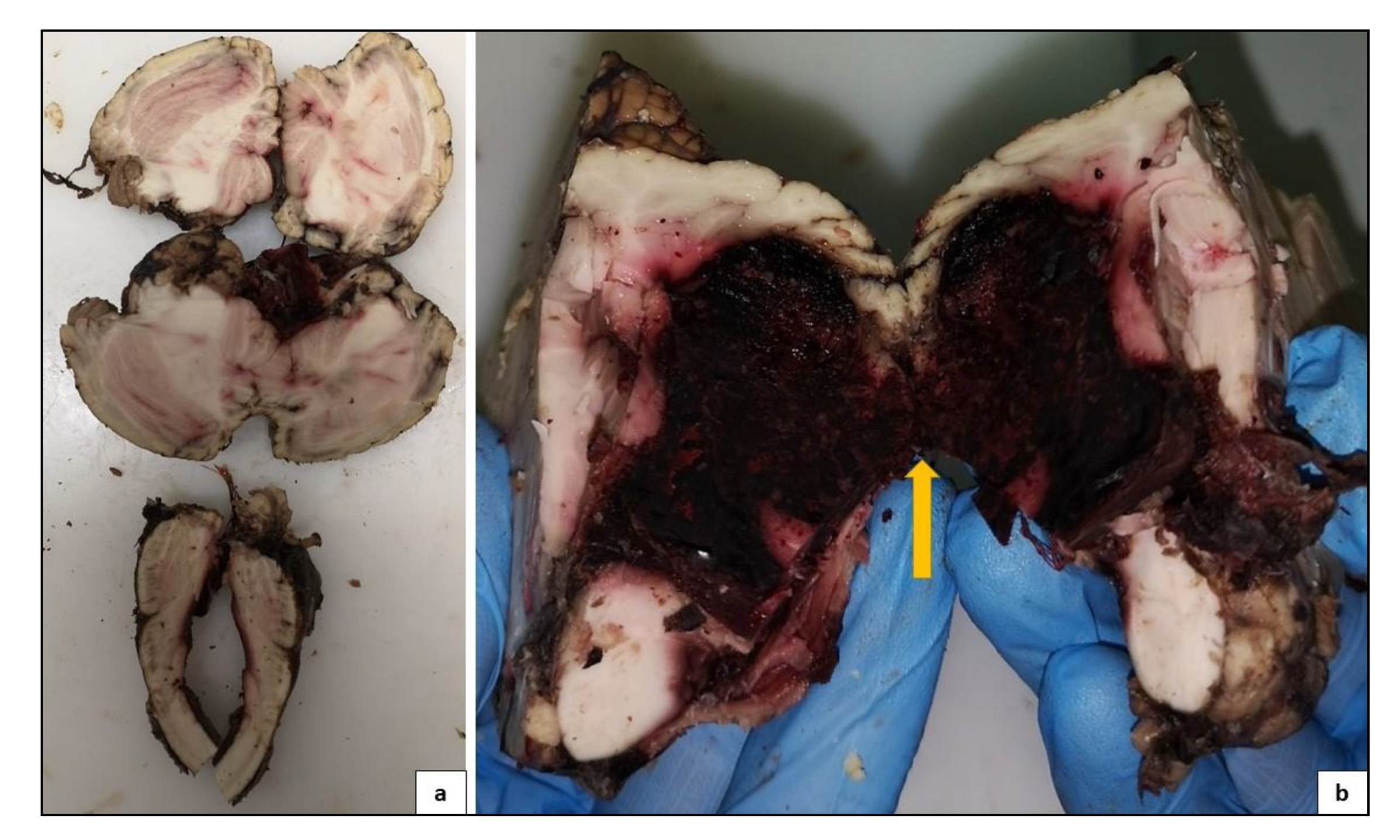
2.4. Autopsy
2.4.1. Technique
2.4.2. Central Nervous System Findings
2.4.3. Other Findings
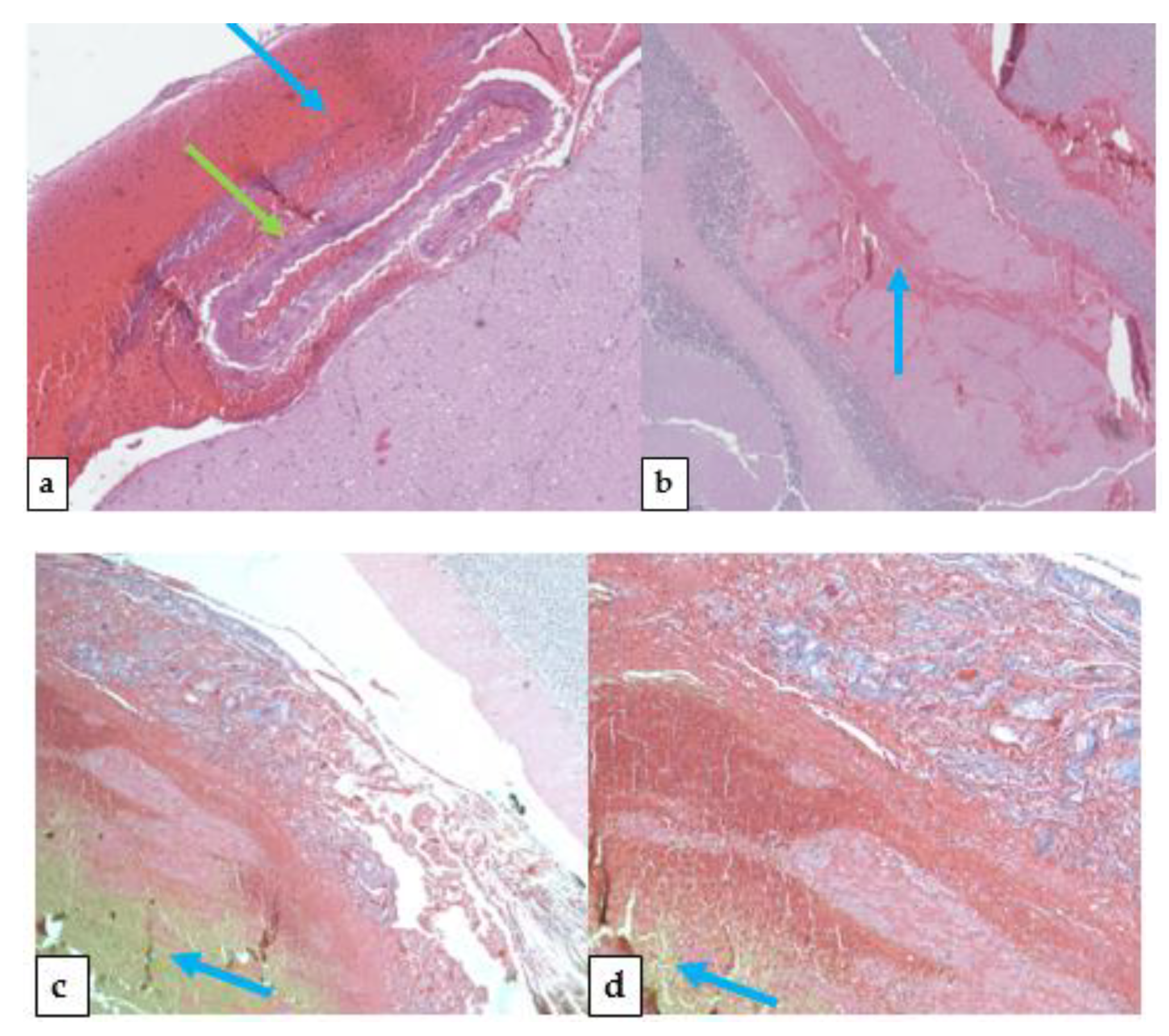
2.5. Histological Findings
2.6. Cause of Death
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ruíz-Sandoval, J.L.; Cantu, C.; Barinagarrementeria, F. Intracerebral hemorrhage in young people: Analysis of risk factors, location, causes, and prognosis. Stroke 1999, 30, 537–541. [Google Scholar] [CrossRef] [Green Version]
- Hernesniemi, J.A.; Dashti, R.; Juvela, S.; Väärt, K.; Niemelä, M.; Laakso, A. Natural history of brain arteriovenous malformations: A long-term follow-up study of risk of hemorrhage in 238 patients. Neurosurgery 2008, 63, 823–831. [Google Scholar] [CrossRef]
- Hillman, J. Population-based analysis of arteriovenous malformation treatment. J. Neurosurg. 2001, 95, 633–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauswald, H.; Milker-Zabel, S.; Sterzing, F.; Schlegel, W.; Debus, J.; Zabel-du Bois, A. Repeated linac-based radiosurgery in high-grade cerebral arteriovenous-malformations (AVM) Spetzler–Martin grade III to IV previously treated with radiosurgery. Radiother. Oncol. 2011, 98, 217–222. [Google Scholar] [CrossRef]
- Bokhari, M.R.; Bokhari, S.R.A. Arteriovenous Malformation of the Brain. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Berman, M.F.; Sciacca, R.R.; Pile-Spellman, J.; Stapf, C.; Connolly, E.S., Jr.; Mohr, J.P. The epidemiology of brain arteriovenous malformations. Neurosurgery 2000, 47, 389–397. [Google Scholar] [CrossRef]
- Stapf, C.; Mohr, J.P.; Pile-Spellman, J.; Solomon, R.A.; Sacco, R.L.; Connolly, E. Epidemiology and natural history of arteriovenous malformations. Neurosurg. Focus 2001, 11, 1–5. [Google Scholar] [CrossRef]
- McCormick, W.F. The pathology of vascular (“arteriovenous”) malformations. J. Neurosurg. 1966, 24, 807–816. [Google Scholar] [CrossRef]
- Brown, R.D., Jr.; Wiebers, D.O.; Torner, J.C.; O’Fallon, W.M. Frequency of intracranial hemorrhage as a presenting symptom and subtype analysis: A population-based study of intracranial vascular malformations in Olmsted County, Minnesota. J. Neurosurg. 1996, 85, 29–32. [Google Scholar] [CrossRef] [Green Version]
- Mast, H.; Mohr, J.P.; Osipov, A.; Pile-Spellman, J.; Marshall, R.S.; Lazar, R.M.; Stein, B.M.; Young, W.L. “Steal” is an unestablished mechanism for the clinical presentation of cerebral arteriovenous malformations. Stroke 1995, 26, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.G. Cerebral arteriovenous malformations: Considerations for and experience with surgical treatment in 166 cases. Clin. Neurosurg. 1979, 26, 145–208. [Google Scholar] [CrossRef] [PubMed]
- Stein, B.M.; Kader, A. Intracranial arteriovenous malformations. Clin. Neurosurg. 1992, 39, 76–113. [Google Scholar] [PubMed]
- Filograna, L.; Thali, M.J. Post-mortem CT imaging of the lungs: Pathological versus non-pathological findings. Radiol. Med. 2017, 122, 902–908. [Google Scholar] [CrossRef] [PubMed]
- WHO. International Classification of Diseases (ICD-10); World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Yeo, J.J.; Low, S.Y.; Seow, W.T.; Low, D.C. Pediatric de novo cerebral AVM: Report of two cases and review of literature. Child’s Nerv. Syst. 2015, 31, 609–614. [Google Scholar] [CrossRef]
- Rispoli, R.; Donati, L.; Bartolini, N.; Bolli, L.; Sulis, A.; Zofrea, G.; Passalacqua, G.P.; Carletti, S. Rupture of an intracranial arteriovenous malformation (AVM) in pregnancy: Case report. J. Stem Cell Res. Ther. 2015, 5, 2. [Google Scholar] [CrossRef]
- Trivedi, R.A.; Kirkpatrick, P.J. Arteriovenous malformations of the cerebral circulation that rupture in pregnancy. J. Obstet. Gynaecol. 2003, 23, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.J.; Wang, S.; Zhao, Y.L.; Teo, M.; Guo, P.; Zhang, D.; Wang, R.; Cao, Y.; Ye, X.; Kang, S.; et al. Risk of cerebral arteriovenous malformation rupture during pregnancy and puerperium. Neurology 2014, 82, 1798–1803. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, B.; Lindquist, C.; Steiner, L. Effect of Gamma Knife surgery on the risk of rupture prior to AVM obliteration. Minim. Invasive Neurosurg. 1996, 39, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Torné, R.; Rodríguez-Hernández, A.; Lawton, M.T. Intraoperative arteriovenous malformation rupture: Causes, management techniques, outcomes, and the effect of neurosurgeon experience. Neurosurg. Focus 2014, 37. [Google Scholar] [CrossRef]
- Gross, B.A.; Rose, D. Rate of re-bleeding of arteriovenous malformations in the first year after rupture. J. Clin. Neurosci. 2012, 19, 1087–1088. [Google Scholar] [CrossRef]
- Matschke, J.; Lockemann, U.; Schulz, F. Intracranial arteriovenous malformations presenting as sudden unexpected death: A report of 3 cases and review of the literature. Am. J. Forensic Med. Pathol. 2007, 28, 173–176. [Google Scholar] [CrossRef]
- Karhunen, P.J.; Penttilä, A.; Erkinjuntti, T. Arteriovenous malformation of the brain: Imaging by postmortem angiography. Forensic Sci. Int. 1990, 48, 9–19. [Google Scholar] [CrossRef]
- Rosen, R.S.; Armbrustmacher, V.; Sampson, B.A. Spontaneous cerebellar hemorrhage in children. J. Forensic Sci. 2003, 48, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, A.; Grech, J.L. Arteriovenous malformation of the cerebellum: A case report and its medicolegal implications. Forensic Sci. 1974, 4, 75–82. [Google Scholar] [CrossRef]
- Racette, S.; Sauvageau, A. Brain arteriovenous malformation and its implication in forensic pathology. J. Forensic Sci. 2007, 52, 189–191. [Google Scholar] [CrossRef]
- Cioca, A.; Gheban, D.; Perju-Dumbrava, D.; Chiroban, O.; Mera, M. Sudden death from ruptured choroid plexus arteriovenous malformation. Am. J. Forensic Med. Pathol. 2014, 35, 100–102. [Google Scholar] [CrossRef]
- Elfawal, M.A.; Haque, A. Trauma and arteriovenous malformation of the brain—A problem in medico-legal practice. J. Clin. Forensic Med. 1999, 6, 49–52. [Google Scholar] [CrossRef]
- Patanè, F.G.; Liberto, A.; Maglitto, A.N.M.; Malandrino, P.; Esposito, M.; Amico, F. Nandrolone Decanoate: Use, Abuse and Side Effects. Medicina 2020, 56, 606. [Google Scholar] [CrossRef] [PubMed]
- Torrisi, M.; Pennisi, G.; Russo, I.; Amico, F.; Esposito, M.; Liberto, A. Sudden Cardiac Death in Anabolic-Androgenic Steroid Users: A Literature Review. Medicina 2020, 56, 587. [Google Scholar] [CrossRef]
- Choi, J.H.; Mohr, J.P. Brain arteriovenous malformations in adults. Lancet Neurol. 2005, 4, 299–308. [Google Scholar] [CrossRef]
- Esposito, M.; Montana, A.; Liberto, A.; Filetti, V.; Nunno, N.D.; Amico, F.; Salerno, M.; Loreto, C.; Sessa, F. Anaphylactic Death: A New Forensic Workflow for Diagnosis. Healthcare 2021, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- Pomara, C.; Salerno, M.; Sessa, F.; Esposito, M.; Barchitta, M.; Ledda, C.; Grassi, P.; Liberto, A.; Mattaliano, A.R.; Rapisarda, V.; et al. Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases. Diagnostics 2021, 11, 457. [Google Scholar] [CrossRef] [PubMed]
- Pomara, C.; Sessa, F.; Ciaccio, M.; Dieli, F.; Esposito, M.; Giammanco, G.M.; Garozzo, S.F.; Giarratano, A.; Prati, D.; Rappa, F.; et al. COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis. Diagnostics 2021, 11, 955. [Google Scholar] [CrossRef] [PubMed]
- Tawfiq Zyoud, T.Y.; Abdul Rashid, S.N.; Suppiah, S.; Abdul Rahim, E.; Mahmud, R. Decoding death by unknown causes using post mortem image-guided virtopsy: A review of recent literature and the Malaysian experience. Med. J. Malays. 2020, 75, 411–418. [Google Scholar]
- Di Nunno, N.; Patanè, F.G.; Amico, F.; Asmundo, A.; Pomara, C. The role of a good quality autopsy in pediatric malpractice claim: A case report of an unexpected death in an undiagnosed thymoma. Front. Pediatr. 2020, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Maiellaro, A.; Perna, A.; Giugliano, P.; Esposito, M.; Vacchiano, G. Sudden Death from Primary Cerebral Melanoma: Clinical Signs and Pathological Observations. Healthcare 2021, 9, 341. [Google Scholar] [CrossRef]
- Montana, A.; Rapisarda, V.; Esposito, M.; Amico, F.; Cocimano, G.; Nunno, N.D.; Ledda, C.; Salerno, M. A Rare Case of Suicide by Ingestion of Phorate: A Case Report and a Review of the Literature. Healthcare 2021, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Albano, G.D.; Amico, F.; Cocimano, G.; Liberto, A.; Maglietta, F.; Esposito, M.; Rosi, G.L.; Di Nunno, N.; Salerno, M.; Montana, A. Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review. Healthcare 2021, 9, 97. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patanè, F.G.; Esposito, M.; Musumeci, A.G.; Palermo, M.; Torrisi, M.; Salerno, M.; Montana, A. Multidisciplinary Approach to Suspected Sudden Death Caused by Arteriovenous Malformation Rupture: A Case Report. Medicina 2021, 57, 644. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070644
Patanè FG, Esposito M, Musumeci AG, Palermo M, Torrisi M, Salerno M, Montana A. Multidisciplinary Approach to Suspected Sudden Death Caused by Arteriovenous Malformation Rupture: A Case Report. Medicina. 2021; 57(7):644. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070644
Chicago/Turabian StylePatanè, Federico Giuseppe, Massimiliano Esposito, Andrea Giovanni Musumeci, Monica Palermo, Marco Torrisi, Monica Salerno, and Angelo Montana. 2021. "Multidisciplinary Approach to Suspected Sudden Death Caused by Arteriovenous Malformation Rupture: A Case Report" Medicina 57, no. 7: 644. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57070644