
Clinical Phenotypes of Dual Kidney Transplant Recipients in the United States as Identified through Machine Learning Consensus Clustering

 ,
,  , , ,
, , ,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Data Collection
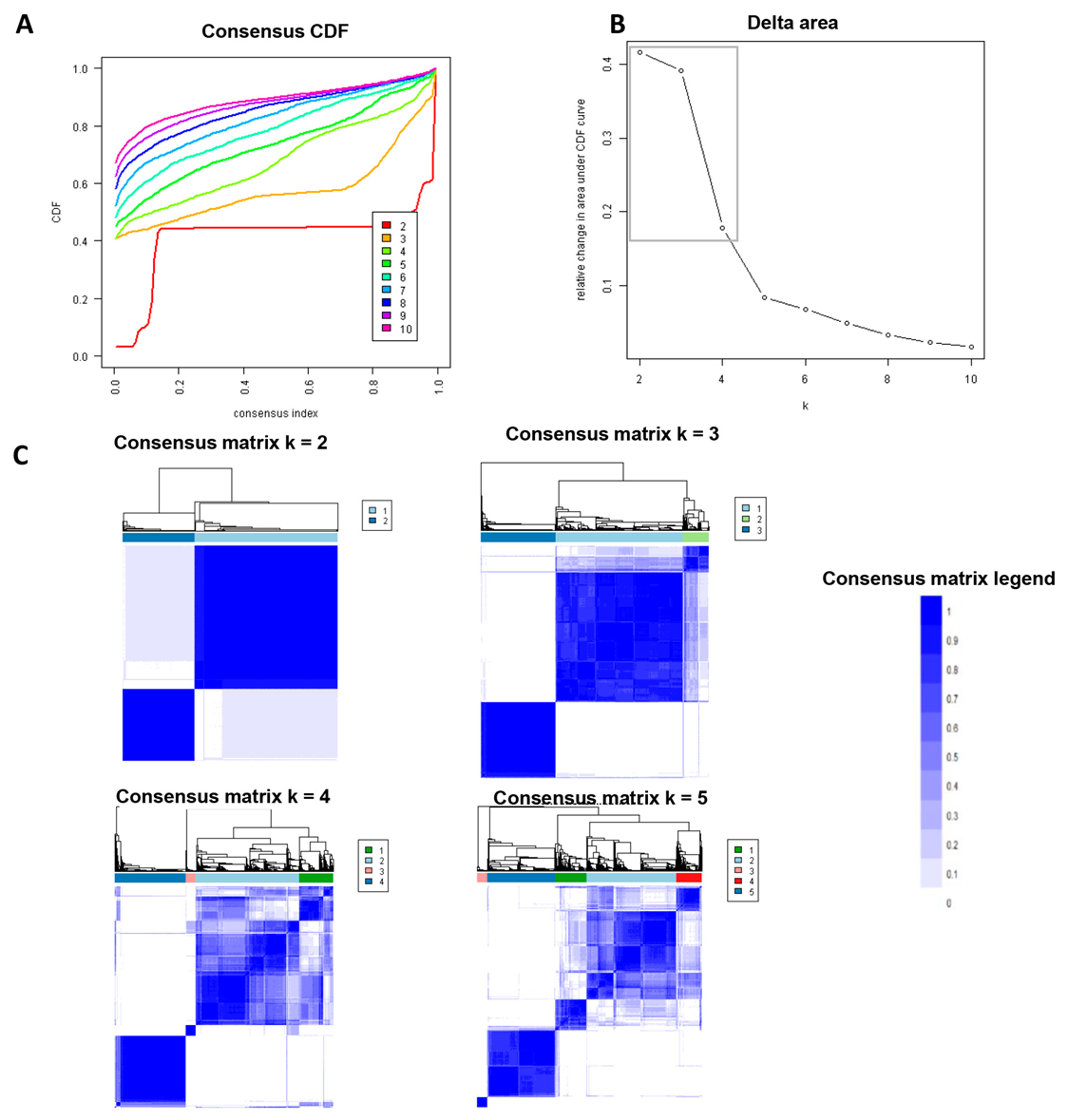
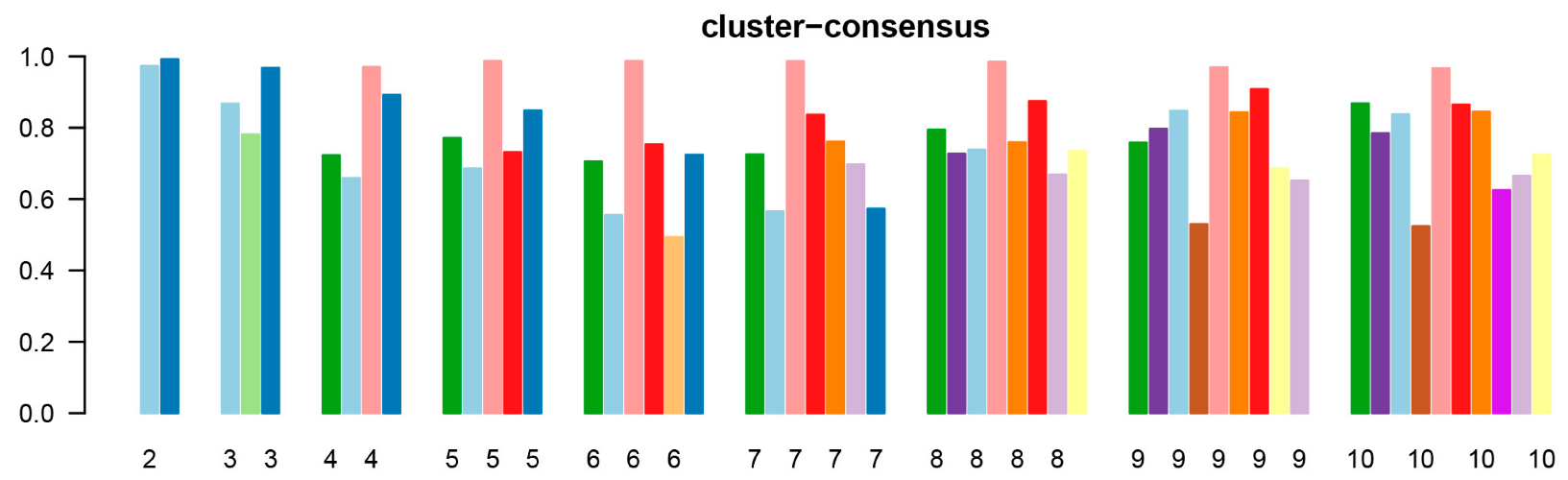
2.3. Clustering Analysis
2.4. Outcomes
2.5. Statistical Analysis
3. Results
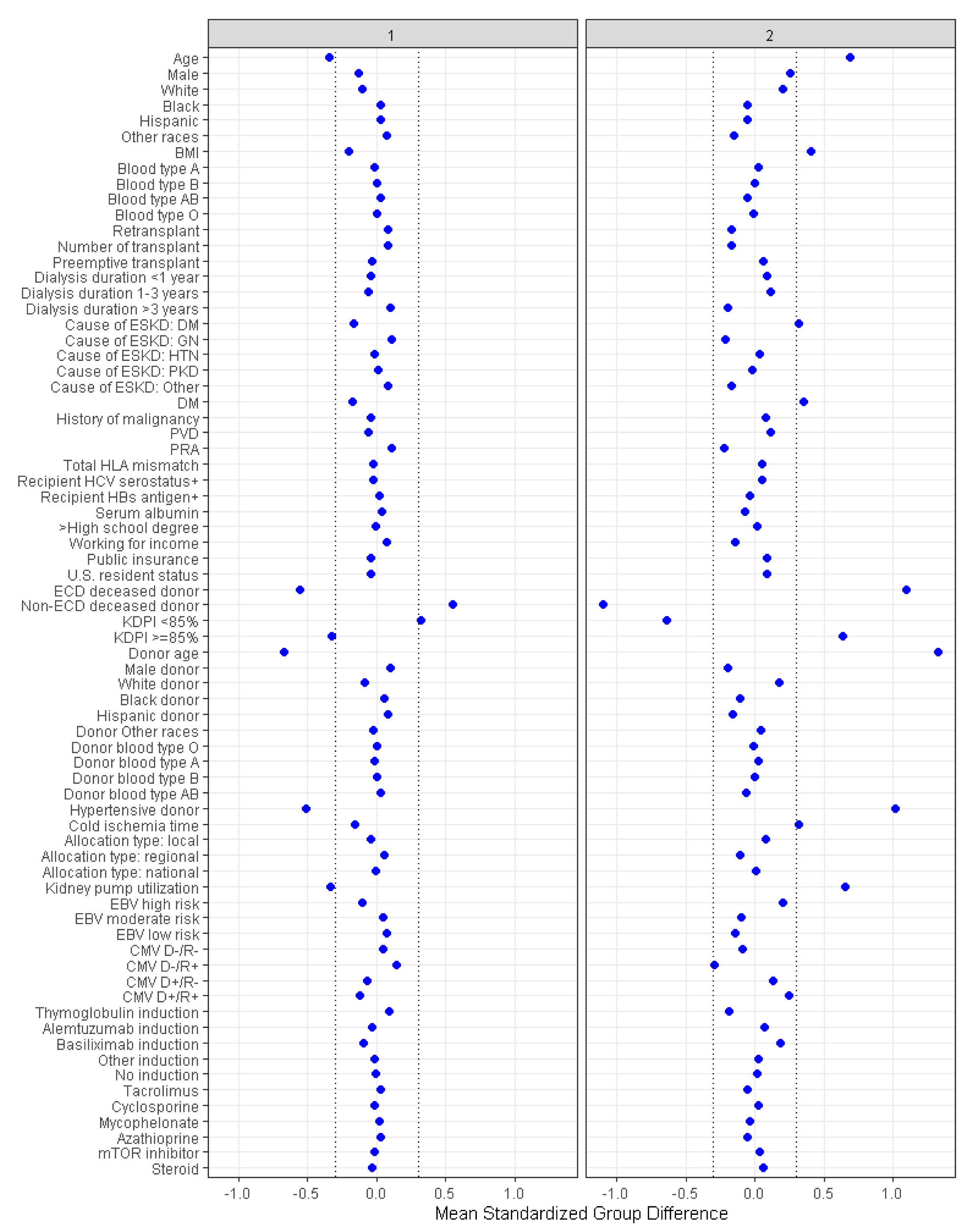
3.1. Characteristics of Each DKT Cluster
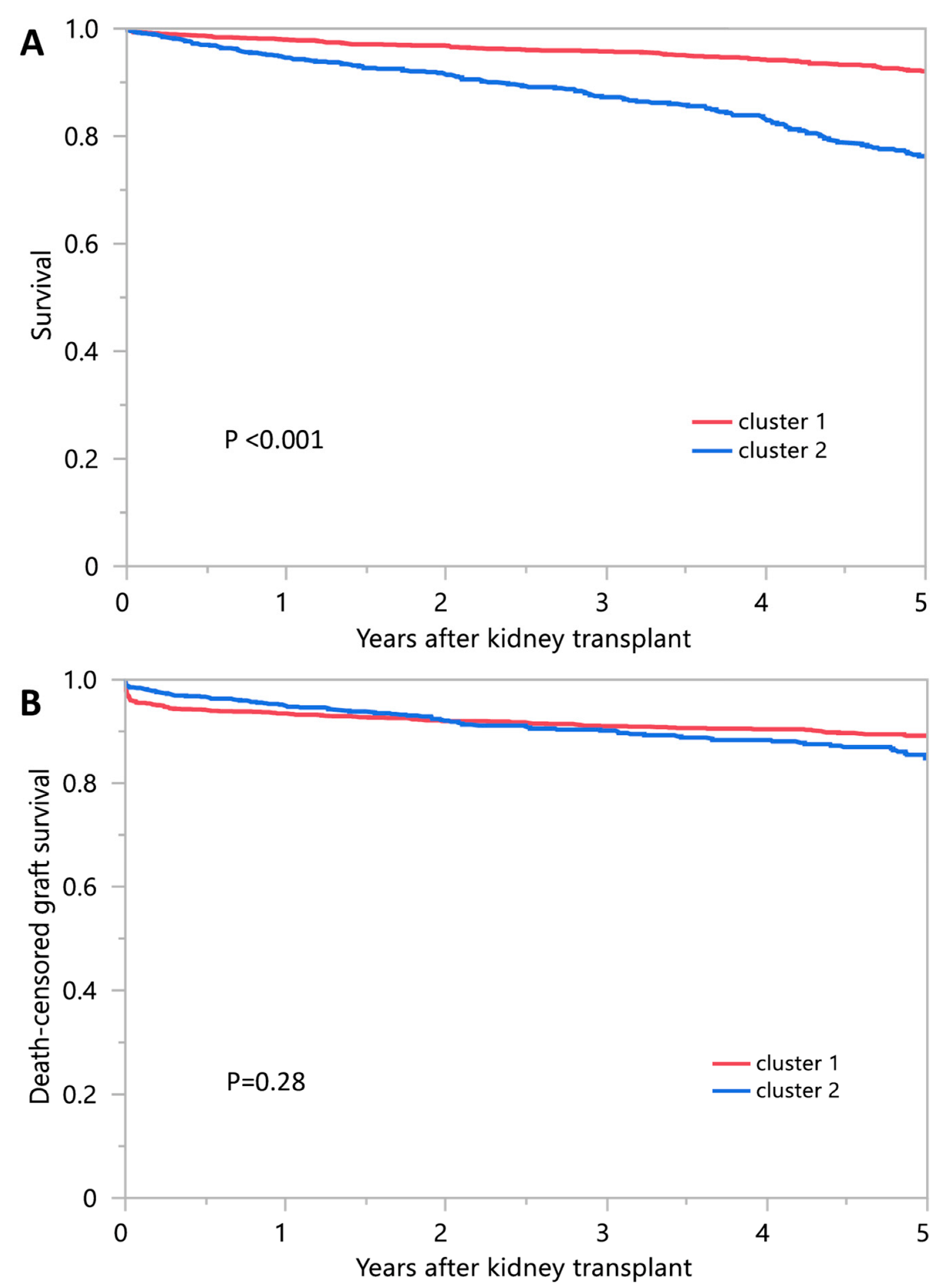
3.2. Post-Transplant Outcomes of Each DKT Clusters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia, G.G.; Harden, P.; Chapman, J. The global role of kidney transplantation. Indian J. Nephrol. 2012, 22, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic Review: Kidney Transplantation Compared with Dialysis in Clinically Relevant Outcomes. Am. J. Transplant. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Liao, M.; Wang, P.; Yang, Z.; Liu, Y. The Cost-Effectiveness of Kidney Replacement Therapy Modalities: A Systematic Review of Full Economic Evaluations. Appl. Health Econ. Health Policy 2020, 19, 163–180. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.S.; Messersmith, E.E.; Ratner, L.E.; Kochik, R.; Baliga, P.K.; Ojo, A.O. Organ Donation and Utilization in the United States, 1999–2008. Am. J. Transplant. 2010, 10, 973–986. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Roys, E.C.; Merion, R.M. Trends in Organ Donation and Transplantation in the United States, 1999-2008. Am. J. Transplant. 2010, 10, 961–972. [Google Scholar] [CrossRef] [Green Version]
- Israni, A.K.; Salkowski, N.; Gustafson, S.; Snyder, J.J.; Friedewald, J.J.; Formica, R.N.; Wang, X.; Shteyn, E.; Cherikh, W.; Stewart, D.; et al. New National Allocation Policy for Deceased Donor Kidneys in the United States and Possible Effect on Patient Outcomes. J. Am. Soc. Nephrol. 2014, 25, 1842–1848. [Google Scholar] [CrossRef] [Green Version]
- Stratta, R.J.; Harriman, D.; Gurram, V.; Gurung, K.; Sharda, B. Dual kidney transplants from adult marginal donors: Review and perspective. Clin. Transplant. 2021, 36, e14566. [Google Scholar] [CrossRef]
- Johnson, L.B.; Kuo, P.C.; Dafoe, D.C.; Schweitzer, E.J.; Alfrey, E.J.; Klassen, D.K.; Hoehn-Sarie, E.W.; Weir, M.R.; Bartlett, S.T. Double adult renal allografts: A technique for expansion of the cadaveric kidney donor pool. Surgery 1996, 120, 580–584. [Google Scholar] [CrossRef]
- Johnson, L.B.; Kuo, P.C.; Dafoe, D.C.; Drachenberg, C.B.; Schweitzer, E.J.; Alfrey, E.J.; Ridge, L.A.; Salvatierra, P.; Papadimitriou, J.C.; Mergner, W.J.; et al. The Use of Bilateral Adult Renal Allografts-A Method to Optimize Function from Donor Kidneys with Suboptimal Neph-ron Mass. Transplantation 1996, 61, 1261–1263. [Google Scholar] [CrossRef]
- Das, D.M.; Heilman, R.L.; Khamash, H.A.; Mathur, A.K.; Singer, A.L.; Reddy, K.S.; Jadlowiec, C.C. Overcoming Mismatch Concerns for Adult Recipients of Small Pediatric Deceased Donor Kidneys. Transplant. Proc. 2021, 53, 1509–1513. [Google Scholar] [CrossRef]
- Das, D.; Wagler, J.; Ohara, S.; Nguyen, M.; Frasco, P.E.; Smith, M.; Khamash, H.; Mathur, A.K.; Budhiraja, P.; Reddy, K.; et al. Outcomes of dual kidney transplants from high KDPI kidneys are superior compared to single kidney high KDPI transplants at 1 year. Clin. Transplant. 2022, 36, e14737. [Google Scholar] [CrossRef]
- Andrés, A.; Morales, J.M.; Herrero, J.C.; Praga, M.; Morales, E.; Hernández, E.; Ortuño, T.; Rodício, J.L.; A Martínez, M.; Usera, G.; et al. Double Versus Single Renal Allografts from Aged Donors. Transplantation 2000, 69, 2060–2066. [Google Scholar] [CrossRef]
- Bunnapradist, S.; Gritsch, H.A.; Peng, A.; Jordan, S.C.; Cho, Y.W. Dual Kidneys from Marginal Adult Donors as a Source for Cadaveric Renal Transplantation in the United States. J. Am. Soc. Nephrol. 2003, 14, 1031–1036. [Google Scholar] [CrossRef] [Green Version]
- De Serres, S.A.; Caumartin, Y.; Noël, R.; Lachance, J.-G.; Côté, I.; Naud, A.; Fradet, Y.; Mfarrej, B.G.; Agharazii, M.; Houde, I. Dual-Kidney Transplants as an Alternative for Very Marginal Donors: Long-Term Follow-Up in 63 Patients. Transplantation 2010, 90, 1125–1130. [Google Scholar] [CrossRef]
- Fernández-Lorente, L.; Riera, L.; Bestard, O.; Carrera, M.; Gomà, M.; Porta, N.; Torras, J.; Melilli, E.; Gil-Vernet, S.; Grinyó, J.M.; et al. Long-Term Results of Biopsy-Guided Selection and Allocation of Kidneys from Older Donors in Older Recipients. Am. J. Transplant. 2012, 12, 2781–2788. [Google Scholar] [CrossRef]
- Gill, J.; Cho, Y.W.; Danovitch, G.M.; Wilkinson, A.; Lipshutz, G.; Pham, P.-T.; Gill, J.S.; Shah, T.; Bunnapradist, S. Outcomes of Dual Adult Kidney Transplants in the United States: An Analysis of the OPTN/UNOS Database. Transplantation 2008, 85, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Impedovo, S.; de Lorenzis, E.; Volpe, A.; Gesualdo, L.; Grandaliano, G.; Palazzo, S.; Lucarelli, G.; Bettocchi, C.; Terrone, C.; Stratta, P.; et al. Middle and Long-term Outcomes of Dual Kidney Transplant: A Multicenter Experience. Transplant. Proc. 2013, 45, 1237–1241. [Google Scholar] [CrossRef]
- Sefora, P.E.; Silvio, S.; Nicola, D.F.; Giuseppe, R.; Iris, F.; Luigino, B.; Maria, G.; Eliana, G.; Donato, D.; Enrico, M.; et al. Optimizing utilization of kidneys from deceased donors over 60 years: Five-year outcomes after implementation of a combined clinical and histological allocation algorithm. Transpl. Int. 2013, 26, 833–841. [Google Scholar] [CrossRef]
- Remuzzi, G.; Cravedi, P.; Perna, A.; Dimitrov, B.D.; Turturro, M.; Locatelli, G.; Rigotti, P.; Baldan, N.; Beatini, M.; Valente, U.; et al. Long-Term Outcome of Renal Transplantation from Older Donors. N. Engl. J. Med. 2006, 354, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Rigotti, P.; Capovilla, G.; Di Bella, C.; Silvestre, C.; Donato, P.; Baldan, N.; Furian, L. A single-center experience with 200 dual kidney transplantations. Clin. Transplant. 2014, 28, 1433–1440. [Google Scholar] [CrossRef]
- Snanoudj, R.; Timsit, M.-O.; Rabant, M.; Tinel, C.; Lazareth, H.; Lamhaut, L.; Martinez, F.; Legendre, C. Dual Kidney Transplantation. Transplantation 2017, 101, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Tanriover, B.; Mohan, S.; Cohen, D.J.; Radhakrishnan, J.; Nickolas, T.L.; Stone, P.W.; Tsapepas, D.S.; Crew, R.J.; Dube, G.K.; Sandoval, P.R.; et al. Kidneys at Higher Risk of Discard: Expanding the Role of Dual Kidney Transplantation. Am. J. Transplant. 2014, 14, 404–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bresnahan, B.A.; McBride, M.A.; Cherikh, W.S.; Hariharan, S. Risk factors for renal allograft survival from pediatric cadaver donors: An analysis of united network for organ sharing data1. Transplantation 2001, 72, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Aawsaj, Y.; Dosani, T.; Talbot, D. Dual Kidney Transplantation: A Single-Center Experience. Transplant. Proc. 2015, 47, 1125–1127. [Google Scholar] [CrossRef] [PubMed]
- Boggi, U.; Barsotti, M.; Collini, A.; Bernini, M.; Vistoli, F.; Paleologo, G.; Bianchi, A.; Tregnaghi, C.; Nerucci, B.; Ruggieri, G.; et al. Kidney Transplantation from Donors Aged 65 Years or More as Single or Dual Grafts. Transplant. Proc. 2005, 37, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Casati, C.; Colombo, V.G.; Perrino, M.; Rossetti, O.M.; Querques, M.; Giacomoni, A.; Binaggia, A.; Colussi, G. Renal Transplants from Older Deceased Donors: Use of Preimplantation Biopsy and Differential Allocation to Dual or Single Kidney Transplant according to Histological Score Has No Advantages over Allocation to Single Kidney Transplant by Simple Clinical Indication. J. Transplant. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- De Paolis, P.; Colonnelli, R.; Favarò, A.; Salem, F.; Vignally, P.; Carriero, C.; Iappelli, M.; Di Giulio, S. Expanded Criteria Donor Kidney Transplantation: Comparative Outcome Evaluation Between Single Versus Double Kidney Transplantation at 8 Years: A Single Center Experience. Transplant. Proc. 2016, 48, 329–332. [Google Scholar] [CrossRef]
- Dietl, K.-H.; Wolters, H.; Marschall, B.; Senninger, N.; Heidenreich, S. Cadaveric “two-in-one” kidney transplantation from marginal donors: Experience of 26 cases after 3 years. Transplantation 2000, 70, 790–794. [Google Scholar] [CrossRef]
- Furian, L.; Baldan, N.; Margani, G.; Ekser, B.; Silvestre, C.; Marchini, F.; Bonfante, L.; Rossi, B.; Valente, M.; Rigotti, P. Calcineurin inhibitor-free immunosuppression in dual kidney transplantation from elderly donors. Clin. Transplant. 2007, 21, 57–62. [Google Scholar] [CrossRef]
- Johnson, A.P.; Price, T.P.; Lieby, B.; Doria, C. Dual Kidney Allocation Score: A Novel Algorithm Utilizing Expanded Donor Criteria for the Allocation of Dual Kidneys in Adults. Ann. Transplant. 2016, 21, 565–576. [Google Scholar] [CrossRef]
- Klair, T.; Gregg, A.; Phair, J.; Kayler, L.K. Outcomes of Adult Dual Kidney Transplants by KDRI in the United States. Am. J. Transplant. 2013, 13, 2433–2440. [Google Scholar] [CrossRef]
- Lee, K.W.; Park, J.B.; Cha, S.R.; Lee, S.H.; Chung, Y.J.; Yoo, H.; Kim, K.; Kim, S.J. Dual kidney transplantation offers a safe and effective way to use kidneys from deceased donors older than 70 years. BMC Nephrol. 2020, 21, 3. [Google Scholar] [CrossRef] [Green Version]
- Mallon, D.H.; Riddiough, G.E.; Summers, D.M.; Butler, A.J.; Callaghan, C.J.; Bradbury, L.L.; Bardsley, V.; Broecker, V.; Saeb-Parsy, K.; Torpey, N.; et al. Successful Transplantation of Kidneys from Elderly Circulatory Death Donors by Using Microscopic and Macroscopic Characteristics to Guide Single or Dual Implantation. Am. J. Transplant. 2015, 15, 2931–2939. [Google Scholar] [CrossRef]
- Perico, N.; Ruggenenti, P.; Scalamogna, M.; Locatelli, G.; Remuzzi, G. One or two marginal organs for kidney transplantation? Transplant. Proc. 2002, 34, 3091–3096. [Google Scholar] [CrossRef]
- Remuzzi, G.; Grinyò, J.; Ruggenenti, P.; Beatini, M.; Cole, E.H.; Milford, E.L.; Brenner, B.M. Early Experience with Dual Kidney Transplantation in Adults using Expanded Donor Criteria. J. Am. Soc. Nephrol. 1999, 10, 2591–2598. [Google Scholar] [CrossRef]
- Remuzzi, G.; Ruggenenti, P.; Ruggenenti, P. Renal transplantation: Single or dual for donors aging ≥60 years? Transplantation 2000, 69, 2000–2001. [Google Scholar] [CrossRef]
- Rigotti, P.; Cadrobbi, R.; Furian, L.; Baldan, N.; Sarzo, G.; Liberati, L.; Valente, M.; Ancona, E. Short-term outcome of dual kidney transplantation at a single center. Transplant. Proc. 2001, 33, 3771–3773. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Silvestre, C.; Boschiero, L.; Rota, G.; Furian, L.; Perna, A.; Rossini, G.; Remuzzi, G.; Rigotti, P. Long-term outcome of renal transplantation from octogenarian donors: A multicenter controlled study. Am. J. Transplant. 2017, 17, 3159–3171. [Google Scholar] [CrossRef] [Green Version]
- Snanoudj, R.; Rabant, M.; Timsit, M.O.; Karras, A.; Savoye, E.; Tricot, L.; Loupy, A.; Hiesse, C.; Zuber, J.; Kreis, H.; et al. Donor-Estimated GFR as an Appropriate Criterion for Allocation of ECD Kidneys into Single or Dual Kidney Transplantation. Am. J. Transplant. 2009, 9, 2542–2551. [Google Scholar] [CrossRef]
- Wolters, H.H.; Palmes, D.; Heidenreich, S.; August, C.; Brockmann, J.; Senninger, N.; Dietl, K.-H. Long-term follow-up of double kidney transplantation using a score for evaluation of marginal donors*. Transpl. Int. 2005, 18, 453–457. [Google Scholar] [CrossRef]
- Ershoff, B.D.; Lee, C.K.; Wray, C.L.; Agopian, V.G.; Urban, G.; Baldi, P.; Cannesson, M. Training and Validation of Deep Neural Networks for the Prediction of 90-Day Post-Liver Transplant Mortality Using UNOS Registry Data. Transplant. Proc. 2020, 52, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Mao, S.A.; Jadlowiec, C.C.; Mao, M.A.; Leeaphorn, N.; Kaewput, W.; Vaitla, P.; Pattharanitima, P.; Tangpanithandee, S.; Krisanapan, P.; et al. Machine Learning Consensus Clustering of Morbidly Obese Kidney Transplant Recipients in the United States. J. Clin. Med. 2022, 11, 3288. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Vaitla, P.; Jadlowiec, C.C.; Leeaphorn, N.; Mao, S.A.; Mao, M.A.; Pattharanitima, P.; Bruminhent, J.; Khoury, N.J.; Garovic, V.D.; et al. Use of Machine Learning Consensus Clustering to Identify Distinct Subtypes of Black Kidney Transplant Recipients and Associated Outcomes. JAMA Surg. 2022, 157, e221286. [Google Scholar] [CrossRef] [PubMed]
- Monti, S.; Tamayo, P.; Mesirov, J.; Golub, T. Consensus Clustering: A Resampling-Based Method for Class Discovery and Visualization of Gene Expression Microarray Data. Mach. Learn. 2003, 52, 91–118. [Google Scholar] [CrossRef]
- MacEachern, S.J.; Forkert, N.D. Machine learning for precision medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef]
- Alyousef, A.A.; Nihtyanova, S.; Denton, C.; Bosoni, P.; Bellazzi, R.; Tucker, A. Nearest Consensus Clustering Classification to Identify Subclasses and Predict Disease. J. Health Inform. Res. 2018, 2, 402–422. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Jadlowiec, C.C.; Kaewput, W.; Vaitla, P.; Mao, S.A.; Mao, M.A.; Leeaphorn, N.; Qureshi, F.; Pattharanitima, P.; Qureshi, F.; et al. Distinct Phenotypes of Kidney Transplant Recipients in the United States with Limited Functional Status as Identified through Machine Learning Consensus Clustering. J. Pers. Med. 2022, 12, 859. [Google Scholar] [CrossRef]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Wilkerson, M.D.; Hayes, D.N. ConsensusClusterPlus: A class discovery tool with confidence assessments and item tracking. Bioinformatics 2010, 26, 1572–1573. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A. Allocation of Dual and En Bloc Kidneys Two Year Post-Implementation Monitoring Report; OPTN Kidney Transplantation Committee: 21 March 2022. Available online: https://optn.transplant.hrsa.gov/media/33faxsvb/data_report_kidney_full_20220321_508_remediated.pdf (accessed on 5 October 2022).
- Sharma, A.; Fisher, R.A.; Cotterell, A.H.; King, A.L.; Maluf, D.G.; Posner, M.P. En Bloc Kidney Transplantation from Pediatric Donors: Comparable Outcomes with Living Donor Kidney Transplantation. Transplantation 2011, 92, 564–569. [Google Scholar] [CrossRef]
- Jannat-Khah, D.P.; Unterbrink, M.; McNairy, M.; Pierre, S.; Fitzgerald, D.W.; Pape, J.; Evans, A. Treating loss-tofollow-up as a missing data problem: A case study using a longitudinal cohort of HIV-infected patients in Haiti. BMC Public Health 2018, 18, 1269. [Google Scholar] [CrossRef] [Green Version]
- Knol, M.J.; Janssen, K.J.; Donders, A.R.; Egberts, A.C.; Heerdink, E.R.; Grobbee, D.E.; Moons, K.G.; Geerlings, M.I. Unpredictable bias when using the missing indicator method or complete case analysis for missing confounder values: An empirical example. J. Clin. Epidemiol. 2010, 63, 728–736. [Google Scholar] [CrossRef]
- White, I.R.; Carlin, J.B. Bias and efficiency of multiple imputation compared with complete-case analysis for missing covariate values. Stat. Med. 2010, 29, 2920–2931. [Google Scholar] [CrossRef]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Hedden, S.L.; Woolson, R.F.; Carter, R.E.; Palesch, Y.; Upadhyaya, H.P.; Malcolm, R.J. The impact of loss to follow up on hypothesis tests of the treatment effect for several statistical methods in substance abuse clinical trials. J. Subst. Abuse Treat. 2009, 37, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Donders, A.R.T.; Van Der Heijden, G.J.; Stijnen, T.; Moons, K.G. A gentle introduction to imputation of missing values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef]
- Șenbabaoğlu, Y.; Michailidis, G.; Li, J.Z. Critical limitations of consensus clustering in class discovery. Sci. Rep. 2014, 4, 6207. [Google Scholar] [CrossRef] [Green Version]
- Pattharanitima, P.; Thongprayoon, C.; Petnak, T.; Srivali, N.; Gembillo, G.; Kaewput, W.; Chesdachai, S.; Vallabhajosyula, S.; O’Corragain, O.A.; Mao, M.A.; et al. Machine Learning Consensus Clustering Approach for Patients with Lactic Acidosis in Intensive Care Units. J. Pers. Med. 2021, 11, 1132. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Dumancas, C.Y.; Nissaisorakarn, V.; Keddis, M.T.; Kattah, A.G.; Pattharanitima, P.; Petnak, T.; Vallabhajosyula, S.; Garovic, V.D.; Mao, M.A.; et al. Machine Learning Consensus Clustering Approach for Hospitalized Patients with Phosphate Derangements. J. Clin. Med. 2021, 10, 4441. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Hansrivijit, P.; Mao, M.A.; Vaitla, P.K.; Kattah, A.G.; Pattharanitima, P.; Vallabhajosyula, S.; Nissaisorakarn, V.; Petnak, T.; Keddis, M.T.; et al. Machine Learning Consensus Clustering of Hospitalized Patients with Admission Hyponatremia. Diseases 2021, 9, 54. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kattah, A.G.; Mao, M.A.; Keddis, M.T.; Pattharanitima, P.; Vallabhajosyula, S.; Nissaisorakarn, V.; Erickson, S.B.; Dillon, J.J.; Garovic, V.D.; et al. Distinct phenotypes of hospitalized patients with hyperkalemia by machine learning consensus clustering and associated mortality risks. QJM Int. J. Med. 2022, 115, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Mao, M.A.; Kattah, A.G.; Keddis, M.T.; Pattharanitima, P.; Erickson, S.B.; Dillon, J.J.; Garovic, V.D.; Cheungpasitporn, W. Subtyping hospitalized patients with hypokalemia by machine learning consensus clustering and associated mortality risks. Clin. Kidney J. 2022, 15, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Mao, M.A.; Keddis, M.T.; Kattah, A.G.; Chong, G.Y.; Pattharanitima, P.; Nissaisorakarn, V.; Garg, A.K.; Erickson, S.B.; Dillon, J.J.; et al. Hypernatremia subgroups among hospitalized patients by machine learning consensus clustering with different patient survival. J. Nephrol. 2022, 35, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Nissaisorakarn, V.; Pattharanitima, P.; Mao, M.A.; Kattah, A.G.; Keddis, M.T.; Dumancas, C.Y.; Vallabhajosyula, S.; Petnak, T.; Erickson, S.B.; et al. Subtyping Hyperchloremia among Hospitalized Patients by Machine Learning Consensus Clustering. Medicina 2021, 57, 903. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Sy-Go, J.P.T.; Nissaisorakarn, V.; Dumancas, C.Y.; Keddis, M.T.; Kattah, A.G.; Pattharanitima, P.; Vallabhajosyula, S.; Mao, M.A.; Qureshi, F.; et al. Machine Learning Consensus Clustering Approach for Hospitalized Patients with Dysmagnesemia. Diagnostics 2021, 11, 2119. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Vaitla, P.; Nissaisorakarn, V.; Mao, M.A.; Genovez, J.L.Z.; Kattah, A.G.; Pattharanitima, P.; Vallabhajosyula, S.; Keddis, M.T.; Qureshi, F.; et al. Clinically Distinct Subtypes of Acute Kidney Injury on Hospital Admission Identified by Machine Learning Consensus Clustering. Med. Sci. 2021, 9, 60. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 2821) | Cluster 1 (n = 1875) | Cluster 2 (n = 946) | p-Value | |
|---|---|---|---|---|
| Recipient Age (year) | 53.7 ± 13.8 | 48.9 ± 13.4 | 63.2 ± 8.8 | <0.001 |
| Recipient male sex | 1511 (54) | 882 (47) | 629 (66) | <0.001 |
| Recipient race | <0.001 | |||
| 1038 (37) | 596 (32) | 442 (47) | |
| 815 (29) | 565 (30) | 250 (26) | |
| 494 (18) | 346 (18) | 148 (16) | |
| 474 (17) | 368 (20) | 106 (11) | |
| ABO blood group | 0.239 | |||
| 955 (34) | 621 (33) | 334 (35) | |
| 431 (15) | 287 (15) | 144 (15) | |
| 144 (5) | 106 (6) | 38 (4) | |
| 1291 (46) | 861 (46) | 430 (45) | |
| Body mass index (kg/m2) | 26.2 ± 4.7 | 25.3 ± 4.4 | 28.2 ± 4.8 | <0.001 |
| Kidney retransplant | 131 (4.6) | 120 (6) | 11 (1) | <0.001 |
| Dialysis duration | <0.001 | |||
| 297 (11) | 180 (10) | 117 (12) | |
| 308 (11) | 179 (10) | 129 (14) | |
| 809 (29) | 489 (26) | 320 (34) | |
| 1407 (50) | 1027 (55) | 380 (40) | |
| Cause of ESKD | <0.001 | |||
| 746 (26) | 362 (19) | 384 (41) | |
| 738 (26) | 477 (25) | 261 (28) | |
| 626 (22) | 499 (27) | 127 (13) | |
| 232 (8) | 159 (8) | 73 (8) | |
| 479 (17) | 378 (20) | 101 (11) | |
| Comorbidity | ||||
| 920 (33) | 455 (24) | 465 (49) | <0.001 |
| 233 (8) | 135 (7) | 98 (10) | 0.004 |
| 214 (8) | 113 (6) | 101 (11) | <0.001 |
| Panel reactive antibody, median (IQR) | 0 (0, 11) | 0 (0, 23) | 0 (0, 0) | <0.001 |
| Positive Hepatitis C virus serostatus | 97 (3) | 55 (3) | 42 (4) | 0.038 |
| Positive Hepatitis B surface antigen | 64 (2) | 48 (3) | 16 (2) | 0.144 |
| Positive Human immunodeficiency virus serostatus | 28 (1) | 22 (1) | 6 (1) | 0.173 |
| Functional status | 0.267 | |||
| 7 (0) | 5 (0) | 2 (0.21) | |
| 1116 (40) | 722 (39) | 394 (42) | |
| 1698 (60) | 1148 (61) | 550 (58) | |
| Working income | 771 (27) | 571 (30) | 200 (21) | <0.001 |
| Public insurance | 2125 (75) | 1376 (73) | 749 (79) | 0.001 |
| US resident | 2776 (98) | 1835 (97) | 941 (99) | 0.001 |
| Undergraduate education or above | 1434 (51) | 946 (50) | 488 (52) | 0.570 |
| Serum albumin (g/dL) | 4 ± 0.6 | 4.0 ± 0.6 | 3.9 ± 0.6 | 0.005 |
| Kidney donor status | <0.001 | |||
| 2152 (76) | 1872 (100) | 280 (30) | |
| 669 (24) | 3 (0) | 666 (70) | |
| Donor age | 21.9 ± 28.1 | 3.0 ± 8.0 | 59.3 ± 10.9 | <0.001 |
| Donor male sex | 1482 (53) | 1079 (58) | 403 (43) | <0.001 |
| Donor race | <0.001 | |||
| 1724 (61) | 1063 (57) | 661 (70) | |
| 555 (20) | 410 (22) | 145 (15) | |
| 386 (14) | 308 (16) | 78 (8) | |
| 156 (6) | 94 (5) | 62 (7) | |
| History of hypertension in donor | 651 (23) | 27 (1) | 624 (66) | <0.001 |
| Kidney donor profile index (KDPI) | <0.001 | |||
| 1981 (70) | 1593 (85) | 388 (41) | |
| 840 (30) | 282 (15) | 558 (59) | |
| HLA mismatch, median (IQR) | 5 (4, 5) | 5 (4, 5) | 5 (4, 5) | 0.06 |
| Cold ischemia time (hours) | 19.6 ± 10.1 | 18.0 ± 9.3 | 22.9 ± 10.9 | <0.001 |
| Kidney on pump | 1028 (36) | 385 (21) | 643 (68) | <0.001 |
| Delay graft function | 660 (23) | 324 (17) | 336 (36) | <0.001 |
| Allocation type | 0.001 | |||
| 1509 (53) | 965 (51) | 544 (58) | |
| 654 (23) | 476 (25) | 178 (19) | |
| 658 (23) | 434 (23) | 224 (24) | |
| Epstein–Barr virus status | <0.001 | |||
| 64 (2) | 63 (3) | 1 (0) | |
| 2588 (92) | 1746 (93) | 842 (89) | |
| 169 (6) | 66 (4) | 103 (11) | |
| Cytomegalovirus status | <0.001 | |||
| 380 (13) | 280 (15) | 100 (11) | |
| 954 (34) | 763 (41) | 191 (20) | |
| 1084 (38) | 608 (32) | 476 (50) | |
| 403 (14) | 224 (12) | 179 (19) | |
| Induction immunosuppression | ||||
| 1732 (61) | 1236 (66) | 496 (52) | <0.001 |
| 353 (13) | 213 (11) | 140 (15) | 0.009 |
| 582 (21) | 315 (17) | 267 (28) | <0.001 |
| 87 (3) | 54 (3) | 33 (3) | 0.378 |
| 173 (6) | 111 (6) | 62 (7) | 0.508 |
| Maintenance Immunosuppression | ||||
| 2557 (91) | 1713 (91) | 844 (89) | 0.065 |
| 29 (1) | 17 (1) | 12 (1) | 0.368 |
| 2604 (92) | 1739 (93) | 865 (91) | 0.218 |
| 7 (0) | 7 (0) | 0 (0) | 0.060 |
| 9 (0) | 4 (0) | 5 (1) | 0.161 |
| 1954 (69) | 1270 (68) | 684 (72) | 0.013 |
| Cluster 1 | Cluster 2 | p-Value | |
|---|---|---|---|
| 1-year survival | 98.0% | 94.6% | <0.001 |
| HR for 1-year mortality | 1 (ref) | 2.62 (1.70–4.08) | <0.001 |
| 5-year survival | 92.1% | 76.3% | <0.001 |
| HR for 5-year mortality | 1 (ref) | 3.12 (2.41–4.05) | <0.001 |
| 1-year death-censored graft survival | 93.5% | 94.9% | 0.08 |
| HR for 1-year death-censored graft loss | 1 (ref) | 0.73 (0.51–1.03) | 0.08 |
| 5-year death-censored graft survival | 89.2% | 84.8% | 0.28 |
| HR for 5-year death-censored graft loss | 1 (ref) | 1.15 (0.89–1.48) | 0.28 |
| 1-year acute rejection | 4.2% | 6.1% | 0.03 |
| OR for 1-year acute rejection | 1 (ref) | 1.48 (1.05–2.10) | 0.03 |
| Patient Death | Death-Censored Graft Failure | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Recipient age | ||||
| 1.94 (1.13–3.21) | 0.02 | 1.26 (0.85–1.83) | 0.25 |
| 2.00 (1.42–2.87) | <0.001 | 1.41 (0.91–2.21) | 0.12 |
| Recipient sex | ||||
| 2.92 (2.11–4.10) | <0.001 | 1.47 (1.03–2.10) | 0.03 |
| 3.03 (1.95–4.68) | <0.001 | 1.00 (0.66–1.46) | 0.99 |
| Recipient race | ||||
| 3.12 (2.11–4.69) | <0.001 | 1.03 (0.68–1.55) | 0.89 |
| 2.89 (2.04–4.12) | <0.001 | 1.25 (0.90–1.72) | 0.18 |
| Recipient body mass index | ||||
| 3.20 (2.36–4.34) | <0.001 | 1.11 (0.81–1.50) | 0.52 |
| 2.22 (1.34–3.82) | 0.002 | 1.05 (0.64–1.74) | 0.84 |
| Kidney retransplant | ||||
| 3.25 (2.49–4.27) | <0.001 | 1.14 (0.88–1.48) | 0.33 |
| 3.59 (0.81–11.55) | 0.09 | 2.95 (0.68–9.18) | 0.13 |
| Preemptive transplant | ||||
| 3.08 (2.35–4.03) | <0.001 | 1.21 (0.92–1.57) | 0.16 |
| 4.43 (1.64–13.94) | 0.003 | 0.71 (0.25–1.78) | 0.48 |
| Recipient diabetes | ||||
| 3.61 (2.50–5.22) | <0.001 | 1.15 (0.82–1.60) | 0.41 |
| 1.84 (1.27–2.69) | 0.001 | 1.11 (0.73–1.70) | 0.63 |
| PRA | ||||
| 3.15 (2.31–4.33) | <0.001 | 1.14 (0.84–1.54) | 0.39 |
| 3.13 (1.94–5.05) | <0.001 | 1.22 (0.74–1.94) | 0.42 |
| Donor sex | ||||
| 3.46 (2.46–4.89) | <0.001 | 1.49 (1.05–2.08) | 0.02 |
| 2.99 (2.01–4.50) | <0.001 | 0.90 (0.61–1.33) | 0.60 |
| Donor race | ||||
| 3.12 (2.23–4.38) | <0.001 | 1.02 (0.74–1.40) | 0.91 |
| 3.23 (2.12–4.91) | <0.001 | 1.44 (0.95–2.19) | 0.10 |
| Donor hypertension | ||||
| 2.92 (2.03–4.13) | <0.001 | 1.11 (0.75–1.61) | 0.58 |
| 2.52 (0.80–15.30) | 0.13 | 0.77 (0.32–2.52) | 0.61 |
| KDPI | ||||
| 2.30 (1.56–3.33) | <0.001 | 1.21 (0.82–1.73) | 0.33 |
| 3.12 (1.94–5.34) | <0.001 | 0.69 (0.46–1.03) | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tangpanithandee, S.; Thongprayoon, C.; Jadlowiec, C.C.; Mao, S.A.; Mao, M.A.; Vaitla, P.; Leeaphorn, N.; Kaewput, W.; Pattharanitima, P.; Krisanapan, P.; et al. Clinical Phenotypes of Dual Kidney Transplant Recipients in the United States as Identified through Machine Learning Consensus Clustering. Medicina 2022, 58, 1831. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121831
Tangpanithandee S, Thongprayoon C, Jadlowiec CC, Mao SA, Mao MA, Vaitla P, Leeaphorn N, Kaewput W, Pattharanitima P, Krisanapan P, et al. Clinical Phenotypes of Dual Kidney Transplant Recipients in the United States as Identified through Machine Learning Consensus Clustering. Medicina. 2022; 58(12):1831. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121831
Chicago/Turabian StyleTangpanithandee, Supawit, Charat Thongprayoon, Caroline C. Jadlowiec, Shennen A. Mao, Michael A. Mao, Pradeep Vaitla, Napat Leeaphorn, Wisit Kaewput, Pattharawin Pattharanitima, Pajaree Krisanapan, and et al. 2022. "Clinical Phenotypes of Dual Kidney Transplant Recipients in the United States as Identified through Machine Learning Consensus Clustering" Medicina 58, no. 12: 1831. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58121831