
Laryngeal Helicobacter pylori Infection and Laryngeal Cancer-Case Series and a Systematic Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Collection of the Data and Specimens
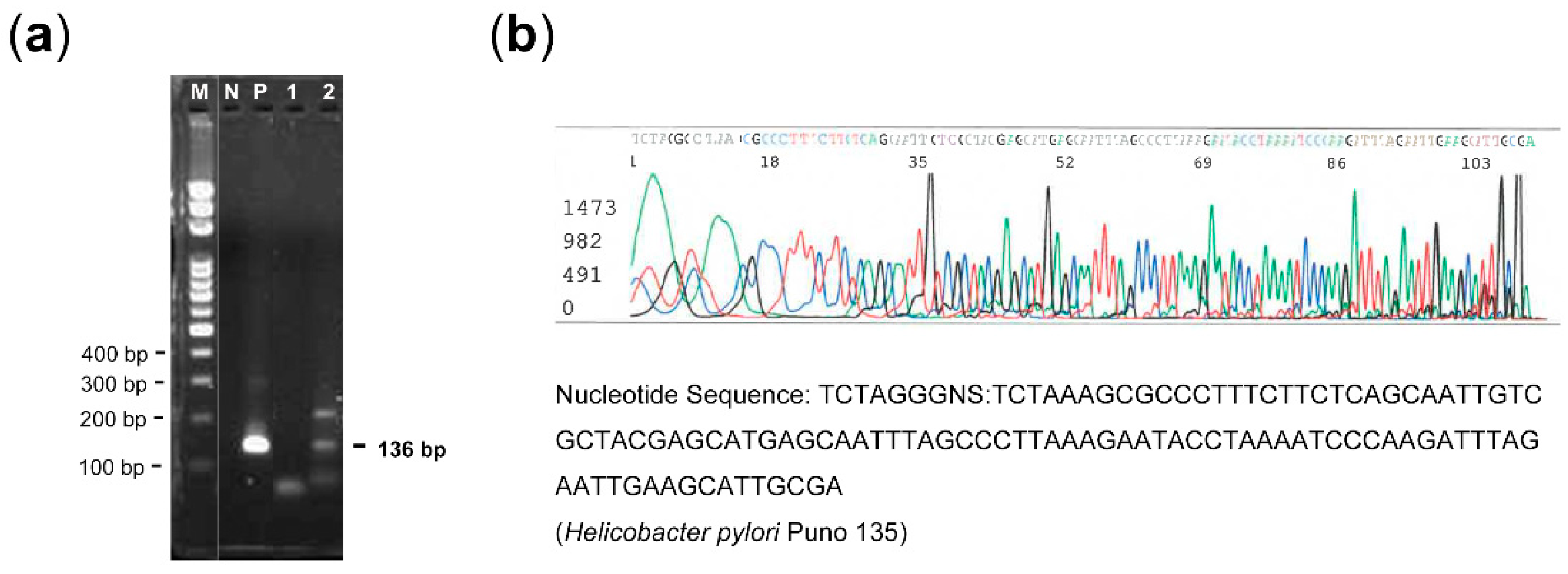
2.3. Detection of H. pylori DNA in the Laryngeal Lesions
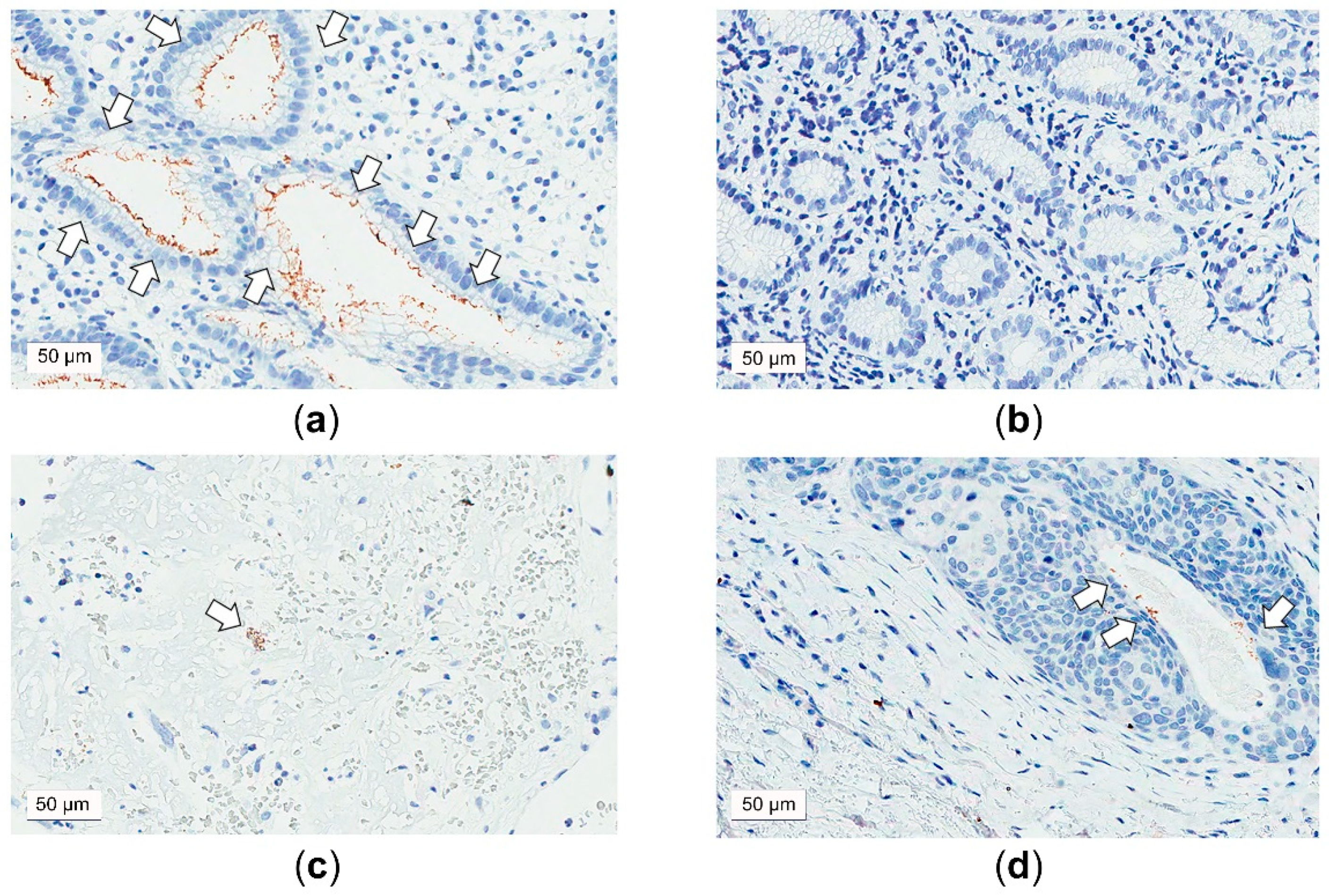
2.4. Detection of H. pylori Antigen in the Laryngeal Lesions
2.5. Measurements of the Expressions of E-cadherin and CD1d in the Laryngeal Lesions
2.6. Systematic Review
2.6.1. Defining the Clinical Question
2.6.2. Identification of Evidence
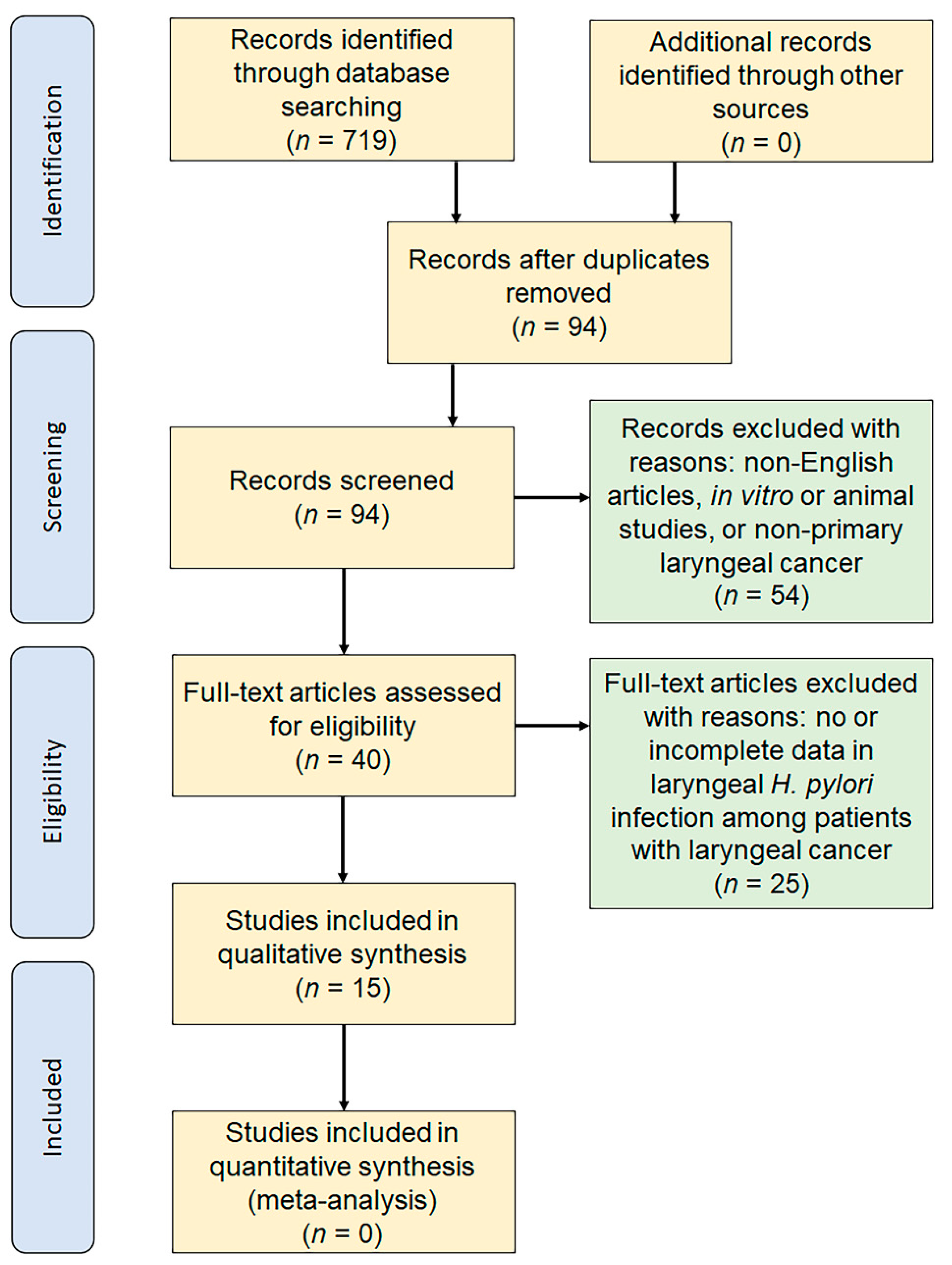
2.6.3. Study Selection
2.6.4. Data Extraction
2.6.5. Study Quality Assessment
2.7. Statistical Analysis
3. Results
3.1. Patient Demographics and Tumor Staging
3.2. H. pylori Infection Status of the Larynx
3.3. Expression of E-cadherin and CD1d of the Larynx
3.4. Relationship between H. pylori Status, LPR Symptom, and Related Biomarkers and Malignant Potential and Pathological Status
3.5. Associations of H. pylori Status, RSI Score, and Related Biomarkers with the Risk of Laryngeal Cancer
3.6. Systematic Review
3.6.1. Study Selection and Characteristics of Included Studies
3.6.2. Level of Evidence
3.6.3. Study Selection and Characteristics of Included Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sokic, S.I.; Adanja, B.J.; Marinkovic, J.P.; Vlajinac, H.D. Risk factors for laryngeal cancer. Eur. J. Epidemiol. 1995, 11, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Promotion Administration. Crude Incidence Rate of Laryngeal Cancer in Taiwan in 2016. Available online: https://cris.hpa.gov.tw/pagepub/Home.aspx?itemNo=cr.q.10 (accessed on 9 November 2020).
- Cattaruzza, M.S.; Maisonneuve, P.; Boyle, P. Epidemiology of laryngeal cancer. Eur. J. Cancer Part B Oral Oncol. 1996, 32, 293–305. [Google Scholar] [CrossRef]
- Ansari, S.; Yamaoka, Y. Helicobacter pylori virulence factors exploiting gastric colonization and its pathogenicity. Toxins 2019, 11, 677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eusebi, L.H.; Zagari, R.M.; Bazzoli, F. Epidemiology of helicobacter pylori infection. Helicobacter 2014, 19 (Suppl. 1), 1–5. [Google Scholar] [CrossRef]
- Hatakeyama, M. Malignant helicobacter pylori-associated diseases: Gastric cancer and malt lymphoma. Adv. Exp. Med. Biol. 2019, 1149, 135–149. [Google Scholar]
- Conteduca, V.; Sansonno, D.; Lauletta, G.; Russi, S.; Ingravallo, G.; Dammacco, F.H. Pylori infection and gastric cancer: State of the art (review). Int. J. Oncol. 2013, 42, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Fasciana, T.; Capra, G.; Calà, C.; Zambuto, S.; Mascarella, C.; Colomba, C.; Di Carlo, P.; Giammanco, A. Helicobacter pylori and epstein barr co-infection in gastric disease. Pharmacol. Online 2017, 1, 73–82. [Google Scholar]
- Teresa, F.; Serra, N.; Capra, G.; Mascarella, C.; Gagliardi, C.; Di Carlo, P.; Cannella, S.; Simonte, M.R.; Lipari, D.; Sciortino, M.; et al. Helicobacter pylori and epstein-barr virus infection in gastric diseases: Correlation with il-10 and il1rn polymorphism. J. Oncol. 2019, 2019, 1785132. [Google Scholar] [CrossRef] [Green Version]
- Aziz, F.; Xin, M.; Gao, Y.; Chakroborty, A.; Khan, I.; Monts, J.; Monson, K.; Bode, A.M.; Dong, Z. Induction and prevention of gastric cancer with combined helicobacter pylori and capsaicin administration and dfmo treatment, respectively. Cancers 2020, 12, 816. [Google Scholar] [CrossRef] [Green Version]
- Pajic Matic, I.; Jelic, D.; Matic, I.; Maslovara, S.; Mendes, T. Presence of helicobacter pylori in the stomach and laryngeal mucosal linings in patients with laryngeal cancer. Acta Clin. Croat. 2018, 57, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Pajic Matic, I.; Matic, I.; Maslovara, S.; Veselski, K.; Stojadinovic, T.; Vuckovic, I. Helicobacter pylori gastric infection in patients with laryngeal cancer and chronic laryngitis. Eur. Arch. Otorhinolaryngol. 2021, 278, 135–139. [Google Scholar] [CrossRef]
- Bao, X.; Yang, H.; Shi, Y.; Deng, A. Analysis of the association between helicobacter pylori infection and laryngeal lesions. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2020, 34, 924–927. [Google Scholar] [PubMed]
- Pirzadeh, A.; Doustmohammadian, N.; Khoshbaten, M.; Doustmohammadion, S. Is there any association between helicobacter pylori infection and laryngeal carcinoma? Asian Pac. J. Cancer Prev. 2011, 12, 897–900. [Google Scholar] [PubMed]
- Fellmann, J.; Weisert, J.U.; Soltermann, A.; Morand, G.; Morra, L.; Moch, H.; Huber, G.F.; Probst, R. Helicobacter pylori detected in pharyngeal and laryngeal pathologies in patients with proven gastric colonization. Head Neck 2014, 36, 1562–1566. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, D.; Yang, Y.; Zhou, L.; Tao, L. Association between helicobacter pylori infection and carcinoma of the larynx or pharynx. Head Neck 2016, 38 (Suppl. 1), E2291–E2296. [Google Scholar] [CrossRef]
- Campbell, R.; Kilty, S.J.; Hutton, B.; Bonaparte, J.P. The role of helicobacter pylori in laryngopharyngeal reflux. Otolaryngol. Head Neck Surg. 2017, 156, 255–262. [Google Scholar] [CrossRef]
- Pokharel, A.; Mayya, J.P.; Upadhyay, H.P. Comparison of proton pump inhibitor and triple therapy regimen for laryngospharyngeal reflux disease. J. Nepal Health Res. Counc. 2020, 18, 513–519. [Google Scholar] [CrossRef]
- Gong, H.; Shi, Y.; Zhou, L.; Tao, L.; Shi, Y.; Cao, W.; Cheng, L. Helicobacter pylori infection of the larynx may be an emerging risk factor for laryngeal squamous cell carcinoma. Clin. Transl. Oncol. 2012, 14, 905–910. [Google Scholar] [CrossRef]
- Genc, R.; Cagli, S.; Yuce, I.; Vural, A.; Okuducu, H.; Patiroglu, T.; Guney, E. The role of h. Pylori in the development of laryngeal squamous cell carcinoma. Dis. Markers 2013, 35, 447–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scida, S.; Russo, M.; Miraglia, C.; Leandro, G.; Franzoni, L.; Meschi, T.; De’ Angelis, G.L.; Di Mario, F. Relationship between helicobacter pylori infection and gerd. Acta Biomed. 2018, 89, 40–43. [Google Scholar] [PubMed]
- Eells, A.C.; Mackintosh, C.; Marks, L.; Marino, M.J. Gastroesophageal reflux disease and head and neck cancers: A systematic review and meta-analysis. Am. J. Otolaryngol. 2020, 41, 102653. [Google Scholar] [CrossRef] [PubMed]
- Fang, T.J.; Lee, L.A.; Li, H.Y.; Yang, C.; Huang, C.G. Helicobacter pylori colonization in the larynges of patients with hoarseness. Laryngoscope 2008, 118, 389–393. [Google Scholar] [CrossRef]
- Chen, M.; Chen, J.; Yang, Y.; Cheng, L.; Wu, H.T. Possible association between helicobacter pylori infection and vocal fold leukoplakia. Head Neck 2018, 40, 1498–1507. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Fang, Y.; Cheng, L.; Wu, H. Helicobacter pylori is associated with poor prognosis of laryngeal precancerous lesion. Auris Nasus Larynx 2020, 47, 268–275. [Google Scholar] [CrossRef]
- Lopes, A.I.; Vale, F.F.; Oleastro, M. Helicobacter pylori infection—Recent developments in diagnosis. World J. Gastroenterol. 2014, 20, 9299–9313. [Google Scholar]
- Wang, Y.K.; Kuo, F.C.; Liu, C.J.; Wu, M.C.; Shih, H.Y.; Wang, S.S.; Wu, J.Y.; Kuo, C.H.; Huang, Y.K.; Wu, D.C. Diagnosis of helicobacter pylori infection: Current options and developments. World J. Gastroenterol. 2015, 21, 11221–11235. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, M.A.; Zabaglia, L.M.; Pereira, W.N.; Orcini, W.A.; de Labio, R.W.; Caleman Neto, A.; Wisnieski, F.; Calcagno, D.Q.; Santos, L.C.; Assumpcao, P.P.; et al. Downregulated expression of e-cadherin and tp53 in patients with gastric diseases: The involvement of h. Pylori infection and its virulence markers. J. Gastrointest. Cancer 2016, 47, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Reichel, O.; Mayr, D.; Durst, F.; Berghaus, A. E-cadherin but not beta-catenin expression is decreased in laryngeal biopsies from patients with laryngopharyngeal reflux. Eur. Arch. Otorhinolaryngol. 2008, 265, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.; Ma, X.; Zhou, H.; Yu, C.; Zhang, Y.; Yang, X.; Shen, X.; Gao, X. Expression and prognostic value of e-cadherin in laryngeal cancer. Acta Otolaryngol. 2016, 136, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Hafezi, N.; Ajami, A.; Farazmandfar, T.; Hosseini, V.; Alizadeh-Navaei, R.; Tehrani, M. Increased expression of two alternative spliced variants of cd1d molecule in human gastric cancer. Iran. J. Immunol. 2015, 12, 129–140. [Google Scholar]
- Rees, L.E.; Pazmany, L.; Gutowska-Owsiak, D.; Inman, C.F.; Phillips, A.; Stokes, C.R.; Johnston, N.; Koufman, J.A.; Postma, G.; Bailey, M.; et al. The mucosal immune response to laryngopharyngeal reflux. Am. J. Respir. Crit. Care Med. 2008, 177, 1187–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, S.; Dhodapkar, M.V. Natural killer t cells in cancer immunotherapy. Front. Immunol. 2017, 8, 1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tae, K.; Jin, B.J.; Ji, Y.B.; Jeong, J.H.; Cho, S.H.; Lee, S.H. The role of laryngopharyngeal reflux as a risk factor in laryngeal cancer: A preliminary report. Clin. Exp. Otorhinolaryngol. 2011, 4, 101–104. [Google Scholar] [CrossRef]
- Huang, C.G.; Lee, L.A.; Fang, T.J.; Li, H.Y.; Liao, C.T.; Kang, C.J.; Yen, T.C.; Tsao, K.C.; Chen, T.C.; Shih, S.R. Human papillomavirus infection is not associated with laryngeal squamous cell carcinoma in taiwan. J. Microbiol. Immunol. Infect. 2020, 53, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.A.; Fang, T.J.; Li, H.Y.; Huang, C.G.; Chen, T.C.; Liao, C.T.; Kang, C.J.; Chang, K.P.; Yen, T.C. Low expression of prb predicts disease relapse in early glottic cancer treated with transoral laser microsurgery. Laryngoscope 2019, 129, E220–E226. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Postma, G.N.; Koufman, J.A. Validity and reliability of the reflux symptom index (rsi). J. Voice 2002, 16, 274–277. [Google Scholar] [CrossRef]
- Chung, J.H.; Tae, K.; Lee, Y.S.; Jeong, J.H.; Cho, S.H.; Kim, K.R.; Park, C.W.; Han, D.S. The significance of laryngopharyngeal reflux in benign vocal mucosal lesions. Otolaryngol. Head Neck Surg. 2009, 141, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Sereg-Bahar, M.; Jerin, A.; Hocevar-Boltezar, I. Higher levels of total pepsin and bile acids in the saliva as a possible risk factor for early laryngeal cancer. Radiol. Oncol. 2015, 49, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the ajcc cancer staging manual and the future of tnm. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Rugge, M.; Busatto, G.; Cassaro, M.; Shiao, Y.-H.; Russo, V.; Leandro, G.; Avellini, C.; Fabiano, A.; Sidoni, A.; Covacci, A. Patients younger than 40 years with gastric carcinoma. Cancer 1999, 85, 2506–2511. [Google Scholar] [CrossRef]
- Amorim, I.; Smet, A.; Alves, O.; Teixeira, S.; Saraiva, A.L.; Taulescu, M.; Reis, C.; Haesebrouck, F.; Gartner, F. Presence and significance of helicobacter spp. In the gastric mucosa of portuguese dogs. Gut Pathog. 2015, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Braun, M.; Kirsten, R.; Rupp, N.J.; Moch, H.; Fend, F.; Wernert, N.; Kristiansen, G.; Perner, S. Quantification of protein expression in cells and cellular subcompartments on immunohistochemical sections using a computer supported image analysis system. Histol. Histopathol. 2013, 28, 605–610. [Google Scholar]
- Lee, L.A.; Fang, T.J.; Li, H.Y.; Chuang, H.H.; Kang, C.J.; Chang, K.P.; Liao, C.T.; Chen, T.C.; Huang, C.G.; Yen, T.C. Effects of epstein-barr virus infection on the risk and prognosis of primary laryngeal squamous cell carcinoma: A hospital-based case-control study in taiwan. Cancers 2021, 13, 1741. [Google Scholar] [CrossRef]
- Hutchinson, R.A.; Coleman, H.G.; Gately, K.; Young, V.; Nicholson, S.; Cummins, R.; Kay, E.; Hynes, S.O.; Dunne, P.D.; Senevirathne, S.; et al. Ihc-based subcellular quantification provides new insights into prognostic relevance of flip and procaspase-8 in non-small-cell lung cancer. Cell Death Discov. 2017, 3, 17050. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (Ocebm) Levels of Evidence (Background Document). Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/explanation-of-the-2011-ocebm-levels-of-evidence/ (accessed on 1 February 2021).
- Akbayir, N.; Basak, T.; Seven, H.; Sungun, A.; Erdem, L. Investigation of helicobacter pylori colonization in laryngeal neoplasia. Eur. Arch. Otorhinolaryngol. 2005, 262, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Kizilay, A.; Saydam, L.; Aydin, A.; Kalcioglu, M.T.; Ozturan, O.; Aydin, N.E. Histopathologic examination for helicobacter pylori as a possible etiopathogenic factor in laryngeal carcinoma. Chemotherapy 2006, 52, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Titiz, A.; Ozcakir, O.; Ceyhan, S.; Yilmaz, Y.F.; Unal, A.; Akyon, Y. The presence of helicobacter pylori in the larynx pathologies. Auris Nasus Larynx 2008, 35, 534–538. [Google Scholar] [CrossRef] [PubMed]
- Grbesa, I.; Marinkovic, M.; Ivkic, M.; Kruslin, B.; Novak-Kujundzic, R.; Pegan, B.; Bogdanovic, O.; Bedekovic, V.; Gall-Troselj, K. Loss of imprinting of igf2 and h19, loss of heterozygosity of igf2r and ctcf, and helicobacter pylori infection in laryngeal squamous cell carcinoma. J. Mol. Med. 2008, 86, 1057–1066. [Google Scholar] [CrossRef]
- Shi, Y.; Gong, H.; Zhou, L.; Tao, L.; Shi, Y.; Cao, W.; Cheng, L. Association between helicobacter pylori infection and laryngeal squamous cell carcinoma in a chinese male population. ORL J. Otorhinolaryngol. Relat. Spec. 2011, 73, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Siupsinskiene, N.; Jurgutaviciute, V.; Katutiene, I.; Janciauskas, D.; Vaitkus, S.; Adamonis, K. Helicobacter pylori infection in laryngeal diseases. Eur. Arch. Otorhinolaryngol. 2013, 270, 2283–2288. [Google Scholar] [CrossRef] [PubMed]
- Burduk, P.K. Association between infection of virulence caga gene helicobacter pylori and laryngeal squamous cell carcinoma. Med. Sci. Monit. 2013, 19, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Amizadeh, M.; Shamsadini, A.; Arabzadeh, A.; Jazayeri, S. Association of caga positive helicobacter pylori infection and laryngeal squamous cell carcinoma: A pcr approach. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, I.; Erkul, E.; Berber, U.; Kucukodaci, Z.; Narli, G.; Haholu, A.; Demirel, D. The presence of helicobacter pylori in laryngeal squamous cell carcinoma. Eur. Arch. Otorhinolaryngol. 2016, 273, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Barakat, G.; Nabiel, Y.; Ali, O.; El-Nady, G.; Musaad, A.; El-Sharkawy, A. Urea and caga genes of helicobacter pylori in egyptian patients with laryngeal squamous cell carcinoma and benign laryngeal polyps: A cohort study. Eur. Arch. Otorhinolaryngol. 2016, 273, 3243–3248. [Google Scholar] [CrossRef] [PubMed]
- Masoud, N.; Manouchehr, K.; Najmeh, D.; Monireh, H. Lack of association between helicobacter pylori and laryngeal carcinoma. Asian Pac. J. Cancer Prev. 2008, 9, 81–82. [Google Scholar]
- Nurgalieva, Z.Z.; Graham, D.Y.; Dahlstrom, K.R.; Wei, Q.; Sturgis, E.M. A pilot study of helicobacter pylori infection and risk of laryngopharyngeal cancer. Head Neck 2005, 27, 22–27. [Google Scholar] [CrossRef]
- Ozyurt, M.; Gungor, A.; Ergunay, K.; Cekin, E.; Erkul, E.; Haznedaroglu, T. Real-time pcr detection of helicobacter pylori and virulence-associated caga in nasal polyps and laryngeal disorders. Otolaryngol. Head Neck Surg. 2009, 141, 131–135. [Google Scholar] [CrossRef]
- Kocsmar, E.; Szirtes, I.; Kramer, Z.; Szijarto, A.; Bene, L.; Buzas, G.M.; Kenessey, I.; Bronsert, P.; Csanadi, A.; Lutz, L.; et al. Sensitivity of helicobacter pylori detection by giemsa staining is poor in comparison with immunohistochemistry and fluorescent in situ hybridization and strongly depends on inflammatory activity. Helicobacter 2017, 22, e12387. [Google Scholar] [CrossRef]
- Qian, X.; Huang, C.; Cho, C.H.; Hui, W.M.; Rashid, A.; Chan, A.O. E-cadherin promoter hypermethylation induced by interleukin-1beta treatment or h. Pylori infection in human gastric cancer cell lines. Cancer Lett. 2008, 263, 107–113. [Google Scholar] [CrossRef]
- Yang, Y.; Du, J.; Liu, F.; Wang, X.; Li, X.; Li, Y. Role of caspase-3/e-cadherin in helicobacter pylori-induced apoptosis of gastric epithelial cells. Oncotarget 2017, 8, 59204–59216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.O.; Chu, K.M.; Huang, C.; Lam, K.F.; Leung, S.Y.; Sun, Y.W.; Ko, S.; Xia, H.H.; Cho, C.H.; Hui, W.M.; et al. Association between helicobacter pylori infection and interleukin 1beta polymorphism predispose to cpg island methylation in gastric cancer. Gut 2007, 56, 595–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Vela, J.L.; Matsumura, F.; Hoshino, H.; Tyznik, A.; Lee, H.; Girardi, E.; Zajonc, D.M.; Liddington, R.; Kobayashi, M.; et al. Helicobacter pylori cholesteryl alpha-glucosides contribute to its pathogenicity and immune response by natural killer t cells. PLoS ONE 2013, 8, e78191. [Google Scholar]
- Kronenberg, M. Toward an understanding of nkt cell biology: Progress and paradoxes. Annu. Rev. Immunol. 2005, 23, 877–900. [Google Scholar] [CrossRef]
- Bendelac, A.; Savage, P.B.; Teyton, L. The biology of nkt cells. Annu. Rev. Immunol. 2007, 25, 297–336. [Google Scholar] [CrossRef] [Green Version]
- Takahashi-Kanemitsu, A.; Knight, C.T.; Hatakeyama, M. Molecular anatomy and pathogenic actions of helicobacter pylori caga that underpin gastric carcinogenesis. Cell. Mol. Immunol. 2020, 17, 50–63. [Google Scholar] [CrossRef] [Green Version]
- Lai, S.W. Helicobacter pylori gastric infection in patients with laryngeal cancer. Eur. Arch. Otorhinolaryngol. 2021, 278, 1295. [Google Scholar] [CrossRef] [PubMed]
- Meine, G.C.; Rota, C.; Dietz, J.; Sekine, S.; Prolla, J.C. Relationship between caga-positive helicobacter pylori infection and risk of gastric cancer: A case control study in porto alegre, rs, brazil. Arq. Gastroenterol. 2011, 48, 41–45. [Google Scholar] [CrossRef] [Green Version]
- Chauhan, N.; Tay, A.C.Y.; Marshall, B.J.; Jain, U. Helicobacter pylori vaca, a distinct toxin exerts diverse functionalities in numerous cells: An overview. Helicobacter 2019, 24, e12544. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | All | VP | VFL | Laryngeal Cancer | p-Value 1 |
|---|---|---|---|---|---|
| Patients | (n = 105) | (n = 37) | (n = 22) | (n = 46) | |
| Clinical characteristics | |||||
| Male sex, n (%) | 93 (89) | 30 (81) | 20 (91) | 43 (94) | 0.20 |
| Age (years), mean (SD) | 58.6 (14.0) | 50.5 (11.1) 2 | 55.5 (15.2) 3 | 66.6 (11.1) 2,3 | <0.001 |
| Cigarette smoking, n (%) | 82 (78) | 24 (65) | 19 (86) | 39 (85) | 0.05 |
| Alcohol consumption, n (%) | 67 (64) | 19 (51) | 17 (77) | 31 (67) | 0.11 |
| RSI score, mean (SD) | 5.9 (3.8) | 8.1 (5.3) 2 | 6.4 (3.7) | 5.6 (3.8) 2 | 0.04 |
| Pathological characteristics | |||||
| Tis, n (%) | ‒ | ‒ | ‒ | 3 (6) | ‒ |
| T1, n (%) | ‒ | ‒ | ‒ | 23 (49) | ‒ |
| T2, n (%) | ‒ | ‒ | ‒ | 15 (32) | ‒ |
| T3, n (%) | ‒ | ‒ | ‒ | 3 (6) | ‒ |
| T4, n (%) | ‒ | ‒ | ‒ | 3 (6) | ‒ |
| N0, n (%) | ‒ | ‒ | ‒ | 45 (96) | ‒ |
| N1, n (%) | ‒ | ‒ | ‒ | 1 (2) | ‒ |
| N2, n (%) | ‒ | ‒ | ‒ | 1 (2) | ‒ |
| Variables | All | VP | VFL | Laryngeal Cancer | p-Value 1 |
|---|---|---|---|---|---|
| Helicobacter pylori status in the laryngeal lesions (n = 105) | |||||
| Patent number (%) | 105 (100) | 37 (35) | 22 (21) | 46 (44) | |
| DNA positivity, n (%) | 1 (1) | 1 (3) | 0 (0) | 0 (0) | 0.40 |
| Antigen positivity, n (%) | 2 (2) | 1 (3) | 0 (0) | 1 (2) | 0.75 |
| Immunohistochemistry of Helicobacter pylori- and LPR-related biomarkers (n = 84) | |||||
| Patent number (%) | 73 (100) | 24 (33) | 17 (23) | 32 (44) | |
| Expression of E-cadherin, mean (SD) | 95.5 (71.1) | 69.8 (55.8) | 115.0 (65.2) | 104.4 (80.3) | 0.08 |
| Patent number (%) | 84 (100) | 26 (31) | 17 (20) | 41 (49) | |
| Expression of CD1d, mean (SD) | 41.8 (48.6) | 23.0 (35.6) | 37.7 (41.7) | 53.0 (60.2) | 0.18 |
| Variables | Malignant Potential | Tumor Status | Neck Lymph Node Status |
|---|---|---|---|
| Helicobacter pylori DNA positivity | r = −0.12; p = 0.23 | ‒ | ‒ |
| n = 105 | n = 46 | n = 46 | |
| Helicobacter pylori antigen positivity | r = −0.01; p = 0.91 | r = 0.08; p = 0.61 | r = −0.05; p = 0.76 |
| n = 105 | n = 46 | n = 46 | |
| RSI score | r = −0.22; p = 0.03 | r = 0.20; p = 0.19 | r = 0.02; p = 0.89 |
| n = 105 | n = 46 | n = 46 | |
| E-cadherin | r = 0.17; p = 0.14 | r = 0.15; p = 0.43 | r = −0.17; p = 0.28 |
| n = 73 | n = 32 | n = 32 | |
| CD1d | r = 0.11; p = 0.31 | r = 0.02; p = 0.92 | r = −0.17; p = 0.28 |
| n = 84 | n = 41 | n = 41 |
| Variables | Odds Ratio (95% CI) 1 | p-Value | Odds Ratio (95% CI) 2 | p-Value |
|---|---|---|---|---|
| Model | Univariate analysis | Multivariate analysis | ||
| Age | 1.10 (1.06–1.15) | <0.001 | 1.11 (1.06–1.16) | <0.001 |
| Male sex | 2.58 (0.66–10.14) | 0.18 | 0.84 (0.14–4.98) | 0.85 |
| Cigarette smoking | 2.07 (0.77–5.57) | 0.15 | 2.40 (0.66–8.70) | 0.18 |
| Alcohol consumption | 1.32 (0.59–2.96) | 0.50 | 0.92 (0.34–2.53) | 0.87 |
| Helicobacter pylori DNA positivity | <0.001 (<0.001–) | >0.99 | <0.001 (<0.001–) | >0.99 |
| Helicobacter pylori antigen positivity | 1.29 (0.08–21.18) | 0.86 | 0.46 (0.03–8.13) | 0.60 |
| RSI score | 0.90 (0.82–0.996) | 0.04 | 0.96 (0.86–0.1.07) | 0.46 |
| Expression of E-cadherin | 1.00 (1.00–1.01) | 0.34 | 1.00 (0.99–1.01) | 0.75 |
| Expression of CD1d | 1.01 (1.00–1.02) | 0.08 | 1.00 (0.99–1.01) | 0.59 |
| First Author (Year) | Country | Sample Type | Detection Methods | Study Design | H. pylori Infection Rate in the Laryngeal Lesions | Level of Evidence | ||
|---|---|---|---|---|---|---|---|---|
| Laryngeal Cancer | Controls | p-Value | ||||||
| Akbayir N (2005) [49] | Turkey | FFPE | H/IHC | CCS | 0% (0/50) | 0% (0/50) | >0.99 | 3 |
| Kizilay A (2006) [50] | Turkey | FFPE | H | CCS | 0% (0/90) | 0% (0/30) | >0.99 | 3 |
| Titiz A (2008) [51] | Turkey | FF | PCR | CCS | 81% (17/21) | 0% (0/19) | <0.001 | 3 |
| Masoud N (2008) [59] | Iran | F/FFPE | RUT/H | CCS | 0% (0/44) | 0% (0/30) | >0.99 | 3 |
| Grbesa I (2008) [52] | Croatia | FF | PCR | CS | 26% (9/35) | NA | NA | 4 |
| Shi Y (2011) [53] | China | FF | PCR | CCS | 76% (45/59) | 32% (13/41) | <0.001 | 3 |
| Gong H (2012) [20] | China | FF | PCR | CCS | 72% (58/81) | 25% (19/75) | <0.001 | 3 |
| Siupsinskiene N (2013) [54] | United States | F | RUT | CS | 46% (6/13) | 9% (1/11) | 0.047 | 4 |
| Burduk PK (2013) [55] | Poland | F | PCR | CS | 47% (35/75) | NA | NA | 4 |
| Genç R (2013) [21] | Turkey | FFPE | IHC | CCS | 0% (0/31) | 0% (0/28) | >0.99 | 3 |
| Fellmann J (2014) [16] | Switzerland | FFPE | PCR | CS | 50% (2/4) | 25% (1/4) | 0.47 | 4 |
| Amizadeh M (2015) [56] | Iran | FF | PCR | CCS | 33% (24/72) | 46% (33/72) | 0.13 | 3 |
| Yilmaz I (2016) [57] | Turkey | FFPE | PCR | CS | 1% (1/74) | NA | NA | 4 |
| Barakat G (2016) [58] | Egypt | F | PCR | CCS | 59% (29/49) | 7% (1/15) | <0.001 | 3 |
| Pajić Matić I (2018) [12] | Croatia | FFPE | H/PCR | CS | 14% (7/51) | NA | NA | 4 |
| This study (2021) | Taiwan | FFPE | PCR/IHC | CS | 0% (0/46)/2% (1/46) | 3% (1/37)/3% (1/37) | 0.26 | 4 |
| Total 1 | 29.4% (234/795) | 16.7% (69/412) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsin, L.-J.; Chuang, H.-H.; Lin, M.-Y.; Fang, T.-J.; Li, H.-Y.; Liao, C.-T.; Kang, C.-J.; Chen, T.-C.; Huang, C.-G.; Yen, T.-C.; et al. Laryngeal Helicobacter pylori Infection and Laryngeal Cancer-Case Series and a Systematic Review. Microorganisms 2021, 9, 1129. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9061129
Hsin L-J, Chuang H-H, Lin M-Y, Fang T-J, Li H-Y, Liao C-T, Kang C-J, Chen T-C, Huang C-G, Yen T-C, et al. Laryngeal Helicobacter pylori Infection and Laryngeal Cancer-Case Series and a Systematic Review. Microorganisms. 2021; 9(6):1129. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9061129
Chicago/Turabian StyleHsin, Li-Jen, Hai-Hua Chuang, Mu-Yun Lin, Tuan-Jen Fang, Hsueh-Yu Li, Chun-Ta Liao, Chung-Jan Kang, Tse-Ching Chen, Chung-Guei Huang, Tzu-Chen Yen, and et al. 2021. "Laryngeal Helicobacter pylori Infection and Laryngeal Cancer-Case Series and a Systematic Review" Microorganisms 9, no. 6: 1129. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9061129