Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease—A Meta-Analysis

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
2.2. Data Abstraction
2.3. Outcomes
2.4. Data Synthesis and Statistical Analysis
3. Results
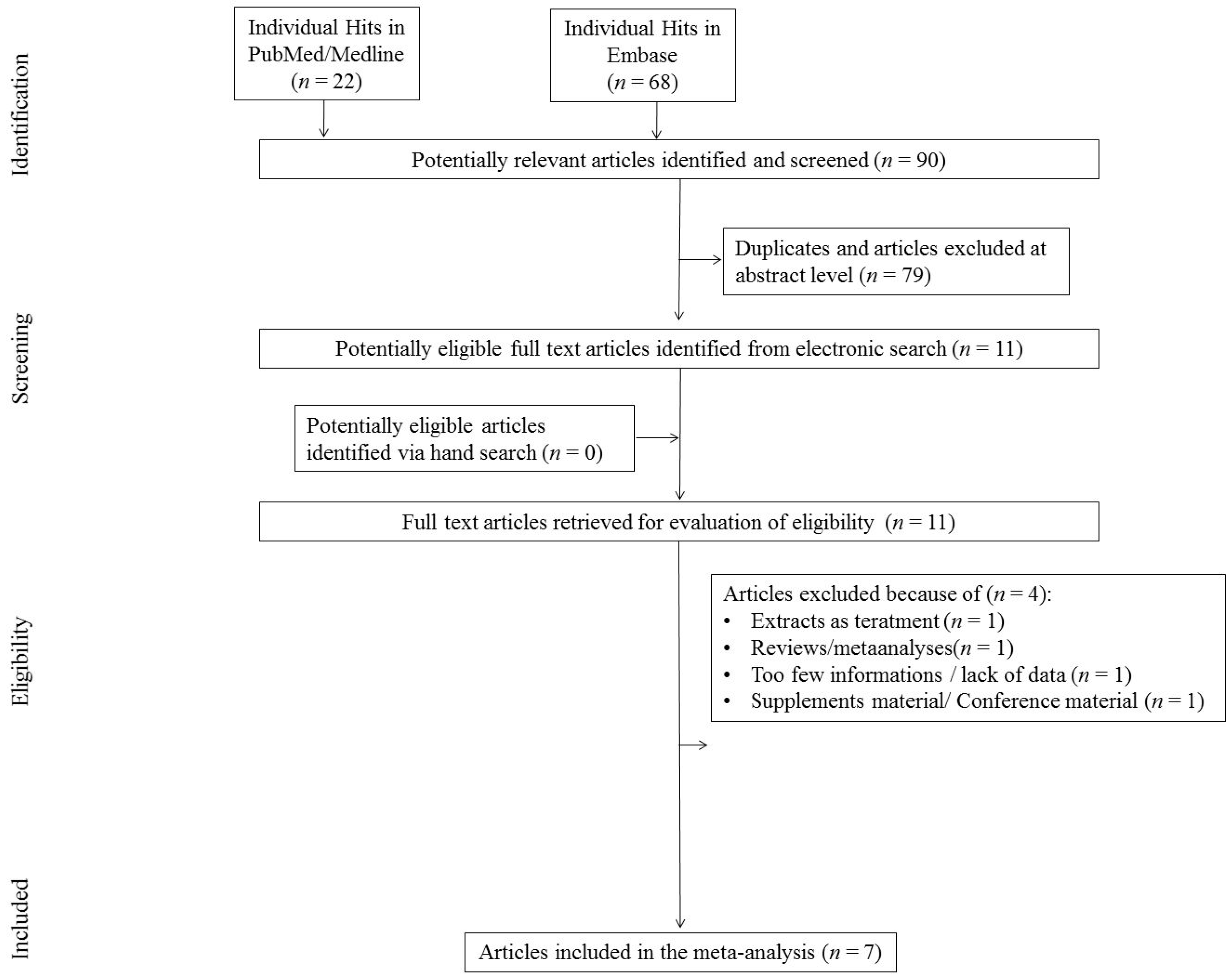
3.1. Search Results
3.2. Study, Patient, and Treatment Characteristics
3.3. Risk of Bias (ROB)
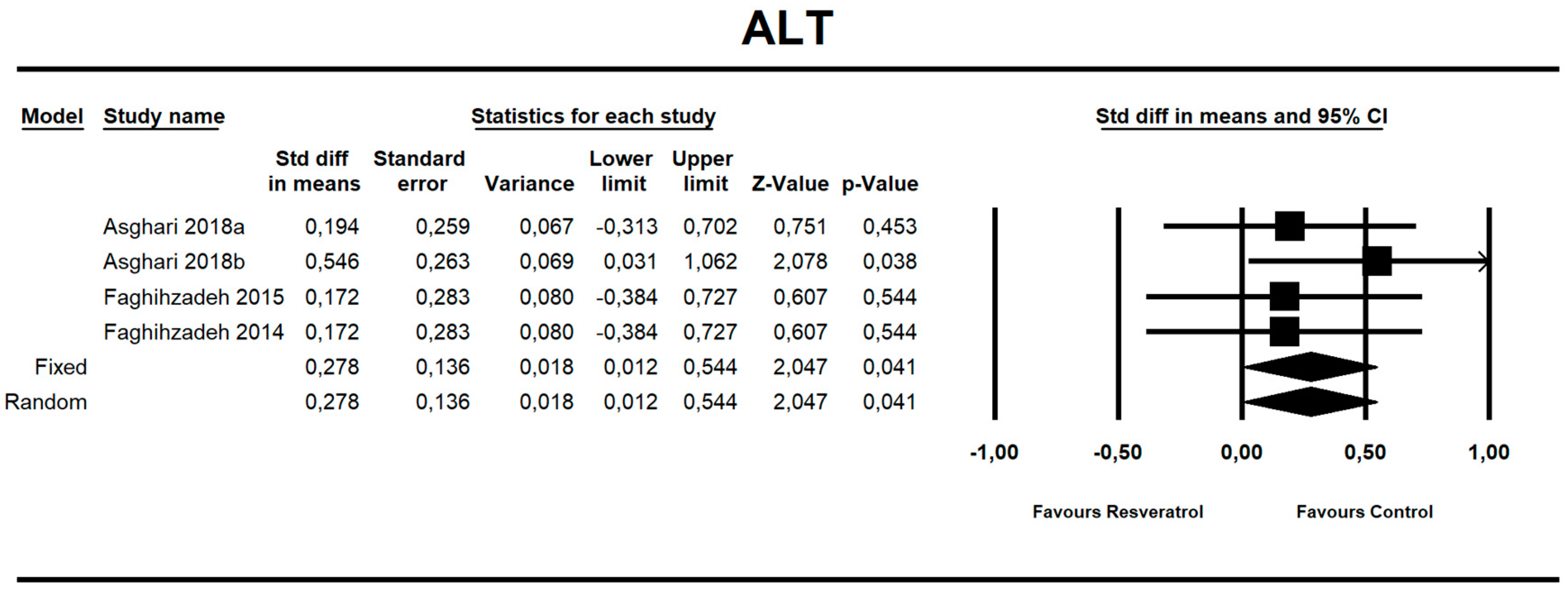
3.4. The Impact of Resveratrol on NAFLD-Related Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef]
- Maciejewska, D.; Stachowska, E. Non-alcoholic fatty liver disease (NAFLD)–epidemic of the XXI century. Postępy Hig. Med. Dośw. 2018, 72, 659–670. [Google Scholar] [CrossRef]
- Maciejewska, D.; Łukomska, A.; Dec, K.; Skonieczna-Żydecka, K.; Gutowska, I.; Skórka-Majewicz, M.; Styburski, D.; Misiakiewicz-Has, K.; Pilutin, A.; Palma, J.; et al. Diet-Induced Rat Model of Gradual Development of Non-Alcoholic Fatty Liver Disease (NAFLD) with Lipopolysaccharides (LPS) Secretion. Diagn. Basel Switz. 2019, 9, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loomba, R.; Sanyal, A.J. The global NAFLD epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Moschen, A.R. Evolution of inflammation in nonalcoholic fatty liver disease: The multiple parallel hits hypothesis. Hepatology 2010, 52, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Sookoian, S.; Chonchol, M.; Loria, P.; Targher, G. Cardiovascular and systemic risk in nonalcoholic fatty liver disease-atherosclerosis as a major player in the natural course of NAFLD. Curr. Pharm. Des. 2013, 19, 5177–5192. [Google Scholar] [CrossRef]
- Molina-Molina, E.; Krawczyk, M.; Stachowska, E.; Lammert, F.; Portincasa, P. Non-Alcoholic Fatty Liver Disease in Non-Obese Individuals: Prevalence, Pathogenesis and Treatment. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 638–645. [Google Scholar] [CrossRef]
- Elgebaly, A.; Radwan, I.A.I.; AboElnas, M.M.; Ibrahim, H.H.; Eltoomy, M.F.M.; Atta, A.A.; Mesalam, H.A.; Sayed, A.A.; Othman, A.A. Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease: Systematic Review and Meta-analysis. J. Gastrointest. Liver Dis. JGLD 2017, 26, 59–67. [Google Scholar] [CrossRef]
- Heebøll, S.; Kreuzfeldt, M.; Hamilton-Dutoit, S.; Kjær Poulsen, M.; Stødkilde-Jørgensen, H.; Møller, H.J.; Jessen, N.; Thorsen, K.; Kristina Hellberg, Y.; Bønløkke Pedersen, S.; et al. Placebo-controlled, randomised clinical trial: High-dose resveratrol treatment for non-alcoholic fatty liver disease. Scand. J. Gastroenterol. 2016, 51, 456–464. [Google Scholar] [CrossRef]
- Marchesini, G.; Babini, M. Nonalcoholic fatty liver disease and the metabolic syndrome. Minerva Cardioangiol. 2006, 54, 229–239. [Google Scholar]
- Salamone, F.; Galvano, F.; Marino, A.; Paternostro, C.; Tibullo, D.; Bucchieri, F.; Mangiameli, A.; Parola, M.; Bugianesi, E.; Volti, G.L. Silibinin improves hepatic and myocardial injury in mice with nonalcoholic steatohepatitis. Dig. Liver Dis. 2012, 44, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Salamone, F.; Galvano, F.; Cappello, F.; Mangiameli, A.; Barbagallo, I.; Volti, G.L. Silibinin modulates lipid homeostasis and inhibits nuclear factor kappa B activation in experimental nonalcoholic steatohepatitis. Transl. Res. 2012, 159, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, L.; Portillo, M.P.; Hijona, E.; Bujanda, L. Effects of resveratrol and other polyphenols in hepatic steatosis. World J. Gastroenterol. 2014, 20, 7366–7380. [Google Scholar] [CrossRef] [PubMed]
- Gambini, J.; Inglés, M.; Olaso, G.; Lopez-Grueso, R.; Bonet-Costa, V.; Gimeno-Mallench, L.; Mas-Bargues, C.; Abdelaziz, K.M.; Gomez-Cabrera, M.C.; Vina, J.; et al. Properties of Resveratrol: In Vitro and In Vivo Studies about Metabolism, Bioavailability, and Biological Effects in Animal Models and Humans. Oxid. Med. Cell. Longev. 2015, 2015, 837042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resveratrol: French Paradox Revisited. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/22822401 (accessed on 17 March 2020).
- Asghari, S.; Asghari-Jafarabadi, M.; Somi, M.-H.; Ghavami, S.-M.; Rafraf, M. Comparison of Calorie-Restricted Diet and Resveratrol Supplementation on Anthropometric Indices, Metabolic Parameters, and Serum Sirtuin-1 Levels in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Controlled Clinical Trial. J. Am. Coll. Nutr. 2018, 37, 223–233. [Google Scholar] [CrossRef]
- Hung, L.M.; Chen, J.K.; Huang, S.S.; Lee, R.S.; Su, M.J. Cardioprotective effect of resveratrol, a natural antioxidant derived from grapes. Cardiovasc. Res. 2000, 47, 549–555. [Google Scholar] [CrossRef]
- Bo, S.; Ciccone, G.; Castiglione, A.; Gambino, R.; De Michieli, F.; Villois, P.; Durazzo, M.; Cavallo-Perin, P.; Cassader, M. Anti-inflammatory and antioxidant effects of resveratrol in healthy smokers a randomized, double-blind, placebo-controlled, cross-over trial. Curr. Med. Chem. 2013, 20, 1323–1331. [Google Scholar] [CrossRef]
- Faghihzadeh, F.; Adibi, P.; Rafiei, R.; Hekmatdoost, A. Resveratrol supplementation improves inflammatory biomarkers in patients with nonalcoholic fatty liver disease. Nutr. Res. 2014, 34, 837–843. [Google Scholar] [CrossRef]
- Effects of Chronic Calorie Restriction or Dietary Resveratrol Supplementation on Insulin Sensitivity Markers in a Primate, Microcebus Murinus. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/22479589 (accessed on 17 March 2020).
- Prevention of Obesity by Dietary Resveratrol: How Strong Is the Evidence? Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC5154689/ (accessed on 17 March 2020).
- Resveratrol Suppresses Body Mass Gain in a Seasonal Non-Human Primate Model of Obesity. Available online: https://www.researchgate.net/publication/44693880_Resveratrol_suppresses_body_mass_gain_in_a_seasonal_non-human_primate_model_of_obesity (accessed on 17 March 2020).
- Zhang, C.; Yuan, W.; Fang, J.; Wang, W.; He, P.; Lei, J.; Wang, C. Efficacy of Resveratrol Supplementation against Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Placebo-Controlled Clinical Trials. PLoS ONE 2016, 11, e0161792. [Google Scholar] [CrossRef] [Green Version]
- Poulsen, M.K.; Nellemann, B.; Bibby, B.M.; Stødkilde-Jørgensen, H.; Pedersen, S.B.; Grønbaek, H.; Nielsen, S. No effect of resveratrol on VLDL-TG kinetics and insulin sensitivity in obese men with nonalcoholic fatty liver disease. Diabetes Obes. Metab. 2018, 20, 2504–2509. [Google Scholar] [CrossRef]
- Poulsen, M.M.; Vestergaard, P.F.; Clasen, B.F.; Radko, Y.; Christensen, L.P.; Stødkilde-Jørgensen, H.; Møller, N.; Jessen, N.; Pedersen, S.B.; Jørgensen, J.O.L. High-dose resveratrol supplementation in obese men: An investigator-initiated, randomized, placebo-controlled clinical trial of substrate metabolism, insulin sensitivity, and body composition. Diabetes 2013, 62, 1186–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, S.; Das, D.K. Resveratrol: A therapeutic promise for cardiovascular diseases. Recent Pat. Cardiovasc. Drug Discov. 2007, 2, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Timmers, S.; Konings, E.; Bilet, L.; Houtkooper, R.H.; van de Weijer, T.; Goossens, G.H.; Hoeks, J.; van der Krieken, S.; Ryu, D.; Kersten, S.; et al. Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metab. 2011, 14, 612–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. A Nonparametric “Trim and Fill” Method of Accounting for Publication Bias in Meta-Analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar] [CrossRef]
- Asghari, S.; Rafraf, M.; Farzin, L.; Asghari-Jafarabadi, M.; Ghavami, S.-M.; Somi, M.-H. Effects of Pharmacologic Dose of Resveratrol Supplementation on Oxidative/Antioxidative Status Biomarkers in Nonalcoholic Fatty Liver Disease Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Adv. Pharm. Bull. 2018, 8, 307–317. [Google Scholar] [CrossRef] [Green Version]
- Chachay, V.S.; Macdonald, G.A.; Martin, J.H.; Whitehead, J.P.; O’Moore–Sullivan, T.M.; Lee, P.; Franklin, M.; Klein, K.; Taylor, P.J.; Ferguson, M.; et al. Resveratrol Does Not Benefit Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2014, 12, 2092–2103.e6. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Zhao, X.; Ran, L.; Wan, J.; Wang, X.; Qin, Y.; Shu, F.; Gao, Y.; Yuan, L.; Zhang, Q.; et al. Resveratrol improves insulin resistance, glucose and lipid metabolism in patients with non-alcoholic fatty liver disease: A randomized controlled trial. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2015, 47, 226–232. [Google Scholar] [CrossRef]
- Faghihzadeh, F.; Adibi, P.; Hekmatdoost, A. The effects of resveratrol supplementation on cardiovascular risk factors in patients with non-alcoholic fatty liver disease: A randomised, double-blind, placebo-controlled study. Br. J. Nutr. 2015, 114, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Charytoniuk, T.; Drygalski, K.; Konstantynowicz-Nowicka, K.; Berk, K.; Chabowski, A. Alternative treatment methods attenuate the development of NAFLD: A review of resveratrol molecular mechanisms and clinical trials. Nutrition 2017, 34, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Theodotou, M.; Fokianos, K.; Moniatis, D.; Kadlenic, R.; Chrysikou, A.; Aristotelous, A.; Mouzouridou, A.; Diakides, J.; Stavrou, E. Effect of resveratrol on non-alcoholic fatty liver disease. Exp. Ther. Med. 2019, 18, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiskirchen, S.; Weiskirchen, R. Resveratrol: Is It Really Good for Liver Health? Available online: http://hepatmon.com/en/articles/12074.html (accessed on 20 March 2020).
- Krige, J.E.; Beckingham, I.J. ABC of diseases of liver, pancreas, and biliary system: Portal hypertension-2. Ascites, encephalopathy, and other conditions. BMJ 2001, 322, 416–418. [Google Scholar] [CrossRef]
- Gowda, S.; Desai, P.B.; Hull, V.V.; Math, A.A.K.; Vernekar, S.N.; Kulkarni, S.S. A review on laboratory liver function tests. Pan Afr. Med. J. 2009, 3, 17. [Google Scholar]
- Baur, J.A.; Pearson, K.J.; Price, N.L.; Jamieson, H.A.; Lerin, C.; Kalra, A.; Prabhu, V.V.; Allard, J.S.; Lopez-Lluch, G.; Lewis, K.; et al. Resveratrol improves health and survival of mice on a high-calorie diet. Nature 2006, 444, 337–342. [Google Scholar] [CrossRef]
- Chen, X.-X.; Xu, Y.-Y.; Wu, R.; Chen, Z.; Fang, K.; Han, Y.-X.; Yu, Y.; Huang, L.-L.; Peng, L.; Ge, J.-F. Resveratrol Reduces Glucolipid Metabolic Dysfunction and Learning and Memory Impairment in a NAFLD Rat Model: Involvement in Regulating the Imbalance of Nesfatin-1 Abundance and Copine 6 Expression. Front. Endocrinol. 2019, 10, 434. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLOS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Qian, L.-Y.; Tu, J.-F.; Ding, Y.-H.; Pang, J.; Che, X.-D.; Zou, H.; Huang, D.-S. Association of blood pressure level with nonalcoholic fatty liver disease in nonhypertensive population. Medicine 2016, 95. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| No. | Study Description | Intervention | Sample Characteristics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference/Year/Country/Sponsorship | Blinding/ Crossover (Y/N) | Focus on | ROB | Form/RSVtype | RSV Dose (mg/day) | Duration of RSV Administration (days)/ Comparator | N Total Randomized/ Analyzed | Age Years (mean ± SD) | Males (n/%) | BMI Baseline (kg/m2): RSV Group (Mean ± SD) | BMI Baseline (kg/m2): Control Group (mean ± SD) | |
| 1 | Asghari et al./ 2018a/Iran/ Non-industry | SB/N | Liver enzymes, lipid and insulin levels, insulin resistance | 5 | Capsules, pure trans-RSV | 600 | 84/placebo | 60/60 | 39.53 ± 6.72 | 35/58.33 | 30.78 (±3.1) | 30.41 (±3.39) |
| 2 | Asghari et al./ 2018b/Iran/ Non-industry | DB/N | Liver enzymes, levels | 5 | Capsules, pure trans-RSV | 600 | 84/placebo | 60/60 | 39.25 ± 26.53 | 40/66.66 | ND | ND |
| 3 | Chachay et al./ 2014/China/Non-industry | DB/N | Liver enzymes, lipid insulin, bilirubin, IL-6, CRP, TNF-α levels, DBP, SBP, insulin resistance | 5 | Capsules | 3000 | 56/placebo | 20/20 | 48.15 ± 11.73 | 20/100 | 31.8 (30.2–37) | 31.2 (27.4–39.3) |
| 4 | Chen et al./ 2015/Australia/Non-industry | DB/N | Insulin resistance, glucose and lipid metabolism | 5 | Capsules (from natural products) | 600 | 90/placebo | 60/60 | 44.30 ± 10.5 | 42/70 | 25.3 (±2.11) | 26.2 (±3.08) |
| 5 | Faghihzadeh et al./ 2015/Iran/Non-industry | DB/N | Liver enzymes, lipid insulin, glucose, bilirubin, levels, DBP, SBP, insulin resistance | 3 | Capsules | 500 | 84/placebo | 50/48 | 41.16 ± 9.81 | 35/70 | 28.35 (±3.49) | 28.75 (±3.5) |
| 6 | Faghihzadeh et al./ 2014/Iran/Non-industry | DB/N | Liver enzymes, lipid, bilirubin, IL-6, CRP, TNF-α levels | 3 | Capsules, pure trans-RSV | 500 | 84/placebo | 50/48 | 41.16 ± 9.81 | 35/70 | 28.35 (±3.49) | 28.75 (±33.5 |
| 7 | Heebøll et al./ 2016/Denmark/Non-industry | DB/N | Liver enzymes, lipid insulin, glucose, bilirubin, TNF-α levels, DBP, SBP, insulin resistance | 3 | Capsules, pure trans-RSV | 1500 | 180/placebo | 28/26 | 43.2 (22–67) PBO 43,5 (21–69) ^^ | 17/65.38 | 32,1 (±3.1) | 32 (±5.4) |
| No. | Reference/Year/Country/Sponsorship | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data Addressed (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | No. Of Low Assessments |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Asghari et al./2018a/Iran/ Non-industry | L | L | L | ? | L | L | ? | 5 |
| 2 | Asghari et al./2018b/Iran/ Non-industry | L | L | L | ? | L | L | ? | 5 |
| 3 | Chachay et al./2014/China/Non-industry | L | L | L | ? | L | L | ? | 5 |
| 4 | Chen et al./2015/Australia/Non-industry | L | L | L | ? | L | L | ? | 5 |
| 5 | Faghihzadeh et al./2015/Iran/Non-industry | ? | ? | L | ? | L | L | ? | 3 |
| 6 | Faghihzadeh et al./2014/Iran/Non-industry | ? | ? | L | ? | L | L | ? | 3 |
| 7 | Heebøll et al./2016/Denmark/Non-industry | H | H | L | ? | L | L | ? | 3 |
| Outcome | SMD | 95%CI | Z | p |
|---|---|---|---|---|
| AST | 0.052 | −0.202, 0.307 | 0.404 | 0.686 |
| Body weight | −0.061 | −0.334, 0.212 | −0.438 | 0.661 |
| BMI | −0.076 | −0.364, 0.212 | −0.518 | 0.604 |
| WC | −0.075 | −0.385. 0.236 | −0.471 | 0.638 |
| Glucose | −0.184 | −0.585, 0.218 | −0.897 | 0.370 |
| Insulin | −0.178 | −0.948, 0.593 | −0.452 | 0.651 |
| TC | −0.053 | −0.401, 0.296 | −0.297 | 0.767 |
| TAG | −0.095 | −0.470, 0.280 | −0.496 | 0.620 |
| LDL | 0.225 | −0.122, 0.571 | 1.270 | 0.204 |
| HDL | −0.184 | −0.559, 0.191 | −0.959 | 0.337 |
| SBP | −0.035 | −0.379, 0.310 | −0.197 | 0.844 |
| DBP | 0.118 | −0.345, 0.580 | 0.498 | 0.618 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakubczyk, K.; Skonieczna-Żydecka, K.; Kałduńska, J.; Stachowska, E.; Gutowska, I.; Janda, K. Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease—A Meta-Analysis. Nutrients 2020, 12, 2435. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082435
Jakubczyk K, Skonieczna-Żydecka K, Kałduńska J, Stachowska E, Gutowska I, Janda K. Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease—A Meta-Analysis. Nutrients. 2020; 12(8):2435. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082435
Chicago/Turabian StyleJakubczyk, Karolina, Karolina Skonieczna-Żydecka, Justyna Kałduńska, Ewa Stachowska, Izabela Gutowska, and Katarzyna Janda. 2020. "Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease—A Meta-Analysis" Nutrients 12, no. 8: 2435. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12082435