Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
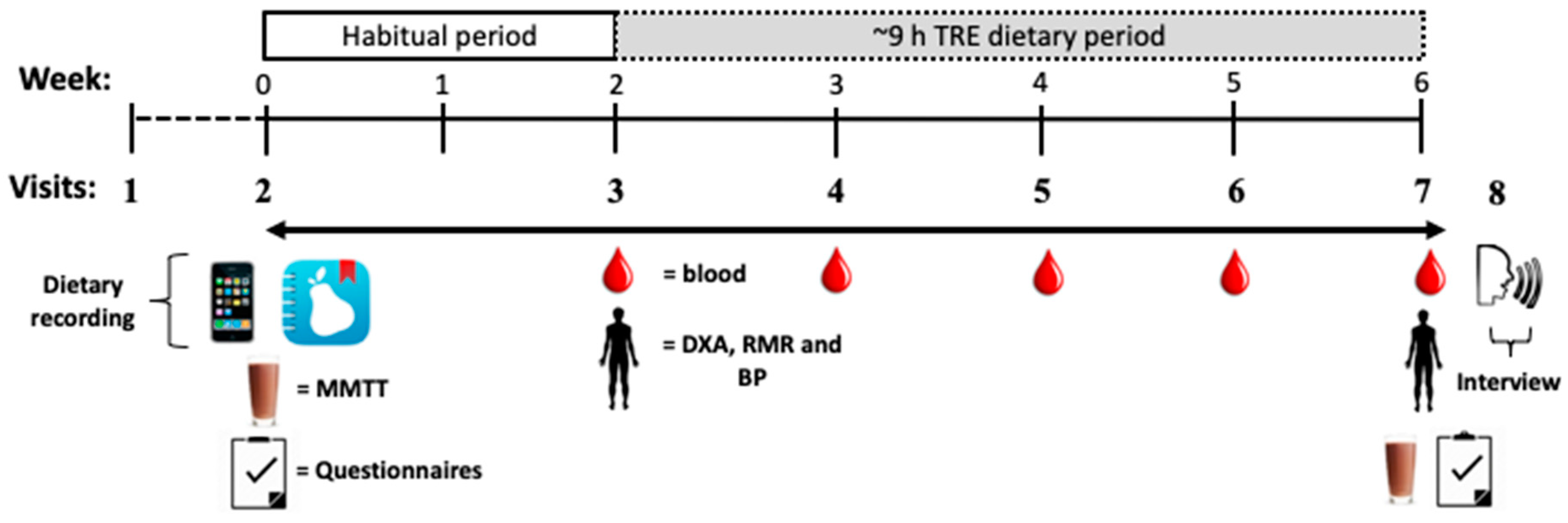
2.1. Study Design
2.2. Participants
2.3. Measurement Visits
2.4. Dietary Recordings and Analysis
2.5. Biochemical Analysis
2.6. Psychological Questionnaires and Analysis
2.7. Qualitative Interviews and Analysis
2.8. Statistical Analyses
3. Results
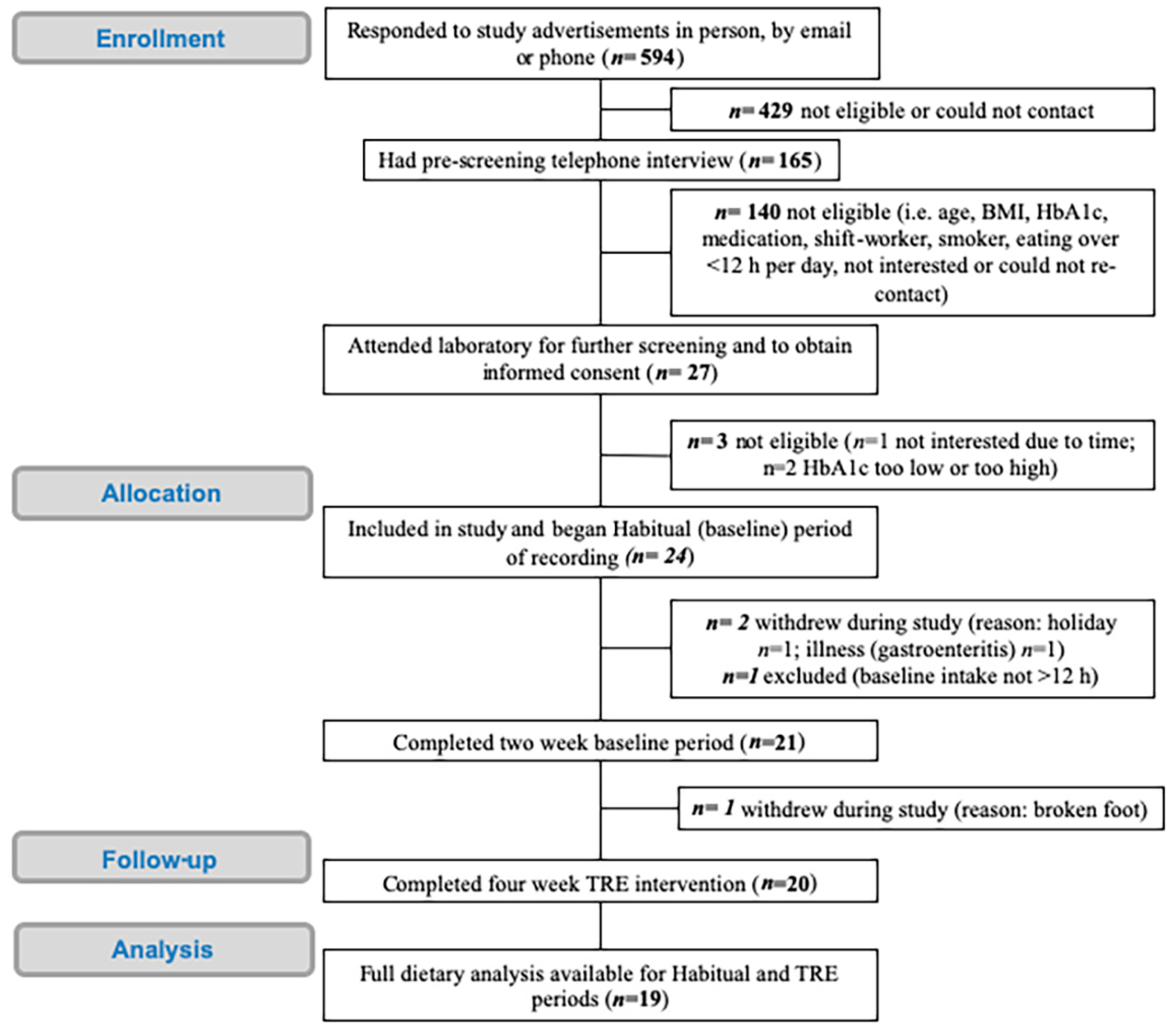
3.1. Participant Recruitment and Characteristics
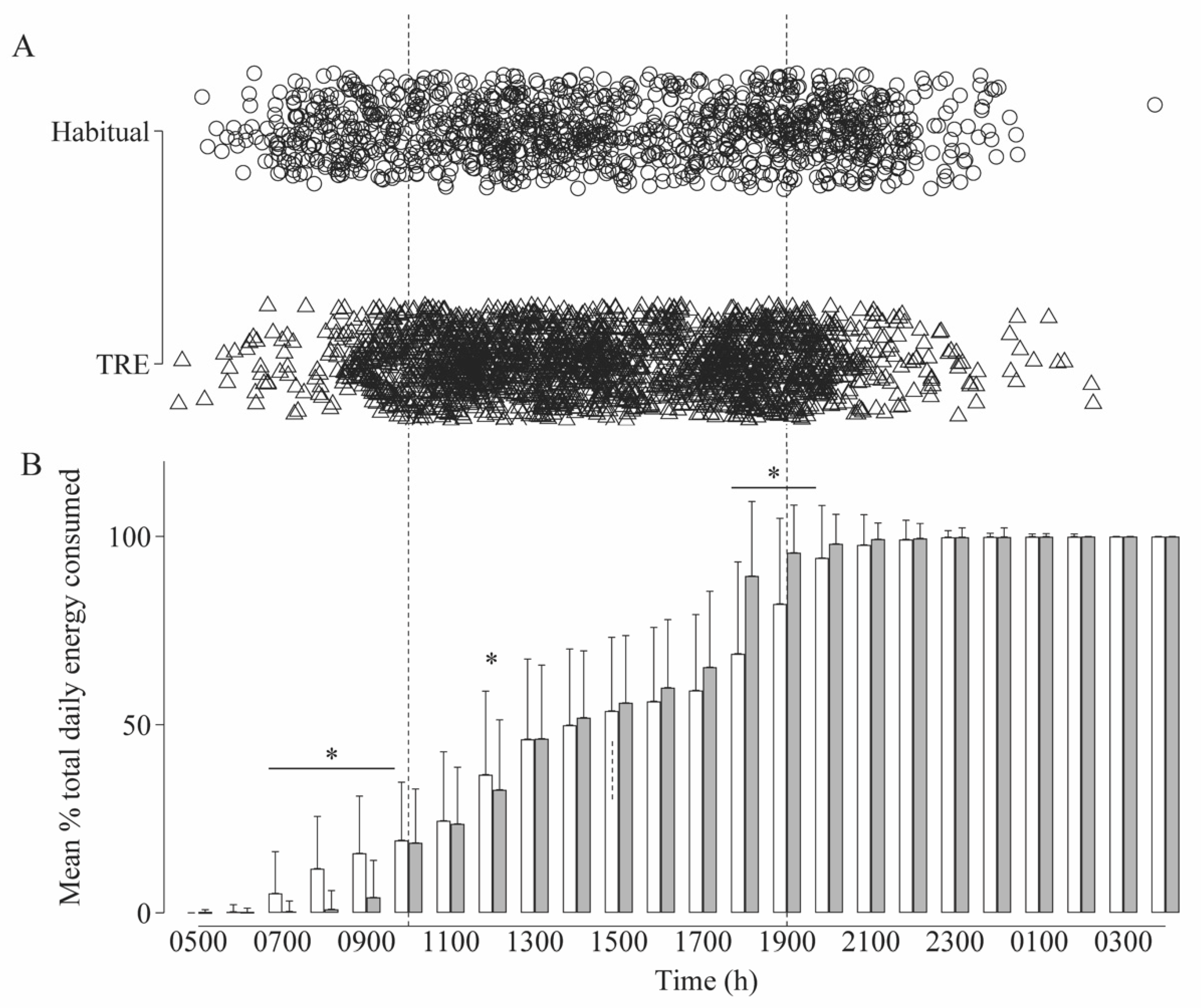
3.2. Dietary Analysis and Adherence
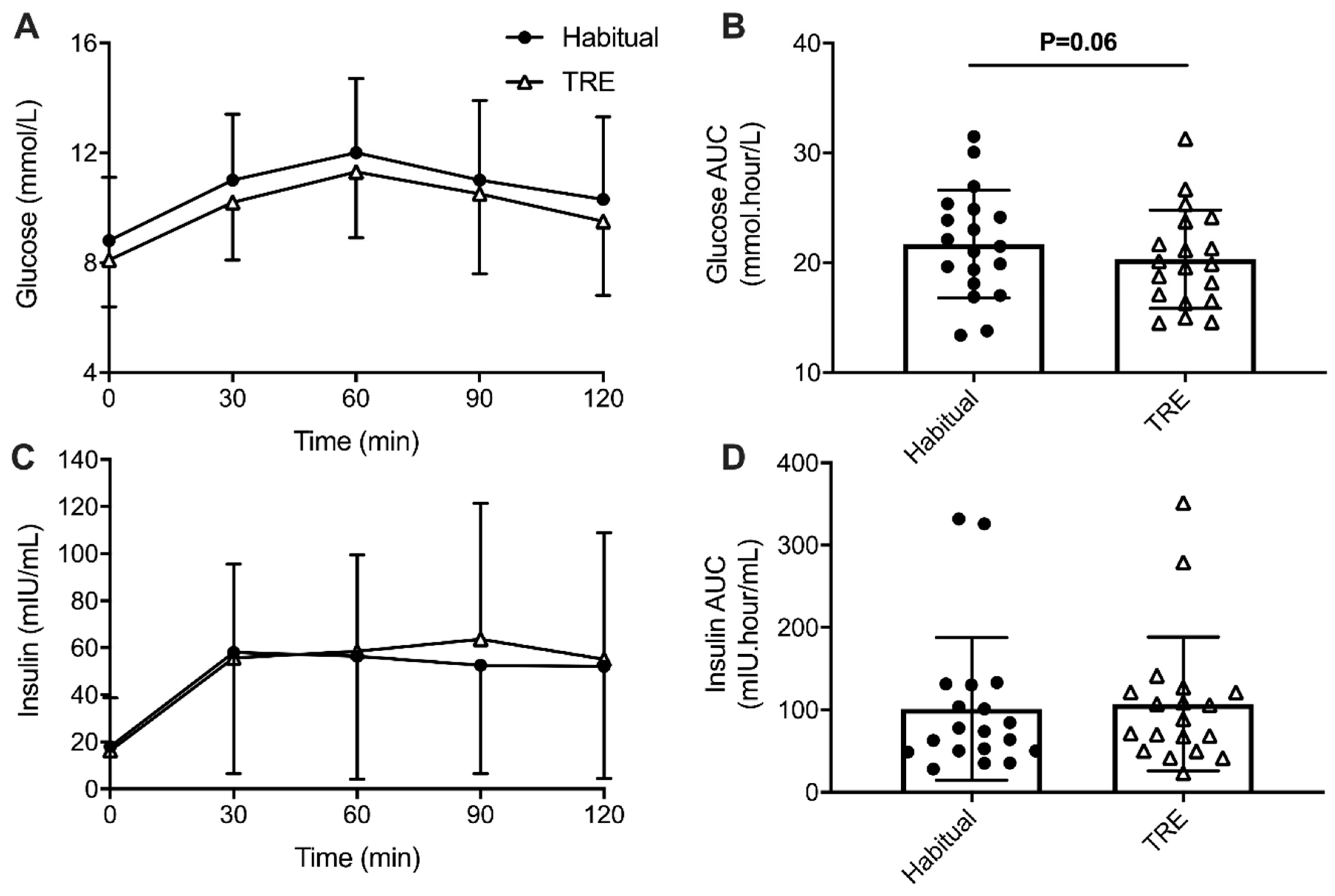
3.3. Fasting Biochemical Measures and Mixed Meal Tolerance Test Responses
3.4. Physiological Data
3.5. Psychological Data
3.5.1. Psychological Wellbeing
3.5.2. Cognitive Functioning
3.6. Qualitative Questionnaire Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Antoni, R.; Robertson, T.M.; Robertson, M.D.; Johnston, J.D. A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. J. Nutr. Sci. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Panda, S. A smartphone app reveals erratic diurnal eating patterns in humans that can be modulated for health benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef] [PubMed]
- Kesztyüs, D.; Cermak, P.; Gulich, M.; Kesztyüs, T. Adherence to time-restricted feeding and impact on abdominal obesity in primary care patients: Results of a pilot study in a pre–post design. Nutrients 2019, 11, 2854. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.A.; Sypniewski, C.; Bensadon, B.A.; McLaren, C.; Donahoo, W.T.; Sibille, K.T.; Anton, S. Determinants of adherence in time-restricted feeding in older adults: Lessons from a pilot study. Nutrients 2020, 12, 874. [Google Scholar] [CrossRef] [Green Version]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef] [Green Version]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef] [Green Version]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-restricted feeding improves glucose tolerance in men at risk for type 2 diabetes: A randomized crossover trial. Obesity 2019, 27, 724–732. [Google Scholar] [CrossRef]
- Ravussin, E.; Beyl, R.A.; Poggiogalle, E.; Hsia, D.S.; Peterson, C.M. Early time-restricted feeding reduces appetite and increases fat oxidation but does not affect energy expenditure in humans. Obesity 2019, 27, 1244–1254. [Google Scholar] [CrossRef]
- Eckel-Mahan, K.; Sassone-Corsi, P. Metabolism and the circadian clock converge. Physiol. Rev. 2013, 93, 107–135. [Google Scholar] [CrossRef] [PubMed]
- Hawley, J.A.; Sassone-Corsi, P.; Zierath, J.R. Chrono-nutrition for the prevention and treatment of obesity and type 2 diabetes: From mice to men. Diabetologia 2020. [Google Scholar] [CrossRef] [PubMed]
- Lundell, L.S.; Parr, E.B.; Devlin, B.L.; Ingerslev, L.R.; Altıntaş, A.; Sato, S.; Sassone-Corsi, P.; Barrès, R.; Zierath, J.R.; Hawley, J.A. Time-restricted feeding alters lipid and amino acid metabolite rhythmicity without perturbing clock gene expression. Nat. Commun. 2020, 11, 4643. [Google Scholar] [CrossRef] [PubMed]
- Radziuk, J.; Pye, S. Diurnal rhythm in endogenous glucose production is a major contributor to fasting hyperglycaemia in type 2 diabetes. Suprachiasmatic deficit or limit cycle behaviour? Diabetologia 2006, 49, 1619–1628. [Google Scholar] [CrossRef] [Green Version]
- Van Cauter, E.; Polonsky, K.S.; Scheen, A.J. Roles of circadian rhythmicity and sleep in human glucose regulation*. Endocr. Rev. 1997, 18, 716–738. [Google Scholar] [CrossRef] [Green Version]
- Jakubowicz, D.; Wainstein, J.; Ahren, B.; Landau, Z.; Bar-Dayan, Y.; Froy, O. Fasting until noon triggers increased postprandial hyperglycemia and impaired insulin response after lunch and dinner in individuals with type 2 diabetes: A randomized clinical trial. Diabetes Care 2015, 38, 1820–1826. [Google Scholar] [CrossRef] [Green Version]
- Mason, I.C.; Qian, J.; Adler, G.K.; Scheer, F.A.J.L. Impact of circadian disruption on glucose metabolism: Implications for type 2 diabetes. Diabetologia 2020, 63, 462–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouda, M.; Matsukawa, M.; Iijima, H. Associations between eating habits and glycemic control and obesity in Japanese workers with type 2 diabetes mellitus. DMSO 2018, 11, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Imai, S.; Kajiyama, S.; Hashimoto, Y.; Yamane, C.; Miyawaki, T.; Ozasa, N.; Tanaka, M.; Fukui, M. Divided consumption of late-night-dinner improves glycemic excursions in patients with type 2 diabetes: A randomized cross-over clinical trial. Diabetes Res. Clin. Pract. 2017, 129, 206–212. [Google Scholar] [CrossRef] [Green Version]
- Arnason, T.G.; Bowen, M.W.; Mansell, K.D. Effects of intermittent fasting on health markers in those with type 2 diabetes: A pilot study. World J. Diabetes 2017, 8, 154. [Google Scholar] [CrossRef]
- Gregg, E.W.; Li, Y.; Wang, J.; Rios Burrows, N.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in diabetes-related complications in the United States, 1990–2010. N. Engl. J. Med. 2014, 370, 1514–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, N.A.; Dyer, K.A.; Buckley, J.D.; Brinkworth, G.D.; Coates, A.M.; Parfitt, G.; Howe, P.R.C.; Noakes, M.; Murphy, K.J. Comparison of two low-fat diets, differing in protein and carbohydrate, on psychological wellbeing in adults with obesity and type 2 diabetes: A randomised clinical trial. Nutr. J. 2018, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Heilbronn, L.K.; Noakes, M.; Clifton, P.M. Effect of energy restriction, weight loss, and diet composition on plasma lipids and glucose in patients with type 2 diabetes. Diabetes Care 1999, 22, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Vijan, S.; Stuart, N.S.; Fitzgerald, J.T.; Ronis, D.L.; Hayward, R.A.; Slater, S.; Hofer, T.P. Barriers to following dietary recommendations in Type 2 diabetes. Diabet. Med. 2005, 22, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, R.; Mishra, P.; Mishra, J.; Parminder, S.; Mishra, B.P. Psychiatric morbidity among diabetic patients: A hospital-based study. Ind. Psychiatry J. 2010, 19, 47–49. [Google Scholar] [CrossRef]
- Brown, S.A.; García, A.A.; Brown, A.; Becker, B.J.; Conn, V.S.; Ramírez, G.; Winter, M.A.; Sumlin, L.L.; Garcia, T.J.; Cuevas, H.E. Biobehavioral determinants of glycemic control in type 2 diabetes: A systematic review and meta-analysis. Patient Educ. Couns. 2016, 99, 1558–1567. [Google Scholar] [CrossRef] [Green Version]
- Martens, C.R.; Rossman, M.J.; Mazzo, M.R.; Jankowski, L.R.; Nagy, E.E.; Denman, B.A.; Richey, J.J.; Johnson, S.A.; Ziemba, B.P.; Wang, Y.; et al. Short-term time-restricted feeding is safe and feasible in non-obese healthy midlife and older adults. GeroScience 2020, 42, 667–686. [Google Scholar] [CrossRef]
- Carter, S.; Clifton, P.M.; Keogh, J.B. Effect of intermittent compared with continuous energy restricted diet on glycemic control in patients with type 2 diabetes: A randomized noninferiority trial. JAMA Netw. Open 2018, 1, e180756. [Google Scholar] [CrossRef]
- Terman, M.; Terman, J.S. Light therapy for seasonal and nonseasonal depression: Efficacy, protocol, safety, and side effects. CNS Spectr. 2005, 10, 647–663. [Google Scholar] [CrossRef] [Green Version]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. 1), 5–41. [Google Scholar]
- Parr, E.; Devlin, B.; Callahan, M.; Radford, B.; Blankenship, J.; Dunstan, D.; Hawley, J. Effects of providing high-fat versus high-carbohydrate meals on daily and postprandial physical activity and glucose patterns: A randomised controlled trial. Nutrients 2018, 10, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leech, R.M.; Worsley, A.; Timperio, A.; McNaughton, S.A. Understanding meal patterns: Definitions, methodology and impact on nutrient intake and diet quality. Nutr. Res. Rev. 2015, 28, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Richardson, J.; Iezzi, A.; Khan, M.A.; Maxwell, A. Validity and reliability of the assessment of quality of life (AQoL)-8D multi-attribute utility instrument. Patient 2014, 7, 85–96. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar]
- Bohn, K.; Doll, H.A.; Cooper, Z.; O’Connor, M.; Palmer, R.L.; Fairburn, C.G. The measurement of impairment due to eating disorder psychopathology. Behav. Res. Ther. 2008, 46, 1105–1110. [Google Scholar] [CrossRef]
- Darby, D.G.; Pietrzak, R.H.; Fredrickson, J.; Woodward, M.; Moore, L.; Fredrickson, A.; Sach, J.; Maruff, P. Intraindividual cognitive decline using a brief computerized cognitive screening test. Alzheimer’s Dement. 2012, 8, 95–104. [Google Scholar] [CrossRef]
- Palta, P.; Schneider, A.L.C.; Biessels, G.J.; Touradji, P.; Hill-Briggs, F. Magnitude of cognitive dysfunction in adults with type 2 diabetes: A meta-analysis of six cognitive domains and the most frequently reported neuropsychological tests within domains. J. Int. Neuropsychol. Soc. 2014, 20, 278–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredrickson, J.; Maruff, P.; Woodward, M.; Moore, L.; Fredrickson, A.; Sach, J.; Darby, D. Evaluation of the usability of a brief computerized cognitive screening test in older people for epidemiological studies. Neuroepidemiology 2010, 34, 65–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawthorne, G.; Richardson, J.; Day, N. Using the Assessment of Quality of Life (AQOL) Version 1; Centre for Health Program Evaluation: Melbourne, Australia, 2009. [Google Scholar]
- Parr, E.B.; Devlin, B.L.; Radford, B.E.; Hawley, J.A. A delayed morning and earlier evening time-restricted feeding protocol for improving glycemic control and dietary adherence in men with overweight/obesity: A randomized controlled trial. Nutrients 2020, 12, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Derman, K.D.; Hawley, J.A.; Noakes, T.D.; Dennis, S.C. Fuel kinetics during intense running and cycling when fed carbohydrate. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 74, 36–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anton, S.D.; Lee, S.A.; Donahoo, W.T.; McLaren, C.; Manini, T.; Leeuwenburgh, C.; Pahor, M. The Effects of Time Restricted Feeding on Overweight, Older Adults: A Pilot Study. Nutrients 2019, 11, 1500. [Google Scholar] [CrossRef] [Green Version]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Wiseman, E.; Pavlou, V.; Lin, S.; Oliveira, M.L.; Varady, K.A. Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial in adults with obesity. Cell Metab. 2020, 32. [Google Scholar] [CrossRef]
- Monnier, L.; Colette, C.; Dejager, S.; Owens, D. Magnitude of the dawn phenomenon and its impact on the overall glucose exposure in type 2 diabetes: Is this of concern? Diabetes Care 2013, 36, 4057–4062. [Google Scholar] [CrossRef] [Green Version]
- Parr, E.B.; Heilbronn, L.K.; Hawley, J.A. A time to eat and a time to exercise. Exerc. Sport Sci. Rev. 2020, 48, 4–10. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Burgess, H.J.; Varady, K.A. Effect of 8-h time-restricted feeding on sleep quality and duration in adults with obesity. Appl. Physiol. Nutr. Metab. 2019, 44, 903–906. [Google Scholar] [CrossRef]
- Fitzgerald, K.C.; Vizthum, D.; Henry-Barron, B.; Schweitzer, A.; Cassard, S.D.; Kossoff, E.; Hartman, A.L.; Kapogiannis, D.; Sullivan, P.; Baer, D.J.; et al. Effect of intermittent vs. daily calorie restriction on changes in weight and patient-reported outcomes in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2018, 23, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Teng, N.I.M.F.; Shahar, S.; Manaf, Z.A.; Das, S.K.; Taha, C.S.C.; Ngah, W.Z.W. Efficacy of fasting calorie restriction on quality of life among aging men. Physiol. Behav. 2011, 104, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.A.; Rezaei, M.; Amiri Baghni, S.; Seifi, M. Effect of fasting on mental health in the general population of Kermanshah, Iran. JFH 2014, 2. [Google Scholar] [CrossRef]
- Michalsen, A.; Frey, U.H.; Merse, S.; Siffert, W.; Dobos, G.J. Hunger and mood during extended fasting are dependent on the GNB3 C825T polymorphism. Ann. Nutr. Metab. 2009, 54, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Horie, N.C.; Serrao, V.T.; Simon, S.S.; Gascon, M.R.P.; dos Santos, A.X.; Zambone, M.A.; de Freitas, M.M.d.B.; Cunha-Neto, E.; Marques, E.L.; Halpern, A.; et al. Cognitive effects of intentional weight loss in elderly obese individuals with mild cognitive impairment. J. Clin. Endocrinol. Metab. 2016, 101, 1104–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benau, E.M.; Orloff, N.C.; Janke, E.A.; Serpell, L.; Timko, C.A. A systematic review of the effects of experimental fasting on cognition☆. Appetite 2014, 77, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Acheson, K.J.; Zahorska-Markiewicz, B.; Pittet, P.; Anantharaman, K.; Jéquier, E. Caffeine and coffee: Their influence on metabolic rate and substrate utilization in normal weight and obese individuals. Am. J. Clin. Nutr. 1980, 33, 989–997. [Google Scholar] [CrossRef]
- Macdiarmid, J.; Blundell, J. Dietary under-reporting: What people say about recording their food intake. Eur. J. Clin. Nutr. 1997, 51, 199–200. [Google Scholar] [CrossRef] [Green Version]
- Mifsud, M.; Molines, M.; Cases, A.-S.; N’Goala, G. It’s MY health care program: Enhancing patient adherence through psychological ownership. Soc. Sci. Med. 2019, 232, 307–315. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 19) | Males (n = 9) | Females (n = 10) | |
|---|---|---|---|
| Age (y) | 50.2 ± 8.9 | 48.7 ± 10.0 | 51.6 ± 8.0 |
| Body mass (kg) * | 99.7 ± 12.7 | 99.8 ± 12.6 | 101.1 ± 12.5 |
| Height (m) | 1.71 ± 0.09 | 1.78 ± 0.04 | 1.66 ± 0.08 |
| BMI (kg/m2) | 34.4 ± 4.8 | 31.4 ± 3.4 | 36.8 ± 4.8 |
| Baseline HbA1c (% (mmol/mol)) | 7.6 ± 1.1 (59 ± 12) | 7.8 ± 1.1 (66 ± 12) | 7.1 ± 0.7 (54 ± 8) |
| Years diagnosed T2D | 3.4 ± 3.1 | 4.7 ± 3.5 | 2.6 ± 2.5 |
| MEQ-SA | 56 ± 11 | 55 ± 11 | 57 ± 11 |
| Habitual Period | TRE Period | p | |
|---|---|---|---|
| Energy (kJ/d) | 8399 ± 2864 | 8566 ± 2704 | 0.42 |
| Protein (g/d) | 95 ± 35 | 97 ± 37 | 0.66 |
| Protein (% of TEI) | 19.6 ± 5.7 | 19.2 ± 5.6 | 0.29 |
| Total fat (g/d) | 94 ± 45 | 96 ± 42 | 0.67 |
| Saturated fat (g/d) | 34 ± 18 | 35 ± 18 | 0.53 |
| Polyunsaturated fat (g/d) | 16 ± 10 | 16 ± 10 | 0.65 |
| Monounsaturated fat (g/d) | 36 ± 20 | 37 ± 18 | 0.78 |
| Total fat (% of TEI) | 41.4 ± 10.5 | 41.8 ± 11.2 | 0.68 |
| Carbohydrate (g/d) | 175 ± 86 | 181 ± 86 | 0.37 |
| Carbohydrate (% of TEI) | 34.9 ± 11.6 | 35.3 ± 12.1 | 0.65 |
| Sugars (g/d) | 55 ± 31 | 55 ± 33 | 0.99 |
| Fibre (g/d) | 25 ± 11 | 25 ± 12 | 0.86 |
| Alcohol (g/d *) | 4 ± 14 | 4 ± 15 | 0.89 |
| Alcohol (% of TEI) | 1.4 ± 4.8 | 1.3 ± 4.4 | 0.76 |
| Vitamin C (mg/d) | 70 ± 54 | 78 ± 70 | 0.13 |
| Sodium (mg/d) | 2834 ± 1475 | 2762 ± 1352 | 0.49 |
| Potassium (mg/d) | 2769 ± 1009 | 2738 ± 981 | 0.68 |
| Calcium (mg/d) | 830 ± 449 | 822 ± 505 | 0.84 |
| n, Days | Adherent (Time Data) | Non-Adherent (Time Data) | Total Self-Report |
|---|---|---|---|
| Adherent (self-report) | 302 | 55 | 357 (68%) |
| Non-adherent (self-report) | 23 | 73 | 96 (18%) |
| Not answered | 53 | 18 | 71 (14%) |
| Total time data | 378 (72%) | 146 (28%) | 524 (100%) |
| TRE-Adherent Days (n = 378) | TRE-Non Adherent Days (n = 146) | p | |
|---|---|---|---|
| Energy (kJ/d) | 8278 ± 2556 | 9312 ± 2936 | <0.001 |
| Protein (g/d) | 97 ± 36 | 96 ± 38 | 0.75 |
| Protein (% of TEI) | 20 ± 6 | 18 ± 6 | <0.001 |
| Total fat (g/d) | 96 ± 43 | 96 ± 39 | 0.99 |
| Saturated fat (g/d) | 35 ± 18 | 35 ± 17 | 0.97 |
| Polyunsaturated fat (g/d) | 16 ± 9 | 16 ± 10 | 0.72 |
| Monounsaturated fat (g/d) | 37 ± 18 | 36 ± 17 | 0.79 |
| Total fat (% of TEI) | 43 ± 11 | 39 ± 10 | <0.001 |
| Carbohydrate (g/d) | 167 ± 78 | 216 ± 96 | <0.001 |
| Carbohydrate (% of TEI) | 34 ± 12 | 39 ± 11 | <0.001 |
| Sugars (g/d) | 52 ± 33 | 62 ± 32 | 0.001 |
| Fibre (g/d) | 24 ± 11 | 27 ± 14 | 0.006 |
| Alcohol (g/d *) | 2 ± 7 | 9 ± 24 | <0.001 |
| Alcohol (% of TEI) | 1 ± 3 | 3 ± 7 | <0.001 |
| Vitamin C (mg/d) | 77 ± 66 | 81 ± 80 | 0.51 |
| Sodium (mg/d) | 2705 ± 1297 | 2908 ± 1479 | 0.12 |
| Potassium (mg/d) | 2682 ± 922 | 2883 ± 1111 | 0.04 |
| Calcium (mg/d) | 812 ± 503 | 850 ± 513 | 0.44 |
| Habitual Period | TRE Period | d | p * | |
|---|---|---|---|---|
| HbA1c (%) (mmol/mol) | 7.6 ± 1.1 (60 ± 12) | 7.4 ± 1.0 (58 ± 11) | 0.17 | 0.053 |
| Glucose (mmol/L) | 8.4 ± 2.3 | 8.1 ± 1.8 | 0.18 | 0.29 |
| Insulin (mIU/mL) | 15.0 ± 15.2 | 17.7 ± 25.2 | 0.13 | 0.09 |
| Total cholesterol (mmol/L) | 4.6 ± 0.9 | 4.5 ± 0.8 | 0.13 | 0.16 |
| HDLC (mmol/L) | 1.1 ± 0.3 | 1.1 ± 0.3 | 0.01 | 0.75 |
| LDLC (mmol/L) | 2.6 ± 0.9 | 2.5 ± 0.8 | 0.17 | 0.22 |
| Triglycerides (mmol/L) | 1.8 ± 0.7 | 1.8 ± 0.8 | 0.00 | 0.78 |
| Habitual Period | TRE Period | d | p | |
|---|---|---|---|---|
| Total body mass (kg) * | 98.9 ± 12.7 | 98.1 ± 12.8 | 0.07 | 0.84 |
| Lean mass (kg) * | 56.3 ± 9.3 | 56.2 ± 9.6 | 0.01 | 0.97 |
| Fat mass (kg) * | 39.8 ± 10.3 | 39.0 ± 10.3 | 0.07 | 0.84 |
| Bone mass (kg) * | 2.8 ± 0.4 | 2.8 ± 0.3 | 0.00 | 1.00 |
| Resting energy expenditure (kcal/d) * | 1889 ± 298 | 1889 ± 310 | 0.00 | 1.00 |
| Blood pressure (BP) | ||||
| Systolic BP (mmHg) | 131 ± 12 | 126 ± 7 | 0.51 | 0.12 |
| Diastolic BP (mmHg) | 84 ± 6 | 80 ± 4 | 0.54 | 0.11 |
| Heart rate (beats per min) | 72 ± 15 | 66 ± 10 | 0.52 | 0.12 |
| Domain | Habitual | Post-TRE Intervention | t | d | p | |
|---|---|---|---|---|---|---|
| Depression, Anxiety and Stress Scale (DASS) | ||||||
| Depression | 6.42 ± 8.90 | 7.05 ± 9.71 | −0.277 | 0.07 | 0.79 | |
| Anxiety | 4.53 ± 4.56 | 6.42 ± 7.32 | −1.158 | 0.32 | 0.28 | |
| Stress | 7.68 ± 7.24 | 8.31 ± 8.51 | −0.287 | 0.08 | 0.78 | |
| Assessment of Quality of Life (AQoL-8D) | ||||||
| Independent living | 0.90 ± 0.12 | 0.92 ± 0.13 | −0.919 | 0.16 | 0.37 | |
| Happiness | 0.77 ± 0.15 | 0.76 ± 0.15 | 0.014 | 0.07 | 0.99 | |
| Mental health | 0.64 ± 0.13 | 0.63 ± 0.14 | 0.253 | 0.00 | 0.80 | |
| Coping | 0.77 ± 0.14 | 0.77 ± 0.17 | −0.01 | 0.00 | 0.92 | |
| Relationship value | 0.75 ± 0.18 | 0.75 ± 0.21 | −0.08 | 0.00 | 0.94 | |
| Self-worth | 0.83 ± 0.19 | 0.79 ± 0.17 | 1.15 | 0.22 | 0.27 | |
| Pain value | 0.74 ± 0.26 | 0.74 ± 0.26 | −0.10 | 0.00 | 0.92 | |
| Senses | 0.87 ± 0.08 | 0.87 ± 0.10 | −0.14 | 0.00 | 0.89 | |
| Pittsburgh Sleep Quality Index (PSQI) | ||||||
| Quality | 1.26 ± 0.87 | 1.21 ± 0.63 | 0.252 | 0.07 | 0.80 | |
| Latency | 1.37 ± 1.26 | 1.21 ± 1.13 | 0.718 | 0.13 | 0.48 | |
| Duration | 0.84 ± 0.76 | 0.84 ± 0.69 | 0.000 | 0.00 | 1.00 | |
| Efficiency | 0.74 ± 0.99 | 0.68 ± 1.00 | 0.170 | 0.04 | 0.87 | |
| Disturbance | 1.42 ± 0.51 | 1.53 ± 0.70 | −0.697 | 0.18 | 0.49 | |
| Medication | 0.42 ± 0.61 | 0.31 ± 0.47 | 0.567 | 0.20 | 0.58 | |
| Daytime sleepiness | 0.95 ± 0.85 | 0.89 ± 0.93 | 0.224 | 0.07 | 0.83 | |
| Global | 7.00 ± 4.29 | 6.68 ± 3.84 | 0.275 | 0.08 | 0.79 | |
| Cogstate Brief Battery (CBB) | ||||||
| Groton Maze Learning | 62.42 ± 20.14 | 50.42 ± 14.81 | 3.334 | 0.69 | 0.004 | |
| Identification ª | 2.75 ± 0.11 | 2.73 ± 0.05 | 0.539 | 0.25 | 0.60 | |
| Detection ᵇ | 2.52 ± 0.07 | 2.57 ± 0.07 | −2.616 | 0.71 | 0.02 | |
| One Card Learning | 0.91 ± 0.16 | 0.93 ± 0.14 | −0.534 | 0.13 | 0.60 | |
| Two Back ᶜ | 1.07 ± 0.35 | 1.11 ± 0.34 | −0.523 | 0.12 | 0.61 | |
| Eating Disorders Examination Questionnaire (EDE-Q) | ||||||
| Restricted | 1.97 ± 1.35 | 1.84 ± 1.44 | 0.429 | 0.09 | 0.67 | |
| Eating | 1.24 ± 1.91 | 1.62 ± 1.98 | −1.421 | 0.20 | 0.17 | |
| Shape | 2.42 ± 1.52 | 2.33 ± 1.53 | 0.268 | 0.06 | 0.78 | |
| Weight | 2.20 ± 1.21 | 2.27 ± 1.45 | −0.352 | 0.05 | 0.73 | |
| Global | 1.96 ± 1.28 | 2.02 ± 1.36 | −0.345 | 0.05 | 0.72 | |
| Clinical Impairment Assessment (CIA) | ||||||
| Total | 6.31 ± 10.23 | 7.89 ± 12.16 | −1.119 | 0.14 | 0.25 | |
| Theme | Sub-Theme | Sample Quote |
|---|---|---|
| Mornings or evenings were difficult (of note, participants generally reported having trouble with the morning OR the evening, not both) | Mornings: starting eating/drinking later was difficult because of hunger or missing the morning coffee and feeling like it impacted on the ability to function. | “Morning things... if you have morning things, then the 10 am breakfast is a bit difficult to do.” “Coffee was a big factor... I couldn’t function too well in the morning at all.” |
| Evenings: finishing eating earlier was difficult because of family, social (particularly on the weekends) or work commitments, or hunger later in the evening. | “Whether I could go for dinner or saying no to doing things especially during the week... because I would have to do them really early.” “I wasn’t hungry at night... I did have a couple of nights where I did feel hungry, but it started to dissipate, and I felt less hungry when I woke up.” | |
| Impact on hunger, eating behaviour and food choices | Hunger: Feeling hungry, or concerned about being hungry, or, feeling less hungry than expected particularly over time. | “You think 10 a.m. is a long time and then sometimes you didn’t have enough the night before and didn’t eat a lot and the next day you’re like, ’I should’ve eaten more last night... I am hungry.’” “Well at first, I thought I was going to struggle with being hungry, then coming to the conclusion of it, yeah, I was a lot more satisfied and not as hungry and didn’t feel like I needed to eat all the time.” |
| Emotional eating and night-time snacking: response to not being able to eat to manage negative emotions (e.g., stress, boredom), and breaking the habit of night-time snacking. | “Probably a little better for it [TRE]. I am prone to eating because I don’t know if boredom or something but when it’s there, you go and snack.” “I guess the main thing for me was I could avoid late night snacking... I was always struggling to stop that, but I guess it [TRE] helped me a lot to stop it totally” | |
| Healthy food or convenient food: either planning ahead to eat healthier, more substantiating meals to avoid evening hunger, or not having healthy options organised and therefore eating convenient food in order to eat before 1900 h. | “…by the time I got home, it was very difficult to cook dinner at that time. So, unless I had something pre-prepared, I was going to eat junk. I would have rather eaten slightly later than eat junk.” “I did sort of think I probably need to eat something healthier that is going to keep me going for a little bit longer because I am not going to have another opportunity to have anything else.” | |
| Positive or negative emotional reactions | Positive reaction: felt good about the routine, appreciated the structure, felt in control, felt had more time, did not feel like a diet (because asked to change when eating, but not what is eaten). | “I found it suited my lifestyle... I tend to be an organised person.” “Enjoyed preparing my meals early and finish up early for the day. That was the best thing.” “Other diets you need to make a choice of what you need to eat and counting everything you want to eat, but this one I just eat what I want to eat and how much. I didn’t have to do all the counting.” |
| Negative reaction: found it stressful, felt anxious about sticking to the routine. | “There was always kind of a stress I have to do it in between this time.” | |
| Monitoring and Accountability | Self-monitoring: increased self-awareness and accountability, identifying patterns and relationships (e.g., eating and blood glucose). | “I think some of that accountability of thinking about what you’re eating and having to report it all.” “The data for me is a big thing... seeing how my blood sugars will react to the foods.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parr, E.B.; Devlin, B.L.; Lim, K.H.C.; Moresi, L.N.Z.; Geils, C.; Brennan, L.; Hawley, J.A. Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study. Nutrients 2020, 12, 3228. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113228
Parr EB, Devlin BL, Lim KHC, Moresi LNZ, Geils C, Brennan L, Hawley JA. Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study. Nutrients. 2020; 12(11):3228. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113228
Chicago/Turabian StyleParr, Evelyn B., Brooke L. Devlin, Karen H. C. Lim, Laura N. Z. Moresi, Claudia Geils, Leah Brennan, and John A. Hawley. 2020. "Time-Restricted Eating as a Nutrition Strategy for Individuals with Type 2 Diabetes: A Feasibility Study" Nutrients 12, no. 11: 3228. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113228