
Iodine Status Modifies the Association between Fluoride Exposure in Pregnancy and Preschool Boys’ Intelligence

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
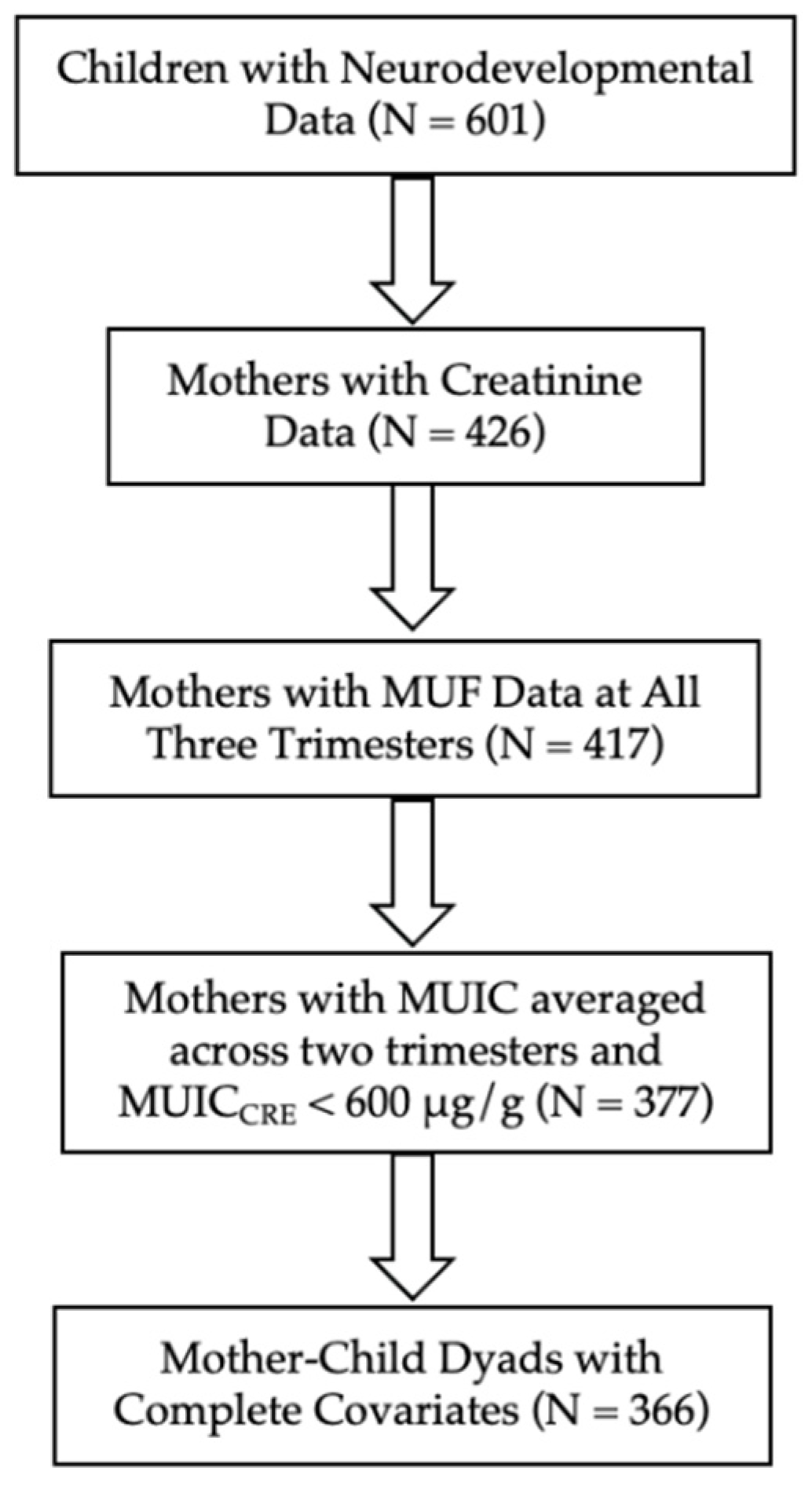
2.1. Participants
2.2. Urine Collection
2.3. Maternal Urinary Fluoride Concentration
2.4. Maternal Urinary Iodine Concentration
2.5. Correcting for Variability in Urinary Dilution
2.6. Children’s Full-Scale Intelligence Quotient
2.7. Covariates
2.8. Statistical Analyses
3. Results
Three-Way Interaction Model
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, Y.; Sun, Z.R.; Wu, L.N.; Wang, X.; Lu, W.; Liu, S.S. Effect of High-Fluoride Water on Intelligence in Children. Fluoride 2000, 33, 74–78. [Google Scholar]
- Xiang, Q.; Liang, Y.; Chen, L.; Wang, C.; Chen, B.; Chen, X.; Zhou, M. Effect of Fluoride in Drinking Water on Children’s Intelligence. Fluoride 2003, 36, 84–94. [Google Scholar]
- Zhao, L.B.; Liang, G.H.; Zhang, D.N.; Wu, X.R. Effect of a High Fluoride Water Supply on Children’s Intelligence. Fluoride 1996, 29, 190–192. [Google Scholar]
- Bashash, M.; Thomas, D.; Hu, H.; Martinez-Mier, E.A.; Sanchez, B.N.; Basu, N.; Peterson, K.E.; Ettinger, A.S.; Wright, R.; Zhang, Z.; et al. Prenatal Fluoride Exposure and Cognitive Outcomes in Children at 4 and 6–12 Years of Age in Mexico. Environ. Health Perspect. 2017, 125, 97017. [Google Scholar] [CrossRef]
- Till, C.; Green, R.; Flora, D.; Hornung, R.; Martinez-Mier, E.A.; Blazer, M.; Farmus, L.; Ayotte, P.; Muckle, G.; Lanphear, B. Fluoride Exposure from Infant Formula and Child IQ in a Canadian Birth Cohort. Environ. Int. 2020, 134, 105315. [Google Scholar] [CrossRef]
- Green, R.; Lanphear, B.; Hornung, R.; Flora, D.; Martinez-Mier, E.A.; Neufeld, R.; Ayotte, P.; Muckle, G.; Till, C. Association between Maternal Fluoride Exposure during Pregnancy and IQ Scores in Offspring in Canada. JAMA Pediatr. 2019, 173, 940–948. [Google Scholar] [CrossRef]
- Chaitanya, N.; Karunakar, P.; Allam, N.; Priya, M.; Alekhya, B.; Nauseen, S. A Systematic Analysis on Possibility of Water Fluoridation Causing Hypothyroidism. Indian J. Dent. Res. 2018, 29, 358–363. [Google Scholar] [CrossRef]
- Wang, M.; Liu, L.; Li, H.; Li, Y.; Liu, H.; Hou, C.; Zeng, Q.; Li, P.; Zhao, Q.; Dong, L.; et al. Thyroid Function, Intelligence, and Low-Moderate Fluoride Exposure among Chinese School-Age Children. Environ. Int. 2020, 134, 105229. [Google Scholar] [CrossRef]
- Khandare, A.L.; Validandi, V.; Gourineni, S.R.; Gopalan, V.; Nagalla, B. Dose-Dependent Effect of Fluoride on Clinical and Subclinical Indices of Fluorosis in School Going Children and Its Mitigation by Supply of Safe Drinking Water for 5 Years: An Indian Study. Environ. Monit. Assess. 2018, 190, 1–8. [Google Scholar] [CrossRef]
- KheradPisheh, Z.; Mirzaei, M.; Mahvi, A.H.; Mokhtari, M.; Azizi, R.; Fallahzadeh, H.; Ehrampoush, M.H. Impact of Drinking Water Fluoride on Human Thyroid Hormones: A Case-Control Study. Sci. Rep. 2018, 8, 2674. [Google Scholar] [CrossRef] [Green Version]
- Peckham, S.; Lowery, D.; Spencer, S. Are Fluoride Levels in Drinking Water Associated with Hypothyroidism Prevalence in England? A Large Observational Study of GP Practice Data and Fluoride Levels in Drinking Water. J. Epidemiol. Community Health 2015, 69, 619–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Research Council. Fluoride in Drinking Water; A Scientific Review of EPA’s Standards; National Academies Press: Washington, DC, USA, 2006; ISBN 9780309101288. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc: A Report of the Panel on Micronutrients… [et al.], Standing Committee on the Scientific Eva; National Academies Press: Cambridge, MA, USA, 2001. [Google Scholar]
- Murcia, M.; Espada, M.; Julvez, J.; Llop, S.; Lopez-Espinosa, M.J.; Vioque, J.; Basterrechea, M.; Rianõ, I.; González, L.; Alvarez-Pedrerol, M.; et al. Iodine Intake from Supplements and Diet during Pregnancy and Child Cognitive and Motor Development: The INMA Mother and Child Cohort Study. J. Epidemiol. Community Health 2018, 72, 216–222. [Google Scholar] [CrossRef] [PubMed]
- de Escobar, G.M.; Obregón, M.J.; Escobar del Rey, F. Maternal Thyroid Hormones Early in Prenancy and Fetal Brain Development. Best Pract. Res. Clin. Endocrinol. Metab. 2004, 18, 225–248. [Google Scholar] [CrossRef]
- Glinoer, D. The Regulation of Thyroid Function during Normal Pregnancy: Importance of the Iodine Nutrition Status. Best Pract. Res. Clin. Endocrinol. Metab. 2004, 18, 133–152. [Google Scholar] [CrossRef]
- Katz, P.M.; Leung, A.M.; Braverman, L.E.; Pearce, E.N.; Tomlinson, G.; He, X.; Vertes, J.; Okun, N.; Walfish, P.G.; Feig, D.S. Iodine Nutrition during Pregnancy in Toronto, Canada. Endocr. Pract. 2013, 19, 206–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Escobar, G.M.; Obregón, M.J.; Del Rey, F.E. Iodine Deficiency and Brain Development in the First Half of Pregnancy. Public Health Nutr. 2007, 10, 1554–1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.B. Iodine Deficiency in Pregnancy and the Effects of Maternal Iodine Supplementation on the Offspring: A Review. Am. J. Clin. Nutr. 2009, 89, 668–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melse-Boonstra, A.; Jaiswal, N. Iodine Deficiency in Pregnancy, infancy, and childhood and its consequences for brain development. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Bath, S.C. The Effect of Iodine Deficiency during Pregnancy on Child Development. Proc. Nutr. Soc. 2019, 78, 150–160. [Google Scholar] [CrossRef]
- Pearce, E.N. Effects of Iodine Deficiency in Pregnancy. J. Trace Elem. Med. Biol. 2012, 26, 131–133. [Google Scholar] [CrossRef]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of Inadequate Iodine Status in UK Pregnant Women on Cognitive Outcomes in Their Children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Levie, D.; Korevaar, T.I.M.; Bath, S.C.; Murcia, M.; Dineva, M.; Llop, S.; Espada, M.; Van Herwaarden, A.E.; De Rijke, Y.B.; Ibarluzea, J.M.; et al. Association of Maternal Iodine Status with Child IQ: A Meta-Analysis of Individual Participant Data. J. Clin. Endocrinol. Metab. 2019, 104, 5957–5967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghassabian, A.; Steenweg-de Graaff, J.; Peeters, R.P.; Ross, H.A.; Jaddoe, V.W.; Hofman, A.; Verhulst, F.C.; White, T.; Tiemeier, H. Maternal Urinary Iodine Concentration in Pregnancy and Children’s Cognition: Results from a Population-Based Birth Cohort in an Iodine-Sufficient Area. BMJ Open 2014, 4, e005520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebagliato, M.; Murcia, M.; Álvarez-Pedrerol, M.; Espada, M.; Fernández-Somoano, A.; Lertxundi, N.; Navarrete-Muñoz, E.M.; Forns, J.; Aranbarri, A.; Llop, S.; et al. Iodine Supplementation during Pregnancy and Infant Neuropsychological Development. Am. J. Epidemiol. 2013, 177, 944–953. [Google Scholar] [CrossRef] [Green Version]
- Ren, D.; Li, K.; Liu, D. A Study of the Intellectual Ability of 8–14 Year-Old Children in High Fluoride, Low Iodine Areas. Fluoride 2008, 41, 319–320. [Google Scholar]
- Fa-Fu, L.; Aihaiti, H.X.Z.; Jin, U.; Ji-Yong, J.; Maimaiti, A. The Relationship of a Low-Iodine and High- Fluoride Environment to Subclinical Cretinism in Xinjiang. Iodine Defic. Disord. Newsl. 1991, 7, 24–25. [Google Scholar]
- Wang, J.; Ge, Y.; Ning, H.; Wang, S. Effects of High Fluoride and Low Iodine on Biochemical Indexes of the Brain and Learning-Memory of Offspring Rats. Fluoride 2004, 37, 201–208. [Google Scholar]
- Hong, J.H.; Ge, Y.M.; Ning, H.M. Effects of High Fluoride and Low Iodine on Learning-Memory and TchE of Brain in Offspring Rats. China Prev. Med. 2005, 6, 489–491. [Google Scholar]
- Mioto, V.C.B.; de Castro Nassif Gomes Monteiro, A.C.; De Camargo, R.Y.A.; Borel, A.R.; Catarino, R.M.; Kobayashi, S.; Chammas, M.C.; Marui, S. High Prevalence of Iodine Deficiency in Pregnant Women Living in Adequate Iodine Area. Endocr. Connect. 2018, 7, 762–767. [Google Scholar] [CrossRef]
- Perrine, C.G.; Herrick, K.A.; Gupta, P.M.; Caldwell, K.L.; Activity, P.; Surveys, N.E. Iodine Status of Pregnant Women and Women of Reproductive Age in the United States. Thyroid 2019, 29, 153–154. [Google Scholar] [CrossRef]
- Green, R.; Rubenstein, J.; Popoli, R.; Capulong, R.; Till, C. Sex-Specific Neurotoxic Effects of Early-Life Exposure to Fluoride: A Review of the Epidemiologic and Animal Literature. Curr. Epidemiol. Rep. 2020, 7, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, T.E.; Fraser, W.D.; Fisher, M.; Davis, K.; Liang, C.L.; Lupien, N.; Bastien, S.; Velez, M.P.; Von Dadelszen, P.; Hemmings, D.G.; et al. Cohort Profile: The Maternal-Infant Research on Environmental Chemicals Research Platform. Paediatr. Perinat. Epidemiol. 2013, 27, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Wan, S.; Zhang, L.; Li, B.; He, Y.; Shen, H.; Liu, L. A Meta-Analysis of the Effect of Iodine Excess on the Intellectual Development of Children in Areas with High Iodine Levels in Their Drinking Water. Biol. Trace Elem. Res. 2022, 200, 1580–1590. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Worldwide Iodine Status. In WHO Global Database on Iodine Deficiency; Department of Nutrition for Health and Development World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Luo, J.; Li, C.; Zhang, X.; Shan, Z.; Teng, W. Reference Intervals of the Ratio of Urine Iodine to Creatinine in Pregnant Women in an Iodine-Replete Area of China. Biol. Trace Elem. Res. 2020, 199, 62–69. [Google Scholar] [CrossRef]
- Till, C.; Green, R.; Grundy, J.G.; Hornung, R.; Neufeld, R.; Martinez-Mier, E.A.; Ayotte, P.; Muckle, G.; Lanphear, B. Community Water Fluoridation and Urinary Fluoride Concentrations in a National Sample of Pregnant Women in Canada. Environ. Health Perspect. 2018, 126, 107001. [Google Scholar] [CrossRef]
- Martínez-Mier, E.A.; Cury, J.A.; Heilman, J.R.; Katz, B.P.; Levy, S.M.; Li, Y.; Maguire, A.; Margineda, J.; O’Mullane, D.; Phantumvanit, P.; et al. Development of Gold Standard Ion-Selective Electrode-Based Methods for Fluoride Analysis. Caries Res. 2011, 45, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.B.; Andersson, M. Assessment of Iodine Nutrition in Populations: Past, Present, and Future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef]
- Li, C.; Peng, S.; Zhang, X.; Xie, X.; Wang, D.; Mao, J.; Teng, X.; Shan, Z.; Teng, W. The Urine Iodine to Creatinine as an Optimal Index of Iodine during Pregnancy in an Iodine Adequate Area in China. J. Clin. Endocrinol. Metab. 2016, 101, 1290–1298. [Google Scholar] [CrossRef]
- Caldwell, B.M.; Bradley, R.H. Home Observation for Measurement of the Environment; University of Arkansas: Little Rock, AR, USA, 1979. [Google Scholar]
- Bauer, D.J.; Curran, P.J.; Thurstone, L.L. Probing Interactions in Fixed and Multilevel Regression: Inferential and Graphical Techniques. Multivariate Behav. Res. 2005, 40, 373–400. [Google Scholar] [CrossRef]
- Van Mil, N.H.; Tiemeier, H.; Bongers-Schokking, J.J.; Ghassabian, A.; Hofman, A.; Hooijkaas, H.; Jaddoe, V.W.V.; de Muinck Keizer-Schrama, S.M.; Steegers, E.A.P.; Visser, T.J.; et al. Low Urinary Iodine Excretion during Early Pregnancy Is Associated with Alterations in Executive Functioning in Children. J. Nutr. 2012, 142, 2167–2174. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Zhou, G.; Gong, B.; Ma, J.; An, N.; Gao, M.; Yang, M.; Ma, Q.; Huang, H.; Zuo, Q.; et al. Iodine Modifies the Susceptibility of Thyroid to Fluoride Exposure in School-Age Children: A Cross-Sectional Study in Yellow River Basin, Henan, China. Biol. Trace Elem. Res. 2021, 199, 3658–3666. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Niu, R.; Zhang, J.; Wang, J. Proteomic Analysis of Brain Proteins of Rats Exposed to High Fluoride and Low Iodine. Arch. Toxicol. 2011, 85, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Ning, H.; Wang, S.; Wang, J. Effects of High Fluoride and Low Iodine on Brain Histopathology in Offspring Rats. Fluoride 2005, 38, 127–132. [Google Scholar]
- Ge, Y.; Ning, H.; Feng, C.; Wang, H.; Yan, X.; Wang, S.; Wang, J. Apoptosis in Brain Cells of Offspring Rats Exposed to High Fluoride and Low Iodine. Fluoride 2006, 39, 173–178. [Google Scholar]
- Malin, A.J.; Riddell, J.; McCague, H.; Till, C. Fluoride Exposure and Thyroid Function among Adults Living in Canada: Effect Modification by Iodine Status. Environ. Int. 2018, 121, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Waugh, D.T. Fluoride exposure induces inhibition of sodium/iodide symporter (NIS) contributing to impaired iodine absorption and iodine deficiency: Molecular mechanisms of inhibition and implications for public health. Int. J. Environ. Res. Public Health 2019, 16, 1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, N.; Verma, K.G.; Verma, P.; Sidhu, G.K.; Sachdeva, S. A comparative study of fluoride ingestion levels, serum thyroid hormone & TSH level derangements, dental fluorosis status among school children from endemic and non-endemic fluorosis areas. Springerplus 2014, 3, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, W.; Zhu, H.; Yu, Z.; Aoki, K.; Misumi, J.; Zhang, X. Long-Term Effects of Various Iodine and Fluorine Doses on the Thyroid and Fluorosis in Mice. Endocr. Regul. 1998, 32, 63–70. [Google Scholar]
- Guan, Z.Z.; Zhuang, Z.-J.; Yang, P.-S.; Pan, S. Synergistic Action of Iodine-Deficiency and Fluorine-Intoxication of Rat Thyroid. Chin. Med. J. 1988, 101, 679–684. [Google Scholar]
- Rovet, J.F. The Role of Thyroid Hormones for Brain Development and Cognitive Function. Endocr. Dev. 2014, 26, 26–43. [Google Scholar] [CrossRef]
- Moog, N.K.; Entringer, S.; Heim, C.; Wadhwa, P.D.; Kathmann, N.; Buss, C. Influence of Maternal Thyroid Hormones during Gestation on Fetal Brain Development. Neuroscience 2017, 342, 68–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prezioso, G.; Giannini, C.; Chiarelli, F. Effect of Thyroid Hormones on Neurons and Neurodevelopment. Horm. Res. Paediatr. 2018, 90, 73–81. [Google Scholar] [CrossRef]
- Jansen, T.A.; Korevaar, T.I.M.; Mulder, T.A.; White, T.; Muetzel, R.L.; Peeters, R.P.; Tiemeier, H. Maternal Thyroid Function during Pregnancy and Child Brain Morphology: A Time Window-Specific Analysis of a Prospective Cohort. Lancet Diabetes Endocrinol. 2019, 7, 629–637. [Google Scholar] [CrossRef]
- Miranda, A.; Sousa, N. Maternal Hormonal Milieu Influence on Fetal Brain Development. Brain Behav. 2018, 8, e00920. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B. The Effects of Iodine Deficiency in Pregnancy and Infancy. Paediatr. Perinat. Epidemiol. 2012, 26, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Green, R.; Goodman, C.V.; Farmus, L.; Lanphear, B.; Martinez-Mier, A.; Hornung, R.; Ayotte, P.; Till, C. Fluoride Exposure and Hypothyroidism in a Canadian Pregnancy Cohort. Birth Defects Res. 2021, 113, 804. [Google Scholar]
- Batista, G.; Hensch, T.K. Critical Period Regulation by Thyroid Hormones: Potential Mechanisms and Sex-Specific Aspects. Front. Mol. Neurosci. 2019, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Duarte-Guterman, P.; Navarro-Martín, L.; Trudeau, V.L. Mechanisms of Crosstalk between Endocrine Systems: Regulation of Sex Steroid Hormone Synthesis and Action by Thyroid Hormones. Gen. Comp. Endocrinol. 2014, 203, 69–85. [Google Scholar] [CrossRef]
- Baksi, S.; Pradhan, A. Thyroid Hormone: Sex-Dependent Role in Nervous System Regulation and Disease. Biol. Sex Differ. 2021, 12, 25. [Google Scholar] [CrossRef]
- Li, P.; Teng, Y.; Ru, X.; Liu, Z.; Han, Y.; Tao, F.; Huang, K. Sex-Specific Effect of Maternal Thyroid Hormone Trajectories on Preschoolers’ Behavioral Development: A Birth Cohort Study. J. Clin. Endocrinol. Metab. 2022, 107, e2037–e2046. [Google Scholar] [CrossRef]
- König, F.; Andersson, M.; Hotz, K.; Aeberli, I.; Zimmermann, M.B. Ten Repeat Collections for Urinary Iodine from Spot Samples or 24-Hour Samples Are Needed to Reliably Estimate Individual Iodine Status in Women. J. Nutr. 2011, 141, 2049–2054. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Characteristic (Mean ± SD or N (%)) | Complete Data (N = 366) | Incomplete Data (N = 211) | p |
|---|---|---|---|
| Mothers | |||
| Maternal Age (years) | 32.50 ± 4.51 | 32.55 ± 4.62 | 0.899 |
| Married or Common Law | 353 (96.54) | 205 (97.16) | 0.646 |
| White | 334 (91.26) | 181 (85.78) | 0.041 |
| Bachelor’s Degree or Higher | 243 (66.39) | 142 (67.30) | 0.824 |
| Taking a prenatal multivitamin | 319 (87.40) | 175 (82.94) | 0.140 |
| HOME Score | 47.23 ± 4.44 | 47.40 ± 4.10 | 0.649 |
| Children | |||
| Male | 186 (50.82) | 98 (46.44) | 0.311 |
| Age at Testing (years) | 3.44 ± 0.32 | 3.40 ± 0.31 | 0.144 |
| Urinary Measurement | All | Boys | Girls | ||||
|---|---|---|---|---|---|---|---|
| n | Median (IQR) | n | Median (IQR) | n | Median (IQR) | p 1 | |
| MUFCRE (mg/g) | 366 | 0.61 (0.49) | 186 | 0.63 (0.52) | 180 | 0.61 (0.48) | 0.538 |
| MUICCRE (μg/g) | 366 | 294 (181) | 186 | 309 (181) | 180 | 287 (203) | 0.059 |
| Low | 86 | 148 (47) | 31 | 131 (73) | 55 | 152 (37) | 0.083 |
| Adequate | 280 | 341 (165) | 155 | 348 (187) | 125 | 336 (146) | 0.893 |
| Outcome | n | Mean ± SD | n | Mean ± SD | n | Mean ± SD | p 1 |
| FSIQ | 366 | 107.46 ± 13.75 | 186 | 105.25 ± 14.90 | 180 | 109.75 ± 12.09 | 0.002 |
| Variable | B | SE(B) | p |
|---|---|---|---|
| MUFCRE (mg/g) | −5.89 | 1.85 | 0.002 |
| MUICCRE (μg/g) | −0.03 | 0.01 | 0.023 |
| Sex | −3.09 | 2.17 | 0.155 |
| MUFCRE × MUICCRE | 0.02 | 0.01 | 0.042 |
| MUFCRE × Sex | 8.51 | 2.40 | <0.001 |
| MUICCRE × Sex | 0.03 | 0.02 | 0.042 |
| MUFCRE × MUICCRE × Sex | −0.04 | 0.02 | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodman, C.V.; Hall, M.; Green, R.; Chevrier, J.; Ayotte, P.; Martinez-Mier, E.A.; McGuckin, T.; Krzeczkowski, J.; Flora, D.; Hornung, R.; et al. Iodine Status Modifies the Association between Fluoride Exposure in Pregnancy and Preschool Boys’ Intelligence. Nutrients 2022, 14, 2920. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14142920
Goodman CV, Hall M, Green R, Chevrier J, Ayotte P, Martinez-Mier EA, McGuckin T, Krzeczkowski J, Flora D, Hornung R, et al. Iodine Status Modifies the Association between Fluoride Exposure in Pregnancy and Preschool Boys’ Intelligence. Nutrients. 2022; 14(14):2920. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14142920
Chicago/Turabian StyleGoodman, Carly V., Meaghan Hall, Rivka Green, Jonathan Chevrier, Pierre Ayotte, Esperanza Angeles Martinez-Mier, Taylor McGuckin, John Krzeczkowski, David Flora, Richard Hornung, and et al. 2022. "Iodine Status Modifies the Association between Fluoride Exposure in Pregnancy and Preschool Boys’ Intelligence" Nutrients 14, no. 14: 2920. https://0-doi-org.brum.beds.ac.uk/10.3390/nu14142920