
The Assessment of Big Data Adoption Readiness with a Technology–Organization–Environment Framework: A Perspective towards Healthcare Employees

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Background and Related Works
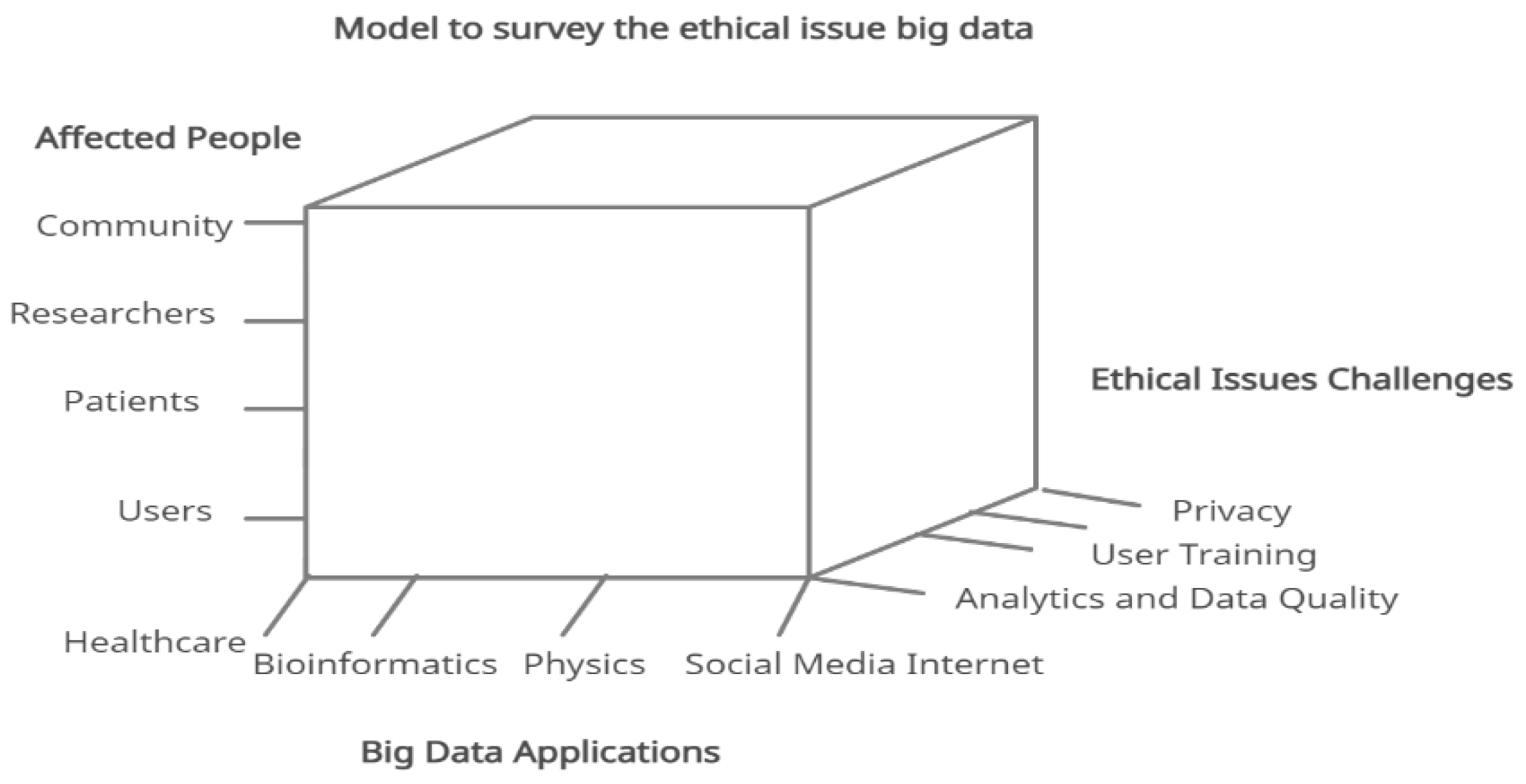
2.1. Healthcare, Big Data, and Challenges
2.2. Theoretical Background
2.2.1. Technology–Organization–Environment (TOE)
2.2.2. Technology Readiness Index
2.2.3. Organizational Factors in Big Data Readiness
2.2.4. Environment Factors in Big Data Readiness
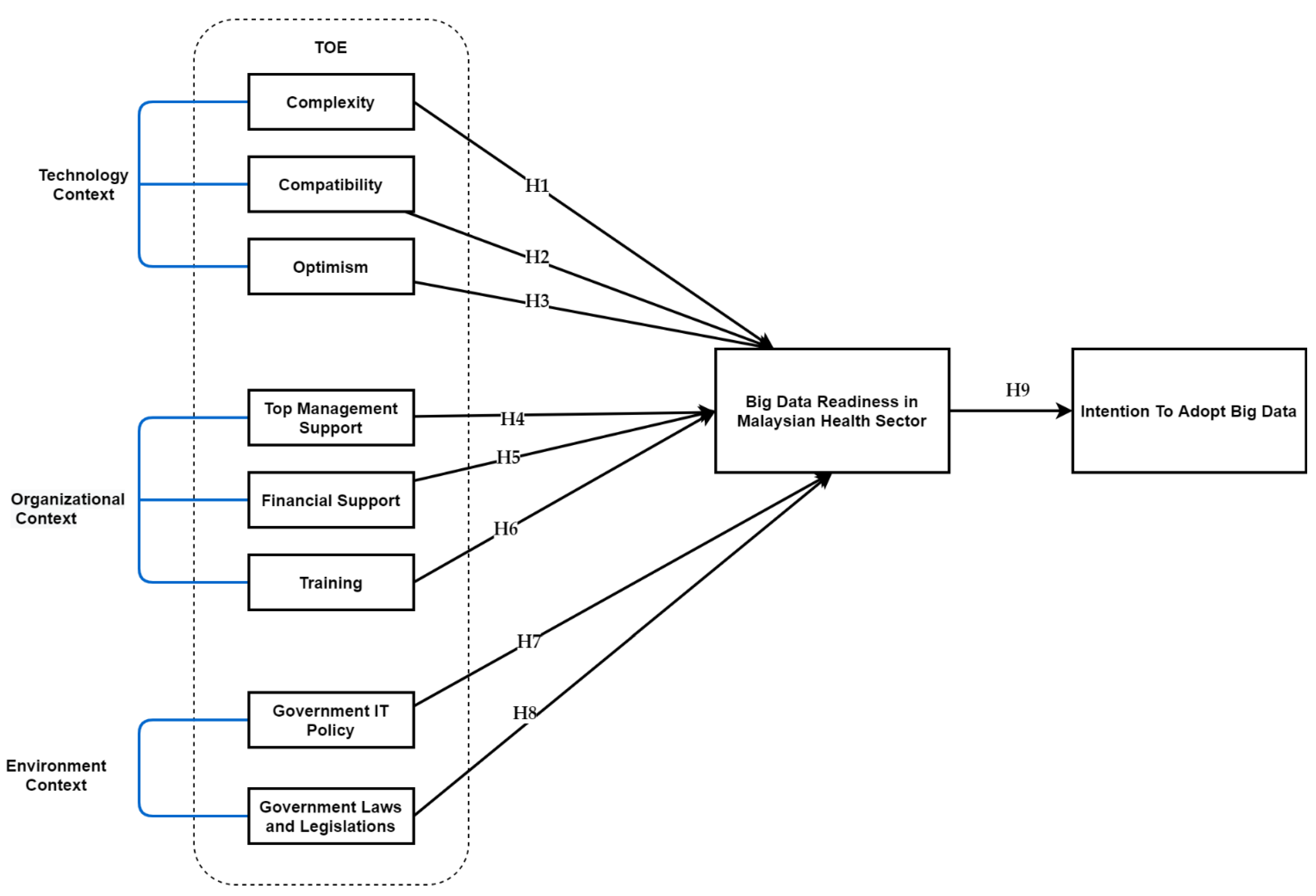
3. Theoretical Framework and Hypothesis Development
3.1. Technology Context
3.2. Organizational Context
3.3. Environmental Context
3.4. BD Readiness in Healthcare Sectors
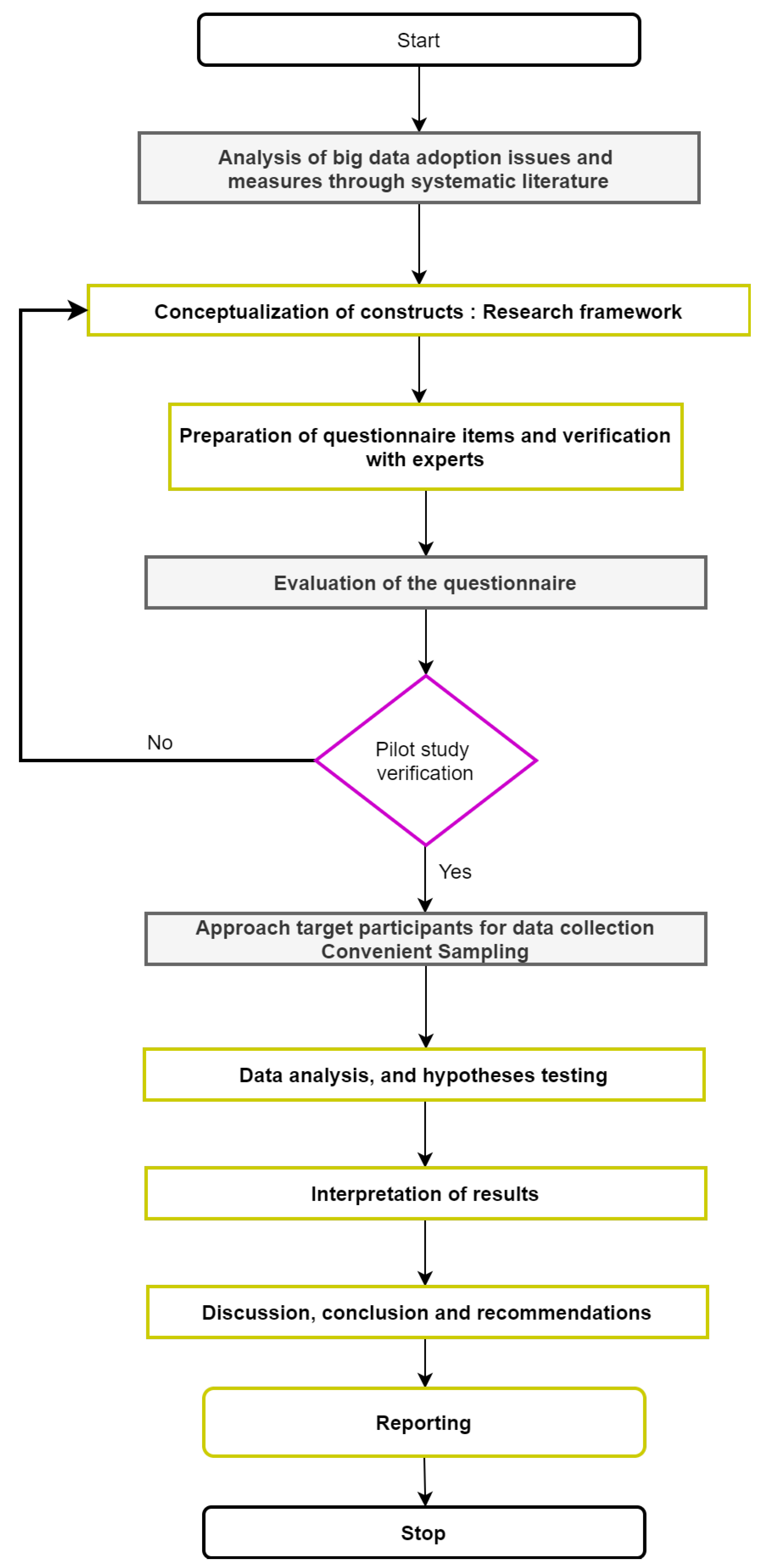
4. Methodology
4.1. Instrument Design
4.2. Pre-Testing
4.3. Sampling and Data Collection Procedure
- Participants must be health professionals.
- Participants should be a frequent user of technology.
- Participants must have some awareness about emerging technologies used in healthcare.
4.4. Measurement Scale
5. Results
5.1. Measurement Framework
5.1.1. Convergent Validity
5.1.2. Discriminant Validity
5.2. Structural Model Assessment
6. Discussion
7. Conclusions
7.1. Theoretical Implications
7.2. Practical Implications
7.3. Limitations and Future Research
7.4. Closing Remarks
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Constructs | Items | References |
|---|---|---|
| Complexity (CX) | [69,100,130,151,163,181,182,183] | |
| BD allows me to manage business operations in an efficient way. | CX1 | |
| The use of BD is frustrating. | CX2 | |
| The skills needed to improve and use the new technologies are easy for me. | CX3 | |
| The use of BD requires a lot of mental effort. | CX4 | |
| Compatibility (CT) | [69,71,91,100,130,181,182,183] | |
| The use of BD is compatible with my healthcare corporate culture and value system. | CT1 | |
| The use of BD will be compatible with existing hardware and software. | CT2 | |
| BD is easy to use and manage. | CT3 | |
| BD is compatible with existing emerging technologies. | CT4 | |
| Optimism (OP) | [139,179,184,185,186] | |
| New technologies contribute to a better quality of life. | OP1 | |
| Technology gives me more freedom of mobility. | OP2 | |
| Technology gives people more control over their daily lives | OP3 | |
| Technology makes me more productive in my personal life. | OP4 | |
| Technology makes me more efficient in my occupation | OP5 | |
| Top Management support (TMS) | [69,100,130,187,188,189,190] | |
| Top management supports plans to adopt the big data. | TMS1 | |
| Top management will support the implementation of BD adoption. | TMS2 | |
| Top management support is important to provide the resources for the company to adopt big data. | TMS3 | |
| The healthcare management is willing to take risks (financial and organizational) involved in the adoption of big data. | TMS4 | |
| The firm size compatible with the adoption of big data. | TMS5 | |
| Financial support (FS) | [191,192,193] | |
| Financial support is important for purchasing new technology equipment. | FS1 | |
| Financial support for the BD technology will strengthen the current system infrastructure in healthcare. | FS1 | |
| Financial support will help to better secure the patient’s data. | FS1 | |
| My company has the financial resources to purchase the hardware and software required for technologies. | FS4 | |
| Training (TR) | [194] | |
| Training on the BD usage is meeting my requirements. | TR1 | |
| Training on BD usage ensures that employees have received the appropriate training. | TR2 | |
| Training on BD usage is adequate for all involved staff. | TR3 | |
| All users have been trained in basic technology skills in the healthcare system. | TR4 | |
| Government IT policies (GITP) | [71,100,130,151,190,195,196] | |
| Government IT policy can attract more foreign investors to invest in sustainable businesses. | GITP1 | |
| Government IT policy can encourage sustainable technology usage. | GITP2 | |
| Government IT policy can improve sustainable technology efficiency. | GITP3 | |
| Government IT policy can educate sustainable technology in Malaysian on the benefits of sustainable technology. | GITP4 | |
| There is a lack of security rules, IT policies, and privacy laws. | GITP5 | |
| Government lows and legislations (GLAL) | [197,198,199] | |
| The laws and regulation that exist nowadays are sufficient to protect the use of big data, | GLAL1 | |
| The government drives the use of the BD through incentive programs. | GLAL2 | |
| The company requires maintaining the regulatory environment in the use of big data. | GLAL3 | |
| The laws and regulations of the government support BD initiatives and implementation. | GLAL4 | |
| Government laws and regulations can provide a better process for adopting technologies. | GLAL5 | |
| BD Readiness (BDR) in Healthcare Sector | [69,71,199,200,201] | |
| The healthcare management understands how they can be used in the healthcare sector. | BDR1 | |
| The healthcare IT infrastructure is good (internet service/devices) and can be used for big data. | BDR2 | |
| The healthcare management already promoted the usage of the BD to the staff very well. | BDR3 | |
| The healthcare staff have the right skills to work with big data. | BDR4 | |
| The healthcare IT department and the healthcare management have the right skills to lead the healthcare transformation, and they give very good support to help the staff. | BDR5 | |
| Intention to adoption BD (ITABD) | [71,197,199,200,201] | |
| BD adoption is effective to enhance the behavioral intentions to use the BD analytics system in healthcare. | ITABD 1 | |
| BD technology adoption will increase the performance and effectiveness of healthcare. | ITABD 2 | |
| I would use BD technology adoption to gather health data. | ITABD 3 | |
| I would use the services provided by use BD technology adoption. | ITABD 4 | |
| I would not hesitate to provide information for use BD technology adoption | ITABD 5 |
References
- Bhavnani, S.P.; Parakh, K.; Atreja, A.; Druz, R.; Graham, G.N.; Hayek, S.S.; Krumholz, H.M.; Maddox, T.M.; Majmudar, M.D.; Rumsfeld, J.S. 2017 Roadmap for Innovation—ACC Health Policy Statement on Healthcare Transformation in the Era of Digital Health, Big Data, and Precision Health: A Report of the American College of Cardiology Task Force on Health Policy Statements and Systems of Care. J. Am. Coll. Cardiol. 2017, 70, 2696–2718. [Google Scholar] [CrossRef]
- Fati, S.M.; Muneer, A.; Mungur, D.; Badawi, A. Integrated Health Monitoring System Using GSM and IoT. In Proceedings of the 2018 International Conference on Smart Computing and Electronic Enterprise (ICSCEE), Kuala Lumpur, Malaysia, 11–12 July 2018; pp. 1–7. [Google Scholar]
- Muneer, A.; Fati, S.M.; Fuddah, S. Smart health monitoring system using IoT based smart fitness mirror. Telkomnika 2020, 18, 317–331. [Google Scholar] [CrossRef]
- Muneer, A.; Fati, S.M. A comparative analysis of machine learning techniques for cyberbullying detection on twitter. Future Internet 2020, 12, 187. [Google Scholar] [CrossRef]
- Ghaleb, E.A.; Dominic, P.; Mohamed, I.; Almaghthawi, A.; AL-Ashmori, A. Factors Affecting the Quality on the Health Information System users among the Yemeni Hospitals. Solid State Technol. 2020, 63, 9202–9209. [Google Scholar]
- Naseer, S.; Ali, R.F.; Muneer, A.; Fati, S.M. IAmideV-deep: Valine amidation site prediction in proteins using deep learning and pseudo amino acid compositions. Symmetry 2021, 13, 560. [Google Scholar] [CrossRef]
- Naseer, S.; Ali, R.F.; Fati, S.M.; Muneer, A. iNitroY-Deep: Computational Identification of Nitrotyrosine Sites to Supplement Carcinogenesis Studies Using Deep Learning. IEEE Access 2021, 9, 73624–73640. [Google Scholar] [CrossRef]
- Kumari, A.; Tanwar, S.; Tyagi, S.; Kumar, N. Verification and validation techniques for streaming big data analytics in internet of things environment. IET Netw. 2019, 8, 155–163. [Google Scholar] [CrossRef]
- Rajabion, L.; Shaltooki, A.A.; Taghikhah, M.; Ghasemi, A.; Badfar, A. Healthcare big data processing mechanisms: The role of cloud computing. Int. J. Inf. Manag. 2019, 49, 271–289. [Google Scholar] [CrossRef]
- Dong, K.; Ali, R.F.; Dominic, P.; Ali, S.E.A. The Effect of Organizational Information Security Climate on Information Security Policy Compliance: The Mediating Effect of Social Bonding towards Healthcare Nurses. Sustainability 2021, 13, 2800. [Google Scholar] [CrossRef]
- Ali, R.F.; Dominic, P.; Ali, S.E.A.; Naseer, S. Information Security Behavior of IT Professionals (Role of Polices and Compliance). Solid State Technol. 2020, 63, 21601–21608. [Google Scholar]
- Verhoef, P.C.; Broekhuizen, T.; Bart, Y.; Bhattacharya, A.; Dong, J.Q.; Fabian, N.; Haenlein, M. Digital transformation: A multidisciplinary reflection and research agenda. J. Bus. Res. 2021, 122, 889–901. [Google Scholar] [CrossRef]
- Ali, R.F.; Dominic, P.; Ali, S.E.A.; Rehman, M.; Sohail, A. Information security behavior and information security policy compliance: A systematic literature review for identifying the transformation process from noncompliance to compliance. Appl. Sci. 2021, 11, 3383. [Google Scholar] [CrossRef]
- Muneer, A.; Fati, S.M. Automated Health Monitoring System Using Advanced Technology. J. Inf. Technol. Res. JITR 2019, 12, 104–132. [Google Scholar] [CrossRef] [Green Version]
- Stratopoulos, T. Duration of Competitive Advantage due to Emerging Technology Adoption. In Proceedings of the UKAIS 2016, UK Academy for Information Systems 21st Annual Conference 2016, St Catherines College, Oxford, UK, 12–13 April 2016; p. 41. [Google Scholar]
- Koo, J.; Kang, G.; Kim, Y.-G. Security and Privacy in Big Data Life Cycle: A Survey and Open Challenges. Sustainability 2020, 12, 10571. [Google Scholar] [CrossRef]
- Iljashenko, O.; Bagaeva, I.; Levina, A. Strategy for establishment of personnel KPI at health care organization digital transformation. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Saint-Petersburg, Russian, 21–22 November 2018; p. 012029. [Google Scholar]
- Gahleb, E.; Mohamed, I. Health information system success framework based on user requirements perspective. J. Theor. Appl. Inf. Technol. 2018, 96, 3740–3746. [Google Scholar]
- Vickers, N.J. Animal communication: When I’m calling you, will you answer too? Curr. Biol. 2017, 27, R713–R715. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.; Winter, S.R. A practical guide for using electronic surveys in aviation research: Best practices explained. Int. J. Aviat. Aeronaut. Aerosp. 2020, 7, 1. [Google Scholar] [CrossRef]
- Gui, Z.; Yu, M.; Yang, C.; Jiang, Y.; Chen, S.; Xia, J.; Huang, Q.; Liu, K.; Li, Z.; Hassan, M.A. Developing subdomain allocation algorithms based on spatial and communicational constraints to accelerate dust storm simulation. PLoS ONE 2016, 11, e0152250. [Google Scholar] [CrossRef]
- McLeod, C.C.; Klabunde, C.N.; Willis, G.B.; Stark, D. Health care provider surveys in the United States, 2000–2010: A review. Eval. Health Prof. 2013, 36, 106–126. [Google Scholar] [CrossRef]
- Appari, A.; Johnson, M.E. Information security and privacy in healthcare: Current state of research. Int. J. Internet Enterp. Manag. 2010, 6, 279–314. [Google Scholar] [CrossRef]
- Fati, S.M.; Muneer, A.; Akbar, N.A.; Taib, S.M. A Continuous Cuffless Blood Pressure Estimation Using Tree-Based Pipeline Optimization Tool. Symmetry 2021, 13, 686. [Google Scholar] [CrossRef]
- Kessler, S.R.; Pindek, S.; Kleinman, G.; Andel, S.A.; Spector, P.E. Information security climate and the assessment of information security risk among healthcare employees. Health Inf. J. 2020, 26, 461–473. [Google Scholar] [CrossRef]
- Laurenza, E.; Quintano, M.; Schiavone, F.; Vrontis, D. The effect of digital technologies adoption in healthcare industry: A case based analysis. Busi. Process Manag. J. 2018, 5, 1124–1144. [Google Scholar] [CrossRef]
- Thomas, S.; Beh, L.; Nordin, R.B. Health care delivery in Malaysia: Changes, challenges and champions. J. Public Health Afr. 2011, 2, e23. [Google Scholar] [CrossRef]
- Argaw, S.T.; Troncoso-Pastoriza, J.R.; Lacey, D.; Florin, M.-V.; Calcavecchia, F.; Anderson, D.; Burleson, W.; Vogel, J.-M.; O’Leary, C.; Eshaya-Chauvin, B. Cybersecurity of Hospitals: Discussing the challenges and working towards mitigating the risks. BMC Med. Inf. Decis. Mak. 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, K.; Tang, Z.; Bilal, K.; Yu, S.; Weng, C.; Li, K. A parallel random forest algorithm for big data in a spark cloud computing environment. IEEE Trans. Parallel Distrib. Syst. 2016, 28, 919–933. [Google Scholar] [CrossRef] [Green Version]
- Jeremiah, P.; Samy, G.N.; Ponkoodalingam, K.; Shanmugam, B.; Maarop, N. Unravelling the Ubiquitous Information Security Compliance Conundrum Among Practitioners in Private Healthcare Organisations Within Malaysia. Psychol. Educ. J. 2020, 57, 3585–3600. [Google Scholar]
- Ross, J.; Stevenson, F.; Lau, R.; Murray, E. Factors that influence the implementation of e-health: A systematic review of systematic reviews (an update). Implement. Sci. 2016, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Jahankhani, H.; Kendzierskyj, S.; Jamal, A.; Epiphaniou, G.; Al-Khateeb, H. Blockchain and Clinical Trial: Securing Patient Data; Springer: Berlin, Germany, 2019. [Google Scholar]
- Gu, D.; Li, J.; Li, X.; Liang, C. Visualizing the knowledge structure and evolution of big data research in healthcare informatics. Int. J. Med. Inf. 2017, 98, 22–32. [Google Scholar] [CrossRef]
- Ristevski, B.; Chen, M. Big data analytics in medicine and healthcare. J. Integr. Bioinform. 2018, 15. [Google Scholar] [CrossRef]
- Ratnam, K.A.; Dominic, P. The factors associating the adoption of cloud computing: An enhancement of the healthcare ecosystem in Malaysia. Int. J. Bus. Inf. Syst. 2014, 16, 462–479. [Google Scholar] [CrossRef]
- Chen, Y.; Ding, S.; Xu, Z.; Zheng, H.; Yang, S. Blockchain-based medical records secure storage and medical service framework. J. Med. Syst. 2019, 43, 1–9. [Google Scholar] [CrossRef]
- Qian, T.; Zhu, S.; Hoshida, Y. Use of big data in drug development for precision medicine: An update. Expert Rev. Precis. Med. Drug Dev. 2019, 4, 189–200. [Google Scholar] [CrossRef]
- Alshagathrh, F.; Khan, S.A.; Alothmany, N.; Al-Rawashdeh, N.; Househ, M. Building a cloud-based data sharing model for the Saudi national registry for implantable medical devices: Results of a readiness assessment. Int. J. Med. Inf. 2018, 118, 113–119. [Google Scholar] [CrossRef]
- Wiener, M.; Saunders, C.; Marabelli, M. Big-data business models: A critical literature review and multiperspective research framework. J. Inf. Technol. 2020, 35, 66–91. [Google Scholar] [CrossRef]
- Antoniou, P.E. Implementing digital learning for health. In Digital Innovations in Healthcare Education and Training; Elsevier: Amsterdam, The Netherlands, 2021; pp. 103–125. [Google Scholar]
- Benzmann, S. How well does the European Digital Single Market Strategy and the Industry 4.0 Framework afford Digitalization Transformation? A Case Study of SAP SE. Master’s Thesis, Utrecht University School of Governance (USG), Utrecht, The Netherlands, 2021. [Google Scholar]
- Meskó, B.; Drobni, Z.; Bényei, É.; Gergely, B.; Győrffy, Z. Digital health is a cultural transformation of traditional healthcare. Mhealth 2017, 3, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.K.; Mann, K.S. Sharing of medical information on cloud platform-a review. IOSR J. Comput. Eng. 2014, 16, 8–11. [Google Scholar] [CrossRef]
- Bahl, S.; Singh, R.P.; Javaid, M.; Khan, I.H.; Vaishya, R.; Suman, R. Telemedicine technologies for confronting COVID-19 pandemic: A review. J. Ind. Integr. Manag. 2020, 5. [Google Scholar] [CrossRef]
- Mehta, N.; Pandit, A. Concurrence of big data analytics and healthcare: A systematic review. Int. J. Med. Inf. 2018, 114, 57–65. [Google Scholar] [CrossRef]
- Shahzad, K.; Nawab, R.M.A.; Abid, A.; Sharif, K.; Ali, F.; Aslam, F.; Mazhar, A. A Process Model Collection and Gold Standard Correspondences for Process Model Matching. IEEE Access 2019, 7, 30708–30723. [Google Scholar] [CrossRef]
- Weill, P.; Woerner, S.L. Is your company ready for a digital future? MIT Sloan Manag. Rev. 2018, 59, 21–25. [Google Scholar]
- Belle, A.; Thiagarajan, R.; Soroushmehr, S.; Navidi, F.; Beard, D.A.; Najarian, K. Big data analytics in healthcare. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, B.K. Big data for secure healthcare system: A conceptual design. Complex Intell. Syst. 2017, 3, 133–151. [Google Scholar] [CrossRef] [Green Version]
- Devadass, L.; Sekaran, S.S.; Thinakaran, R. Management. Cloud computing in healthcare. Int. J. Stud. Res. Technol. Manag. 2017, 5, 25–31. [Google Scholar]
- Guo, U.; Chen, L.; Mehta, P.H.J.H.I.M.J. Electronic health record innovations: Helping physicians–One less click at a time. Health Inf. Manag. J. 2017, 46, 140–144. [Google Scholar] [CrossRef]
- Agarwal, R.; Gao, G.; DesRoches, C.; Jha, A.K. Research commentary—The digital transformation of healthcare: Current status and the road ahead. Inf. Syst. Res. 2010, 21, 796–809. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, C.; Staib, A.J.A.H.R. Digital disruption ‘syndromes’ in a hospital: Important considerations for the quality and safety of patient care during rapid digital transformation. Aust. Health Rev. 2018, 42, 294–298. [Google Scholar] [CrossRef]
- Rasmi, M.; Alazzam, M.B.; Alsmadi, M.K.; Almarashdeh, I.A.; Alkhasawneh, R.A.; Alsmadi, S. Healthcare professionals’ acceptance Electronic Health Records system: Critical literature review (Jordan case study). Int. J. Healthc. Manag. 2018. [Google Scholar] [CrossRef]
- Choi, S.L.; Goh, C.F.; Adam, M.B.H.; Tan, O.K. Transformational leadership, empowerment, and job satisfaction: The mediating role of employee empowerment. Hum. Resour. Health 2016, 14, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Christodoulakis, A.; Karanikas, H.; Billiris, A.; Thireos, E.; Pelekis, N. “Big data” in health care. Arch. Hell. Med. Arheia Ellenikes Iatr. 2016, 33, 490–496. [Google Scholar]
- Iqbal, M.H.; Soomro, T.R. Big data analysis: Apache storm perspective. Int. J. Comput. Trends Technol. 2015, 19, 9–14. [Google Scholar] [CrossRef]
- Chen, J.; Li, K.; Tang, Z.; Bilal, K.; Li, K. A parallel patient treatment time prediction algorithm and its applications in hospital queuing-recommendation in a big data environment. IEEE Access 2016, 4, 1767–1783. [Google Scholar] [CrossRef]
- Zaharia, M.; Chowdhury, M.; Das, T.; Dave, A.; Ma, J.; Mccauley, M.; Franklin, M.; Shenker, S.; Stoica, I. Fast and interactive analytics over Hadoop data with Spark. Usenix Login 2012, 37, 45–51. [Google Scholar]
- Zaharia, M.; Chowdhury, M.; Das, T.; Dave, A.; Ma, J.; McCauly, M.; Franklin, M.J.; Shenker, S.; Stoica, I. Resilient distributed datasets: A fault-tolerant abstraction for in-memory cluster computing. In Proceedings of the 9th {USENIX} Symposium on Networked Systems Design and Implementation ({NSDI} 12), San Joe, CA, USA, 25–27 April 2012; pp. 15–28. [Google Scholar]
- Fatt, Q.K.; Ramadas, A. The usefulness and challenges of big data in healthcare. J. Healthc. Commun 2018, 3, 21. [Google Scholar] [CrossRef]
- Marr, B. How big data is changing healthcare. Forbes/Tech. 2015. Available online: https://www.forbes.com/sites/bernardmarr/2015/04/21/how-big-data-is-changing-healthcare/?sh=54ce3a052873. (accessed on 2 May 2021).
- Piai, S.; Claps, M. Bigger data for better healthcare. IDC Health Insights 2013, 8, 1–24. [Google Scholar]
- Ghaleb, E.A.; Dominic, P.D.; Sarlan, A. Impact of emerging technology innovations on healthcare transformation in developing countries. In Proceedings of the 2020 Second International Sustainability and Resilience Conference: Technology and Innovation in Building Designs (51154), Sakhir, Bahrain, 11 November 2021; pp. 1–5. [Google Scholar]
- Pustovit, S.V.; Williams, E.D. Philosophical aspects of dual use technologies. Sci. Eng. Ethics 2010, 16, 17–31. [Google Scholar] [CrossRef]
- Stylianou, A.; Talias, M.A. Big data in healthcare: A discussion on the big challenges. Health Technol. 2017, 7, 97–107. [Google Scholar] [CrossRef]
- Frize, M. A debate on the ethics of body enhancement technologies and regeneration. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Beijing, China, 26–31 May 2012; pp. 2072–2075. [Google Scholar]
- Manovich, L. Trending: The promises and the challenges of big social data. Debates Digit. Hum. 2011, 2, 460–475. [Google Scholar]
- Oliveira, T.; Thomas, M.; Espadanal, M. Assessing the determinants of cloud computing adoption: An analysis of the manufacturing and services sectors. Inf. Manag. 2014, 51, 497–510. [Google Scholar] [CrossRef]
- Lee, S.W. Research on Determinants for Big Data System Adoption in Organization. Ph.D. Thesis, Graduate School of Sungkyunkwan University Seoul, Seoul, Korea, August 2016. [Google Scholar]
- Chong, K.W.; Kim, Y.S.; Choi, J. A Study of Factors Affecting Intention to Adopt a Cloud-Based Digital Signature Service. Information 2021, 12, 60. [Google Scholar] [CrossRef]
- Pan, Y.; Froese, F.; Liu, N.; Hu, Y.; Ye, M. The adoption of artificial intelligence in employee recruitment: The influence of contextual factors. Int. J. Hum. Resour. Manag. 2021, 1–23. [Google Scholar] [CrossRef]
- Wisdom, J.P.; Chor, K.H.B.; Hoagwood, K.E.; Horwitz, S.M.J.A. Innovation adoption: A review of theories and constructs. Adm. Policy Ment. Health Ment. Health Serv. Res. 2014, 41, 480–502. [Google Scholar] [CrossRef] [PubMed]
- Tornatzky, L.G.; Fleischer, M.; Chakrabarti, A.K. Processes of Technological Innovation; Lexington Books: Washington, DC, USA, 1990. [Google Scholar]
- Dedrick, J.; West, J. Why firms adopt open source platforms: A grounded theory of innovation and standards adoption. In Standard Making: A Critical Research Frontier for Information Systems; Management Information Systems Research Center, University of Minnesota: Minneapolis, MN, USA; Saint Paul, MN, USA, 2003; pp. 236–257. [Google Scholar]
- Amron, M.T.; Ibrahim, R.; Bakar, N.A.A.; Chuprat, S. Acceptance of cloud computing in the Malaysian public sector: A proposed model. Int. J. Eng. Bus. Manag. 2019, 11, 1847979019880709. [Google Scholar] [CrossRef] [Green Version]
- Parasuraman, A. Technology Readiness Index (TRI) a multiple-item scale to measure readiness to embrace new technologies. J. Serv. Res. 2000, 2, 307–320. [Google Scholar] [CrossRef]
- Adiyarta, K.; Napitupulu, D.; Nurdianto, H.; Rahim, R.; Ahmar, A. User acceptance of E-Government Services Based on TRAM model. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Banda Aceh, Indonesia, 18–20 October 2017; p. 012057. [Google Scholar]
- Kim, J.K. A Study on the Usage Intention of Category Types in the Mobile Application Based on the Technology Readiness and Acceptance Model. Ph.D. Thesis, Kongju National University, Gongju, Korea, 2013. [Google Scholar]
- Asiaei, A.; Rahim, N.Z.A. A multifaceted framework for adoption of cloud computing in Malaysian SMEs. J. Sci. Technol. Policy Manag. 2019, 10, 708–750. [Google Scholar] [CrossRef]
- Al-Sharafi, M.A.; Arshah, R.A.; Abu-Shanab, E.A. Factors affecting the continuous use of cloud computing services from expert’s perspective. In Proceedings of the TENCON 2017–2017 IEEE Region 10 Conference, Penang, Malaysia, 5–8 November 2017; pp. 986–991. [Google Scholar]
- Ijab, M.T.; Wahab, S.M.A.; Salleh, M.A.M.; Bakar, A.A. Investigating Big Data Analytics Readiness in Higher Education Using the Technology-Organisation-Environment (TOE) Framework. In Proceedings of the 2019 6th International Conference on Research and Innovation in Information Systems (ICRIIS), Johor Bahru, Johor, 2–3 December 2019; pp. 1–7. [Google Scholar]
- Low, C.; Chen, Y.; Wu, M. Understanding the determinants of cloud computing adoption. Ind. Manag. Data Syst. 2011, 111, 1006–1023. [Google Scholar] [CrossRef] [Green Version]
- Nkhoma, M.Z.; Dang, D.; De Souza-Daw, A. Contributing factors of cloud computing adoption: A technology-organisation-environment framework approach. In Proceedings of the European Conference on Information Management & Evaluation, University College Dublin (UCD), School of Politics and International Relations, Ho Chi Minh City, Vietnam, 13–14 May 2013; pp. 180–188. [Google Scholar]
- Awa, H.O.; Ojiabo, O.U. A model of adoption determinants of ERP within TOE framework. Inf. Technol. People 2016, 29, 901–930. [Google Scholar] [CrossRef]
- Oliveira, T.; Martins, M.F. Literature review of information technology adoption models at firm level. Electron. J. Inf. Syst. Eval. 2011, 14, 110–121. [Google Scholar]
- Williams, M.D.; Rana, N.P.; Dwivedi, Y.K. A bibliometric analysis of articles citing the unified theory of acceptance and use of technology. In Information Systems Theory; Springer: Berlin, Germany, 2012; pp. 37–62. [Google Scholar]
- Awa, H.O.; Ojiabo, O.U.; Orokor, L.E. Integrated technology-organization-environment (TOE) taxonomies for technology adoption. J. Enterp. Inf. Manag. 2017, 30, 893–921. [Google Scholar] [CrossRef]
- Martins, M.; Oliveira, T. Determinants of e-commerce adoption by small firms in Portugal. In Proceedings of the 3rd European Conference on Information Management and Evaluation, Gothenburg, Sweden, 17–18 September 2009; pp. 328–338. Available online: https://novaresearch.unl.pt/en/publications/determinants-of-e-commerce-adoption-by-small-firms-in-portugal (accessed on 23 July 2021).
- Oliveira, T.; Martins, M.F. A Comparison of Web Site Adoption in Small and Large Portuguese Firms. In Proceedings of the International Conference on e-Business, Porto, Portugal, 26–29 July 2008; pp. 370–377. [Google Scholar]
- Zhu, K.; Kraemer, K.L.; Xu, S. The process of innovation assimilation by firms in different countries: A technology diffusion perspective on e-business. Manag. Sci. 2006, 52, 1557–1576. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, T.; Martins, M.F. Information technology adoption models at firm level: Review of literature. In Proceedings of the European Conference on Information Systems Management, Academic Conferences International Limited, Lisbon, Portugal, 9–10 September 2010; p. 312. [Google Scholar]
- Rogers, E. The Diffusion of Innovations, 4th ed.; The Free Press, Simon and Schuster: New York, NY, USA, 1995. [Google Scholar]
- Greenhalgh, T.; Robert, G.; Macfarlane, F.; Bate, P.; Kyriakidou, O. Diffusion of innovations in service organizations: Systematic review and recommendations. Milbank Q. 2004, 82, 581–629. [Google Scholar] [CrossRef] [Green Version]
- Fichman, R.G. The diffusion and assimilation of information technology innovations. Proj. Future Through Past 2000, 105127, 105–128. [Google Scholar]
- Tarofder, A.K.; Jawabri, A.; Haque, A.; Sherief, S.R. Validating technology-organization-Environment (TOE) framework in web 2.0 adoption in supply chain management. Ind. Eng. Manag. Syst. 2019, 18, 482–494. [Google Scholar] [CrossRef]
- Yusif, S.; Hafeez-Baig, A.; Soar, J. A model for evaluating eHealth preparedness–a case study approach. Transform. Gov. People Process. Policy 2020, 14, 561–587. [Google Scholar] [CrossRef]
- Qasem, Y.A.; Abdullah, R.; Yaha, Y.; Atana, R. Continuance Use of Cloud Computing in Higher Education Institutions: A Conceptual Model. Appl. Sci. 2020, 10, 6628. [Google Scholar] [CrossRef]
- Shahbaz, M.; Gao, C.; Zhai, L.; Shahzad, F.; Hu, Y. Investigating the adoption of big data analytics in healthcare: The moderating role of resistance to change. J. Big Data 2019, 6, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Maroufkhani, P.; Ismail, W.K.W.; Ghobakhloo, M. Big data analytics adoption model for small and medium enterprises. J. Sci. Technol. Policy Manag. 2020, 11, 483–513. [Google Scholar] [CrossRef]
- Cabrera-Sánchez, J.-P.; Villarejo-Ramos, A.F. Factors affecting the adoption of big data analytics in companies. Rev. Adm. Empresas 2020, 59, 415–429. [Google Scholar] [CrossRef]
- Sahid, N.Z.; Sani, M.K.J.A.; Noordin, S.A.; Zaini, M.K.; Baba, J. Determinants factors of intention to adopt big data analytics in Malaysian public agencies. J. Ind. Eng. Manag. 2021, 14, 269–293. [Google Scholar]
- Ram, J.; Afridi, N.K.; Khan, K.A. Adoption of Big Data analytics in construction: Development of a conceptual model. Built Environ. Proj. Asset Manag. 2019, 9, 564–579. [Google Scholar] [CrossRef]
- Awa, H.O.; Ukoha, O.; Igwe, S.R. Revisiting technology-organization-environment (TOE) theory for enriched applicability. Bottom Line 2017, 30, 2–22. [Google Scholar] [CrossRef]
- Van Deursen, N.; Buchanan, W.J.; Duff, A. Monitoring information security risks within health care. Comput. Secur. 2013, 37, 31–45. [Google Scholar] [CrossRef]
- Yang, Z.; Sun, J.; Zhang, Y.; Wang, Y. Understanding SaaS adoption from the perspective of organizational users: A tripod readiness model. Comput. Hum. Behav. 2015, 45, 254–264. [Google Scholar] [CrossRef]
- Bag, S.; Wood, L.C.; Xu, L.; Dhamija, P.; Kayikci, Y. Big data analytics as an operational excellence approach to enhance sustainable supply chain performance. Resour. Conserv. Recycl. 2020, 153, 104559. [Google Scholar] [CrossRef]
- Raguseo, E. Big data technologies: An empirical investigation on their adoption, benefits and risks for companies. International J. Inf. Manag. 2018, 38, 187–195. [Google Scholar] [CrossRef]
- Troshani, I.; Rampersad, G.; Plewa, C. Adopting innovation management software in university innovation commercialization. J. Comput. Inf. Syst. 2011, 52, 83–92. [Google Scholar]
- Hernandez-Munoz, L.; Torane, M.; Amini, A.; Vivekanandan-Dhukaram, A. A state-of-the-art analysis of innovation models and innovation software tools. In Proceedings of the European Conference on Innovation and Entrepreneurship, Lisbon, Portugal, 16–17 September 2021; p. 237. [Google Scholar]
- Saghafian, M.; Laumann, K.; Skogstad, M.R. Stagewise Overview of Issues Influencing Organizational Technology Adoption and Use. Front. Psychol. 2021, 12, 654. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Zhang, W.; Li, H.; Bose, R.; Chung, Q.B. Cloud computing capability: Its technological root and business impact. J. Organ. Comput. Electron. Commer. 2018, 28, 193–213. [Google Scholar] [CrossRef]
- Rather, M.-K.; Rather, S.-A. Impact of smartphones on young generation. Libr. Philos. Pract. 2019, 10, 1–9. [Google Scholar]
- Giotopoulos, I.; Kontolaimou, A.; Korra, E.; Tsakanikas, A. What drives ICT adoption by SMEs? Evidence from a large-scale survey in Greece. J. Bus. Res. 2017, 81, 60–69. [Google Scholar] [CrossRef]
- Subramani Parasuraman, A.T.S.; Yee, S.W.K.; Chuon, B.L.C.; Ren, L.Y. Smartphone usage and increased risk of mobile phone addiction: A concurrent study. Int. J. Pharm. Investig. 2017, 7, 125. [Google Scholar] [CrossRef]
- Baig, M.I.; Shuib, L.; Yadegaridehkordi, E. Big data in education: A state of the art, limitations, and future research directions. Int. J. Educ. Technol. High. Educ. 2020, 17, 1–23. [Google Scholar] [CrossRef]
- Silow-Carroll, S.; Edwards, J.N.; Rodin, D. Using electronic health records to improve quality and efficiency: The experiences of leading hospitals. Issue Brief 2012, 17, 40. [Google Scholar]
- Kapoor, K.K.; Dwivedi, Y.K.; Williams, M.D. Empirical examination of the role of three sets of innovation attributes for determining adoption of IRCTC mobile ticketing service. Inf. Syst. Manag. 2015, 32, 153–173. [Google Scholar] [CrossRef] [Green Version]
- Baker, J. The technology–organization–environment framework. Inf. Syst. Theory 2012, 28, 231–245. [Google Scholar]
- Gu, V.C.; Cao, Q.; Duan, W. Unified Modeling Language (UML) IT adoption—A holistic model of organizational capabilities perspective. Decis. Support Syst. 2012, 54, 257–269. [Google Scholar] [CrossRef]
- Rogers, E.M.; Singhal, A.; Quinlan, M.M. Diffusion of Innovations; Routledge: London, UK, 2014. [Google Scholar]
- Bolonne, H.; Wijewardene, P. Critical Factors Affecting the Intention to Adopt Big Data Analytics in Apparel Sector, Sri Lanka. Int. J. Adv. Comput. Sci. Appl. 2020, 11. [Google Scholar] [CrossRef]
- Sharma, M.; Gupta, R.; Acharya, P. Analysing the adoption of cloud computing service: A systematic literature review. Glob. Knowl. Mem. Commun. 2020, 70, 114–153. [Google Scholar] [CrossRef]
- Maroufkhani, P.; Tseng, M.-L.; Iranmanesh, M.; Ismail, W.K.W.; Khalid, H. Big data analytics adoption: Determinants and performances among small to medium-sized enterprises. Int. J. Inf. Manag. 2020, 54, 102190. [Google Scholar] [CrossRef]
- Harindranath, G.; Dyerson, R.; Barnes, D. ICT in small firms: Factors affecting the adoption and use of ICT in Southeast England SMEs. Int. J. Adv. Comput. Sci. Appl. 2008, 11. Available online: https://www.researchgate.net/publication/221408742_ICT_in_small_firms_Factors_affecting_the_adoption_and_use_of_ICT_in_southeast_England_SMEs (accessed on 8 May 2021).
- Kandil, A.M.N.A.; Ragheb, M.A.; Ragab, A.A.; Farouk, M. Examining the effect of TOE model on cloud computing adoption in Egypt. Bus. Manag. Rev. 2018, 9, 113–123. [Google Scholar]
- Alshamaila, Y.; Papagiannidis, S.; Li, F. Cloud computing adoption by SMEs in the north east of England. J. Enterp. Inf. Manag. 2013, 26, 250–275. [Google Scholar] [CrossRef] [Green Version]
- Rowe, F.; Truex, D.; Huynh, M.Q. An empirical study of determinants of e-commerce adoption in SMEs in Vietnam: An economy in transition. J. Glob. Inf. Manag. JGIM 2012, 20, 23–54. [Google Scholar]
- Gangwar, H. Understanding the determinants of big data adoption in India: An analysis of the manufacturing and services sectors. Inf. Resour. Manag. J. IRMJ 2018, 31, 1–22. [Google Scholar] [CrossRef]
- Lai, Y.; Sun, H.; Ren, J. Understanding the determinants of big data analytics (BDA) adoption in logistics and supply chain management. Int. J. Logist. Manag. 2018, 29, 676–703. [Google Scholar] [CrossRef]
- Chen, D.Q.; Preston, D.S.; Swink, M. How the use of big data analytics affects value creation in supply chain management. J. Manag. Inf. Syst. 2015, 32, 4–39. [Google Scholar] [CrossRef]
- Ren, J.-F.; Fosso Wamba, S.; Akter, S.; Dubey, R.; Childe, S.J. Modelling quality dynamics on business value and firm performance in big data analytics environment. Int. J. Prod. Res. 2017, 55, 5011–5026. [Google Scholar]
- Wamba, S.F.; Gunasekaran, A.; Akter, S.; Ren, S.J.-f.; Dubey, R.; Childe, S.J. Big data analytics and firm performance: Effects of dynamic capabilities. J. Bus. Res. 2017, 70, 356–365. [Google Scholar] [CrossRef] [Green Version]
- Jarrar, Y.; Awobamise, A.; Sellos, P. Technological Readiness Index (TRI) and the intention to use smartphone apps for tourism: A focus on inDubai mobile tourism app. Int. J. Data Netw. Sci. 2020, 4, 297–304. [Google Scholar] [CrossRef]
- Anjum, N.; Islam, M.A. Employees’ Behavioral Intention to Adopt E-HRM System-An Approach to Extend Technology Acceptance Model. Int. J. Acad. Res. Account. Financ. Manag. Sci. 2020. [Google Scholar] [CrossRef]
- Chen, S.-C.; Li, S.-H.; Liu, S.-C.; Yen, D.C.; Ruangkanjanases, A. Assessing Determinants of Continuance Intention towards Personal Cloud Services: Extending UTAUT2 with Technology Readiness. Symmetry 2021, 13, 467. [Google Scholar] [CrossRef]
- Sarkar, A.; Qian, L.; Peau, A.K. Structural equation modeling for three aspects of green business practices: A case study of Bangladeshi RMG’s industry. Environ. Sci. Pollut. Res. 2020, 27, 35750–35768. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.F.; Dominic, P.; Ali, K. Organizational governance, social bonds and information security policy compliance: A perspective towards oil and gas employees. Sustainability 2020, 12, 8576. [Google Scholar] [CrossRef]
- Shim, H.-S.; Han, S.-L.; Ha, J. The Effects of Consumer Readiness on the Adoption of Self-Service Technology: Moderating Effects of Consumer Traits and Situational Factors. Sustainability 2021, 13, 95. [Google Scholar] [CrossRef]
- Ali, R.F.; Dominic, P.; Karunakaran, P.K. Information security policy and compliance in oil and gas organizations—A pilot study. Solid State Technol. 2020, 63, 1275–1282. [Google Scholar]
- Sanders, N.R. Pattern of information technology use: The impact on buyer–suppler coordination and performance. J. Oper. Manag. 2008, 26, 349–367. [Google Scholar] [CrossRef]
- Jahanshahi, A.A.; Brem, A. Sustainability in SMEs: Top management teams behavioral integration as source of innovativeness. Sustainability 2017, 9, 1899. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jesus, F.; Pinheiro, A.; Oliveira, T. Understanding CRM adoption stages: Empirical analysis building on the TOE framework. Comput. Ind. 2019, 109, 1–13. [Google Scholar] [CrossRef]
- Wang, L.; Yang, M.; Pathan, Z.H.; Salam, S.; Shahzad, K.; Zeng, J. Analysis of influencing factors of big data adoption in Chinese enterprises using DANP technique. Sustainability 2018, 10, 3956. [Google Scholar] [CrossRef] [Green Version]
- Nabhani, I.; Daryanto, A.; Rifin, A. Mobile broadband for the farmers: A case study of technology adoption by cocoa farmers in Southern East Java, Indonesia. AGRIS On-Line Pap. Econ. Inform. 2016, 8, 111–120. [Google Scholar] [CrossRef] [Green Version]
- Mukred, M.; Yusof, Z.M.; Al-Moallemi, W.A.; Mokhtar, U.A.A.; Hawash, B. Electronic records management systems and the competency of educational institutions: Evidence from Yemen. Inf. Dev. 2021. [Google Scholar] [CrossRef]
- Walker, J.H.; Saffu, K.; Mazurek, M. An empirical study of factors influencing e-commerce adoption/non-adoption in Slovakian SMEs. J. Internet Commer. 2016, 15, 189–213. [Google Scholar] [CrossRef]
- Premkumar, G.; Ramamurthy, K.; Crum, M. Determinants of EDI adoption in the transportation industry. Eur. J. Inf. Syst. 1997, 6, 107–121. [Google Scholar] [CrossRef]
- Vaishnavi, V.; Suresh, M.; Dutta, P. Modelling the readiness factors for agility in healthcare organization: A TISM approach. Benchmark. An Int. J. 2019, 26, 2372–2400. [Google Scholar] [CrossRef]
- Ruivo, P.; Johansson, B.; Sarker, S.; Oliveira, T. The relationship between ERP capabilities, use, and value. Comput. Ind. 2020, 117, 103209. [Google Scholar] [CrossRef]
- Xu, W.; Ou, P.; Fan, W. Antecedents of ERP assimilation and its impact on ERP value: A TOE-based model and empirical test. Inf. Syst. Front. 2017, 19, 13–30. [Google Scholar] [CrossRef]
- Ghobakhloo, M.; Arias-Aranda, D.; Benitez-Amado, J. Adoption of e-commerce applications in SMEs. Ind. Manag. Data Syst. 2011. [Google Scholar] [CrossRef]
- Grandon, E.E.; Pearson, J.M. Electronic commerce adoption: An empirical study of small and medium US businesses. Inf. Manag. 2004, 42, 197–216. [Google Scholar] [CrossRef]
- Aboelmaged, M. The drivers of sustainable manufacturing practices in Egyptian SMEs and their impact on competitive capabilities: A PLS-SEM model. J. Clean. Prod. 2018, 175, 207–221. [Google Scholar] [CrossRef]
- Lautenbach, P.; Johnston, K.; Adeniran-Ogundipe, T. Factors influencing business intelligence and analytics usage extent in South African organisations. S. Afr. J. Bus. Manag. 2017, 48, 23–33. [Google Scholar] [CrossRef]
- Chang, I.-C.; Hwang, H.-G.; Hung, M.-C.; Lin, M.-H.; Yen, D.C. Factors affecting the adoption of electronic signature: Executives’ perspective of hospital information department. Decis. Support Syst. 2007, 44, 350–359. [Google Scholar] [CrossRef]
- Premkumar, G.; Ramamurthy, K. The role of interorganizational and organizational factors on the decision mode for adoption of interorganizational systems. Decis. Sci. 1995, 26, 303–336. [Google Scholar] [CrossRef]
- Saeed, I.; Juell-Skielse, G.; Uppström, E. Cloud enterprise resource planning adoption: Motives & barriers. Adv. Enterp. Inf. Syst. II 2012, 429. [Google Scholar]
- Amini, M.; Sadat Safavi, N.; Mirzaeyan Bahnamiri, R.; Mirzaei Omran, M.; Amini, M. Development of an instrument for assessing the impact of environmental context on adoption of cloud computing for small and medium enterprises. Aust. J. Basic Appl. Sci. AJBAS 2014, 8, 129–135. [Google Scholar]
- Li, Y.-h. An empirical investigation on the determinants of e-procurement adoption in Chinese manufacturing enterprises. In Proceedings of the 2008 International Conference on Management Science and Engineering 15th Annual Conference Proceedings, Long Beach, CA, USA, 10–12 September 2008; pp. 32–37. [Google Scholar]
- Abd Elmonem, M.A.; Nasr, E.S.; Geith, M.H. Benefits and challenges of cloud ERP systems–A systematic literature review. Future Comput. Inf. J. 2016, 1, 1–9. [Google Scholar] [CrossRef]
- Lin, J.S.C.; Hsieh, P.l. The role of technology readiness in customers’ perception and adoption of self-service technologies. Int. J. Serv. Ind. Manag. 2006, 17, 497–517. [Google Scholar] [CrossRef]
- Ifinedo, P. Internet/e-business technologies acceptance in Canada’s SMEs: An exploratory investigation. Internet Res. 2011, 21, 255–281. [Google Scholar] [CrossRef]
- Tashkandi, A.; Al-Jabri, I. Cloud computing adoption by higher education institutions in Saudi Arabia: Analysis based on TOE. In Proceedings of the 2015 International Conference on Cloud Computing (ICCC), Riyadh, Saudi Arabia, 26–29 April 2015; pp. 1–8. [Google Scholar]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage Publishers: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Gefen, D.; Rigdon, E.E.; Straub, D. Editor’s comments: An update and extension to SEM guidelines for administrative and social science research. Mis Q. 2011, 32, iii-xiv. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford publications: New York, NY, USA, 2015. [Google Scholar]
- Ringle, C.M.; Wende, S.; Becker, J.-M. SmartPLS 3; SmartPLS GmbH: Boenningstedt, Germany, 2015. [Google Scholar]
- Chin, W.W.; Marcolin, B.L.; Newsted, P.R. A partial least squares latent variable modeling approach for measuring interaction effects: Results from a Monte Carlo simulation study and an electronic-mail emotion/adoption study. Inf. Syst. Res. 2003, 14, 189–217. [Google Scholar] [CrossRef] [Green Version]
- Kock, N. Common method bias in PLS-SEM: A full collinearity assessment approach. Int. J. e-Collab. 2015, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kock, N.; Lynn, G. Lateral collinearity and misleading results in variance-based SEM: An illustration and recommendations. J. Assoc. Inf. Syst. 2012, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Sarstedt, M.; Ringle, C.M. Rethinking some of the rethinking of partial least squares. Eur. J. Mark. 2019, 53, 566–583. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Ramayah, T.; Cheah, J.; Chuah, F.; Ting, H.; Memon, M. Partial least squares structural equation modeling (PLS-SEM) using smartPLS 3.0. In An Updated Guide and Practical Guide to Statistical Analysis; Pearson: London, UK, 2018. [Google Scholar]
- Sarstedt, M.; Ringle, C.M.; Hair, J.F. Partial least squares structural equation modeling. Handb. Mark. Res. 2017, 26, 1–40. [Google Scholar]
- Hair, J.F., Jr.; Sarstedt, M.; Hopkins, L.; Kuppelwieser, V.G. Partial least squares structural equation modeling (PLS-SEM). Eur. Bus. Rev. 2014, 26, 106–121. [Google Scholar] [CrossRef]
- Yadegaridehkordi, E.; Nilashi, M.; Shuib, L.; Nasir, M.H.N.B.M.; Asadi, S.; Samad, S.; Awang, N.F. The impact of big data on firm performance in hotel industry. Electron. Commer. Res. Appl. 2020, 40, 100921. [Google Scholar] [CrossRef]
- Kim, T.; Chiu, W. Consumer acceptance of sports wearable technology: The role of technology readiness. Int. J. Sports Mark. Spons. 2019, 20, 109–126. [Google Scholar] [CrossRef]
- Nejati, M.; Rabiei, S.; Jabbour, C.J.C. Envisioning the invisible: Understanding the synergy between green human resource management and green supply chain management in manufacturing firms in Iran in light of the moderating effect of employees’ resistance to change. J. Clean. Prod. 2017, 168, 163–172. [Google Scholar] [CrossRef]
- Agrawal, K. Investigating the determinants of Big Data Analytics (BDA) Adoption in Asian Emerging Economies. Available online: https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.911.3875&rep=rep1&type=pdf (accessed on 17 May 2021).
- Gutierrez, A.; Boukrami, E.; Lumsden, R. Technological, organisational and environmental factors influencing managers’ decision to adopt cloud computing in the UK. J. Enterp. Inf. Manag. 2015, 28, 788–807. [Google Scholar] [CrossRef]
- Zhu, K.; Dong, S.; Xu, S.X.; Kraemer, K.L. Innovation diffusion in global contexts: Determinants of post-adoption digital transformation of European companies. Eur. J. Inf. Syst. 2006, 15, 601–616. [Google Scholar] [CrossRef]
- Chiu, W.; Cho, H. The role of technology readiness in individuals’ intention to use health and fitness applications: A comparison between users and non-users. Asia Pac. J. Mark. Logist. 2020, 33, 807–825. [Google Scholar] [CrossRef]
- Parasuraman, A.; Colby, C.L. An updated and streamlined technology readiness index: TRI 2.0. J. Serv. Res. 2015, 18, 59–74. [Google Scholar] [CrossRef]
- Nugroho, M.A.; Fajar, M.A. Effects of technology readiness towards acceptance of mandatory web-based attendance system. Procedia Comput. Sci. 2017, 124, 319–328. [Google Scholar] [CrossRef]
- Ragu-Nathan, B.S.; Apigian, C.H.; Ragu-Nathan, T.; Tu, Q. A path analytic study of the effect of top management support for information systems performance. Omega 2004, 32, 459–471. [Google Scholar] [CrossRef]
- Weill, P. The relationship between investment in information technology and firm performance: A study of the valve manufacturing sector. Inf. Syst. Res. 1992, 3, 307–333. [Google Scholar] [CrossRef] [Green Version]
- Premkumar, G.; Potter, M. Adoption of computer aided software engineering (CASE) technology: An innovation adoption perspective. Adv. Inf. Syst. 1995, 26, 105–124. [Google Scholar] [CrossRef]
- Lian, J.-W.; Yen, D.C.; Wang, Y.-T. An exploratory study to understand the critical factors affecting the decision to adopt cloud computing in Taiwan hospital. Int. J. Inf. Manag. 2014, 34, 28–36. [Google Scholar] [CrossRef]
- Jamoom, E.W.; Patel, V.; Furukawa, M.F.; King, J. EHR adopters vs. non-adopters: Impacts of, barriers to, and federal initiatives for EHR adoption. Healthcare 2014, 2, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Tung, F.-C.; Chang, S.-C.; Chou, C.-M. An extension of trust and TAM model with IDT in the adoption of the electronic logistics information system in HIS in the medical industry. Int. J. Med. Inf. 2008, 77, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Chan, F.T.; Chong, A.Y.-L. Determinants of mobile supply chain management system diffusion: A structural equation analysis of manufacturing firms. Int. J. Prod. Res. 2013, 51, 1196–1213. [Google Scholar] [CrossRef]
- Stratman, J.K.; Roth, A.V. Enterprise resource planning (ERP) competence constructs: Two-stage multi-item scale development and validation. Decis. Sci. 2002, 33, 601–628. [Google Scholar] [CrossRef]
- Gupta, H.; Barua, M.K. Identifying enablers of technological innovation for Indian MSMEs using best–worst multi criteria decision making method. Technol. Forecast. Soc. Change 2016, 107, 69–79. [Google Scholar] [CrossRef]
- Raghavan, A.; Demircioglu, M.A.; Taeihagh, A. Public Health Innovation through Cloud Adoption: A Comparative Analysis of Drivers and Barriers in Japan, South Korea, and Singapore. Int. J. Environ. Res. Public Health 2021, 18, 334. [Google Scholar] [CrossRef] [PubMed]
- Mukred, M.; Yusof, Z.M.; Alotaibi, F.M.; Asma’Mokhtar, U.; Fauzi, F.J.I.A. The Key Factors in Adopting an Electronic Records Management System (ERMS) in the Educational Sector: A UTAUT-Based Framework. IEEE Access 2019, 7, 35963–35980. [Google Scholar] [CrossRef]
- Long, T.B.; Blok, V.; Coninx, I. Barriers to the adoption and diffusion of technological innovations for climate-smart agriculture in Europe: Evidence from the Netherlands, France, Switzerland and Italy. J. Clean. Prod. 2016, 112, 9–21. [Google Scholar] [CrossRef]
- Gangwar, H.; Date, H.; Ramaswamy, R. Understanding determinants of cloud computing adoption using an integrated TAM-TOE model. J. Enterp. Inf. Manag. 2015, 28, 107–130. [Google Scholar] [CrossRef]
- Nugroho, M.A. Impact of government support and competitor pressure on the readiness of SMEs in Indonesia in adopting the information technology. Procedia Comput. Sci. 2015, 72, 102–111. [Google Scholar] [CrossRef] [Green Version]
- Sam, K.M.; Chatwin, C.R. Understanding adoption of Big data analytics in China: From organizational users perspective. In Proceedings of the 2018 IEEE International Conference on Industrial Engineering and Engineering Management (IEEM), Bangkok, Thailand, 16–19 December 2018; pp. 507–510. [Google Scholar]




| Study | Title | Theory | Method | Findings | Limitations |
|---|---|---|---|---|---|
| [71] | A Study of Factors Affecting Intention to Adopt a Cloud-Based Digital Signature Service | TOE | Survey | Management collaboration and support influence suitability. | Study was conducted in a developed country. |
| The invention has no evident influence on service readiness or appropriateness. This confirms Parasuraman’s results. | |||||
| [10] | The Effect of Organizational Information Security Climate on Information Security Policy Compliance: The Mediating Effect of Social Bonding towards Healthcare Employees | TPB and others | survey | The top management increases social IS activities that help staff attitudes towards ISPC. | Data obtained solely from public hospitals, 30 out of 120 institutions. |
| [98] | Continuance Use of Cloud Computing in Higher Education Institutions: A Conceptual Model | TOE, DOI, IS UTAT, TAM, and others | survey | The current study investigated the most important reasons why HEIs employ CC services. | Study was done in a developed country. |
| [99] | Investigating the adoption of big data analytics in healthcare: the moderating role of resistance to change | TTF and TAM | Survey/quantitative | It is revealed that technological and organizational factors are the most significant predictors of BDA adoption in the context of SMEs. | A small number of variables were investigated. |
| [100] | Big data analytics adoption model for small and medium enterprises | TOE | Survey | The data indicate that TOE circumstances have a considerable impact. | The study was conducted in a developed country. |
| BDA adoption has a beneficial influence on its adoption, and BDA adoption increases the performance of SMEs. | |||||
| [101] | Factors Affecting the Adoption of Big Data Analytics in Companies | UTAUT | survey | Behavioral intent to use BDA in companies. | This research did not include organizational culture, factors that may affect the amount of adoption of this method. |
| [102] | Determinants Factors of Intention to Adopt Big Data Analytics in Malaysian Public Agencies | Survey | To identify the critical model, which public agencies would find beneficial in funding decisions and when creating outreach initiatives. | Small dataset for analysis | |
| [103] | Adoption of BD analytics in construction: development of a conceptual mode | TOE | Survey | Will allow managers (e.g., IT/IS managers, and business and senior management) to understand the driving forces behind construction BD adoption and plan their own BD adoption. | Only three adoption criteria and creates a new conceptual model to study developing technology acceptability. |
| [80] | A multifaceted framework for adoption of cloud computing in Malaysian SMEs | TOE, DOI, and TAM | survey | Intentions to use cloud computing can operate as a mediator between TOE variables and cloud computing adoption. | This study included a single informant for each enterprise. The subsequent research may examine the micro-foundations of routines. |
| [104] | Revisiting technology–organization–environment (TOE) theory for enriched applicability | TOE | survey | Indicate that elements in the technical, organizational, and environmental contexts all have a direct statistically significant link to adoption; hence, adoption is more influenced by T–O–E variables than by individual characteristics. | Extended data are needed to apply the findings to different sectors, industries, and nations and to include the implementation and post-adoption stages and business-to-business (B2B) adoption to construct a more holistic framework. |
| [105] | Monitoring information security risks within the health care | NA | survey | Inadequate procedures of healthcare employees cause most security breaches. | A study was done in a developed nation and mostly tech issues and solutions. |
| Demographic Variable | Categories | Frequency (n = 254) | Percentage (%) |
|---|---|---|---|
| Age (range in years) | 20–30 | 103 | 35 |
| 31–40 | 92 | 30 | |
| 41–50 | 67 | 22 | |
| 51–60 | 41 | 13 | |
| Education | Undergraduate | 173 | 58 |
| Graduate | 130 | 42 | |
| Sector | Public | 187 | 62 |
| Private | 116 | 38 | |
| Position | Doctor/Nurse | 100 | 33 |
| IT Staff | 203 | 67 | |
| Years of experience | 1–5 | 122 | 45 |
| 6–15 | 93 | 28 | |
| 16–25 | 42 | 12 | |
| 26–35 | 46 | 15 | |
| Information Technology Competence | Low | 132 | 44 |
| High | 171 | 56 | |
| Daily usage of computers (hours) | 4–7 | 93 | 30 |
| 8–11 | 164 | 55 | |
| More than 11 | 46 | 15 | |
| Awareness of Technology | Not aware | 49 | 16 |
| Somewhat aware | 68 | 23 | |
| Very much aware | 186 | 61 |
| Criterion | Acceptable Threshold Values |
|---|---|
| Reliability | For this survey questionnaire, two reliability criteria were followed. |
| Content validity | The validity of content relates to how effectively the construct’s domain content is captured by its indicators [165]. The thorough examination demonstrates how closely an individual item represents the concept being assessed [166]. |
| Construct validity | The construct validity defined as the degree to which a test assesses what it claims to measure. Construct validity also refers to the degree to which test findings are used to identify the link between measurement items and the constructs in question.
|
| CX | CT | TMS | FS | TR | GITP | GLAL | BDR | IABD |
|---|---|---|---|---|---|---|---|---|
| 1.651 | 1.721 | 2.021 | 2.032 | 1.652 | 1.451 | 2.011 | 1.687 | 1.623 |
| Constructs | Items | Reliability | |||
|---|---|---|---|---|---|
| Cronbach’s Alpha | rho_A | CR | AVE | ||
| Complexity (CX) | |||||
| BD allows me to manage business operations in an efficient way. | CX1 | 0.883 | 0.884 | 0.985 | 0.751 |
| The use of BD is frustrating. | CX2 | ||||
| The skills needed to improve and use the new technologies are easy for me. | CX3 | ||||
| The use of BD requires a lot of mental effort. | CX4 | ||||
| Compatibility (CT) | |||||
| The use of BD is compatible with my healthcare corporate culture and value system. | CT1 | 0.894 | 0.898 | 0.952 | 0.665 |
| The use of BD will be compatible with existing hardware and software. | CT2 | ||||
| BD is easy to use and manage. | CT3 | ||||
| BD is compatible with existing emerging technologies. | CT4 | ||||
| Optimism (OP) | |||||
| New technologies contribute to a better quality of life. | OP1 | 0.882 | 0.898 | 0.892 | 0.663 |
| Technology gives me more freedom of mobility. | OP2 | ||||
| Technology gives people more control over their daily lives. | OP3 | ||||
| Technology makes me more productive in my personal life. | OP4 | ||||
| Technology makes me more efficient in my occupation. | OP5 | ||||
| Top Management support (TMS) | |||||
| Top management supports plans to adopt the big data. | TMS1 | 0.872 | 0.873 | 0.982 | 0.712 |
| Top management will support the implementation of BD adoption. | TMS2 | ||||
| Top management support is important to provide the resources for the company to adopt big data. | TMS3 | ||||
| The healthcare management is willing to take risks (financial and organizational) involved in the adoption of big data. | TMS4 | ||||
| The firm size compatible with the adoption of big data. | TMS5 | ||||
| Financial support (FS) | |||||
| Financial support is important for purchasing new technology equipment. | FS1 | 0.868 | 0.869 | 0.852 | 0.689 |
| Financial support for the BD technology will strengthen the current system infrastructure in healthcare. | FS1 | ||||
| Financial support will help to better secure the patient’s data. | FS1 | ||||
| My company has the financial resources to purchase the hardware and software required for technologies. | FS4 | ||||
| Training (TR) | |||||
| Training on the BD usage is meeting my requirements. | TR1 | 0.860 | 0.862 | 0.971 | 0.721 |
| Training on BD usage ensures that employees have received the appropriate training. | TR2 | ||||
| Training on BD usage is adequate for all involved staff. | TR3 | ||||
| All users have been trained in basic technology skills in the healthcare system. | TR4 | ||||
| Government IT policies (GITP) | |||||
| Government IT policy can attract more foreign investors to invest in sustainable businesses. | GITP1 | 0.750 | 0.750 | 0.902 | 0.753 |
| Government IT policy can encourage sustainable technology usage. | GITP2 | ||||
| Government IT policy can improve sustainable technology efficiency. | GITP3 | ||||
| Government IT policy can educate sustainable technology in Malaysian on the benefits of sustainable technology. | GITP4 | ||||
| There is a lack of security rules, IT policies, and privacy laws. | GITP5 | ||||
| Government lows and legislations (GLAL) | |||||
| The laws and regulation that exist nowadays are sufficient to protect the use of big data. | GLAL1 | 0.829 | 0.829 | 0.895 | 0.663 |
| The government drives the use of the BD through incentive programs. | GLAL2 | ||||
| The company requires maintaining the regulatory environment in the use of big data. | GLAL3 | ||||
| The laws and regulations of the government support BD initiatives and implementation. | GLAL4 | ||||
| Government laws and regulations can provide a better process for adopting technologies. | GLAL5 | ||||
| BD Readiness (BDR) in Healthcare Sector | |||||
| The healthcare management understands how they can be used in the healthcare sector. | BDR1 | 0.901 | 0.895 | 0.965 | 0.669 |
| The healthcare IT infrastructure is good (internet service/devices) and can be used for big data. | BDR2 | ||||
| The healthcare management already promoted the usage of the BD to the staff very well. | BDR3 | ||||
| The healthcare staff have the right skills to work with big data. | BDR4 | ||||
| The healthcare IT department and the healthcare management have the right skills to lead the healthcare transformation, and they give very good support to help the staff. | BDR5 | ||||
| Intention to adoption BD (ITABD) | |||||
| BD adoption is effective to enhance the behavioral intentions to use the BD analytics system in healthcare. | ITABD 1 | 0.925 | 0.882 | 0.856 | 0.603 |
| BD technology adoption will increase the performance and effectiveness of healthcare. | ITABD 2 | ||||
| I would use BD technology adoption to gather health data. | ITABD 3 | ||||
| I would use the services provided by use BD technology adoption. | ITABD 4 | ||||
| I would not hesitate to provide information for use BD technology adoption | ITABD 5 | ||||
| Latent Construct | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) |
|---|---|---|---|---|---|---|---|---|---|---|
| CX (1) | -- | |||||||||
| CT (2) | 0.451 | -- | ||||||||
| OP (3) | 0.612 | 0.554 | -- | |||||||
| TMS (4) | 0.621 | 0.412 | 0.289 | -- | ||||||
| FS (5) | 0.355 | 0.423 | 0.287 | 0.521 | -- | |||||
| TR (6) | 0.451 | 0.414 | 0.356 | 0.321 | 0.561 | -- | ||||
| GITP (7) | 0.321 | 0.208 | 0.206 | 0.572 | 0.451 | 0.486 | -- | |||
| GLAL (8) | 0.257 | 0.209 | 0.258 | 0.365 | 0.254 | 0.425 | 0.210 | -- | ||
| BDR (9) | 0.265 | 0.207 | 0.236 | 0.211 | 0.361 | 0.352 | 0.325 | 0.321 | -- | |
| IABD (10) | 0.268 | 0.298 | 0.354 | 0.203 | 0.262 | 0.261 | 0.421 | 0.321 | 0.220 | -- |
| Hypothesis | Path | Beta-Value (n = 254) | t-Value Deviation | p-Value | f2 | Result |
|---|---|---|---|---|---|---|
| H1 | CX ≥ BDR | 0.092 | 0.712 | 1.202 | 0.002 | Not Significant |
| H2 | CT ≥ BDR | 0.267 | 4.730 | 0.006 | 0.027 | Significant |
| H3 | OP ≥ BDR | 0.232 | 3.332 | 0.020 | 0.207 | Significant |
| H4 | TMS ≥ BDR | 0.657 | 9.763 | 0.000 | 0.231 | Significant |
| H5 | FS ≥ BDR | 0.381 | 3.047 | 0.005 | 0.321 | Significant |
| H6 | TR ≥ BDR | 0.208 | 3.580 | 0.010 | 1.092 | Significant |
| H7 | GITP ≥ BDR | 0.312 | 3.415 | 0.021 | 0.321 | Significant |
| H8 | GLAI ≥ BDR | 0.235 | 3.983 | 0.048 | 0.024 | Significant |
| H9 | BDR ≥ ITABD | 0.412 | 4.574 | 0.000 | 2.164 | Significant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghaleb, E.A.A.; Dominic, P.D.D.; Fati, S.M.; Muneer, A.; Ali, R.F. The Assessment of Big Data Adoption Readiness with a Technology–Organization–Environment Framework: A Perspective towards Healthcare Employees. Sustainability 2021, 13, 8379. https://0-doi-org.brum.beds.ac.uk/10.3390/su13158379
Ghaleb EAA, Dominic PDD, Fati SM, Muneer A, Ali RF. The Assessment of Big Data Adoption Readiness with a Technology–Organization–Environment Framework: A Perspective towards Healthcare Employees. Sustainability. 2021; 13(15):8379. https://0-doi-org.brum.beds.ac.uk/10.3390/su13158379
Chicago/Turabian StyleGhaleb, Ebrahim A. A., P. D. D. Dominic, Suliman Mohamed Fati, Amgad Muneer, and Rao Faizan Ali. 2021. "The Assessment of Big Data Adoption Readiness with a Technology–Organization–Environment Framework: A Perspective towards Healthcare Employees" Sustainability 13, no. 15: 8379. https://0-doi-org.brum.beds.ac.uk/10.3390/su13158379