
The Self-Reported Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) and PainDETECT Questionnaires in COVID-19 Survivors with Post-COVID Pain

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Neuropathic Pain Assessment
2.3. Sensitization-Associated Symptoms
2.4. Psychological Variables
2.5. Cognitive Variables
2.6. Health-Related Quality of Life
2.7. Sample Size Determination
2.8. Statistical Analysis
3. Results
3.1. Clinical Data of the Sample
3.2. Bivariate Correlation Analysis
3.3. Multiple Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of Post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Int. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Navarro-Santana, M.; Plaza-Manzano, G.; Palacios-Ceña Arendt-Nielsen, L. Time course prevalence of Post-COVID pain symptoms of musculoskeletal origin in patients who had survived to SARS-CoV-2 infection: A systematic review and meta-analysis. Pain 2022, 163, 1220–1231. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; de-la-Llave-Rincón, A.I.; Ortega-Santiago, R.; Ambite-Quesada, S.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Hernández-Barrera, V.; Martín-Guerrero, J.D.; Pellicer-Valero, O.J.; et al. Prevalence and risk factors of musculoskeletal pain symptoms as long-term post-COVID sequelae in hospitalized COVID-19 survivors: A multicenter study. Pain 2021. [Google Scholar] [CrossRef]
- Attal, N.; Martinez, V.; Bouhassira, D. Potential for increased prevalence of neuropathic pain after the COVID-19 pandemic. Pain Rep. 2021, 6, e884. [Google Scholar] [CrossRef]
- Bakılan, F.; Gökmen, İ.G.; Ortanca, B.; Uçan, A.; Eker Güvenç, Ş.; Şahin Mutlu, F.; Gökmen, H.M.; Ekim, A. Musculoskeletal symptoms and related factors in postacute COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14734. [Google Scholar] [CrossRef]
- Karaarslan, F.; Demircioğlu, G.F.; Kardeş, S. Postdischarge rheumatic and musculoskeletal symptoms following hospitalization for COVID-19: Prospective follow-up by phone interviews. Rheumatol. Int. 2021, 41, 1263–1271. [Google Scholar] [CrossRef]
- Soares, F.H.C.; Kubota, G.T.; Fernandes, A.M.; Hojo, B.; Couras, C.; Costa, B.V.; Lapa, J.D.D.S.; Braga, L.M.; Almeida, M.M.; Cunha, P.H.M.D.; et al. “Pain in the Pandemic Initiative Collaborators”. Prevalence and characteristics of new-onset pain in COVID-19 survivours, a controlled study. Eur. J. Pain 2021, 25, 1342–1354. [Google Scholar] [CrossRef]
- Bileviciute-Ljungar, I.; Norrefalk, J.R.; Borg, K. Pain burden in post-COVID-19 syndrome following mild COVID-19 infection. J. Clin. Med. 2022, 11, 771. [Google Scholar] [CrossRef]
- Oguz-Akarsu, E.; Gullu, G.; Kilic, E.; Dinç, Y.; Ursavas, A.; Yilmaz, E.; Zarifoglu, M.; Karli, N.; Pandemic Study Team. Insight into pain syndromes in acute phase of mild-to-moderate COVID-19: Frequency, clinical characteristics, and associated factors. Eur. J. Pain 2021, 26, 492–504. [Google Scholar] [CrossRef]
- Herrero-Montes, M.; Fernández-de-las-Peñas, C.; Ferrer-Pargada, D.; Tello-Mena, S.; Cancela-Cilleruelo, I.; Rodríguez-Jiménez, J.; Palacios-Ceña, D.; Parás-Bravo, P. Prevalence of neuropathic component in post-COVID pain symptoms in previously hospitalized COVID-19 survivors. Int. J. Clin. Pract. 2022, 2022, 3532917. [Google Scholar] [CrossRef] [PubMed]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central sensitisation in chronic pain conditions: Latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Shraim, M.A.; Massé-Alarie, H.; Hodges, P.W. Methods to discriminate between mechanism-based categories of pain experienced in the musculoskeletal system: A systematic review. Pain 2021, 162, 1007–1037. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef]
- Bennett, M.I.; Smith, B.H.; Torrance, N.; Potter, J. The S-LANSS score for identifying pain of predominantly neuropathic origin: Validation for use in clinical and postal research. J. Pain 2005, 6, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef]
- Gauffin, J.; Hankama, T.; Kautiainen, H.; Hannonen, P.; Haanpää, M. Neuropathic pain and use of PainDETECT in patients with fibromyalgia: A cohort study. BMC Neurol. 2013, 13, 21. [Google Scholar] [CrossRef] [Green Version]
- Gavrilova, N.; Soprun, L.; Lukashenko, M.; Ryabkova, V.; Fedotkina, T.V.; Churilov, L.P.; Shoenfeld, Y. New clinical phenotype of the Post-COVID syndrome: Fibromyalgia and joint hypermobility condition. Pathophysiology 2022, 29, 24–29. [Google Scholar] [CrossRef]
- Úbeda-D’Ocasar, E.; Valera-Calero, J.A.; Gallego-Sendarrubias, G.M.; Fernández-de-Las-Peñas, C.; Arias-Buría, J.L.; Morales-Cabezas, M.; Arendt-Nielsen, L.; Cigarán-Méndez, M. Association of neuropathic pain symptoms with sensitization related symptomatology in women with fibromyalgia. Biomedicines 2022, 10, 612. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012, 12, 276–285. [Google Scholar] [CrossRef] [Green Version]
- Neblett, R.; Cohen, H.; Choi, Y.; Hartzell, M.M.; Williams, M.; Mayer, T.G.; Gatchel, R.J. The Central Sensitization Inventory (CSI): Establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J. Pain 2013, 14, 438–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta-Vargas, A.I.; Neblett, R.; Chiarotto, A.; Kregel, J.; Nijs, J.; van Wilgen, C.P.; Pitance, L.; Knezevic, A.; Gatchel, R.J.; Mayer, T.G.; et al. Dimensionality and reliability of the Central Sensitization Inventory in a pooled multi-country sample. J. Pain 2018, 19, 317–329. [Google Scholar] [CrossRef] [Green Version]
- Herrmann-Lingen, C.; Buss, U.; Snaith, R.P. Hospital Anxiety and Depression Scale–Deutsche Version (HADS-D); Verlag Hans Huber: Bern, Switzerland, 2011. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Woby, S.R.; Roach, N.K.; Urmston, M.; Watson, P.J. Psychometric properties of the TSK-11: A shortened version of the Tampa Scale for Kinesiophobia. Pain 2005, 117, 137–144. [Google Scholar] [CrossRef]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Van Hout, B.; Janssen, M.F.; Feng, Y.J.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C.; Steyerberg, E.W. The number of subjects per variable required in linear regression analyses. J. Clin. Epidemiol. 2015, 68, 627–636. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.G.; Quintana-Ascencio, P.F. A solution to minimum sample size for regressions. PLoS ONE 2020, 15, e0229345. [Google Scholar]
- Bouhassira, D.; Lantéri-Minet, M.; Attal, N.; Laurent, B.; Touboul, C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008, 136, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Moreton, B.J.; Tew, V.; das Nair, R.; Wheeler, M.; Walsh, D.A.; Lincoln, N.B. Pain phenotype in patients with knee osteoarthritis: Classification and measurement properties of painDETECT and self-report Leeds assessment of neuropathic symptoms and signs scale in a cross-sectional study. Arthritis Care Res. 2015, 67, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Felix, E.R.; Gater, D.R., Jr. Interrelationship of neurogenic obesity and chronic neuropathic pain in persons with spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2021, 27, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Cattadori, G.; Di Marco, S.; Baravelli, M.; Picozzi, A.; Ambrosio, G. Exercise training in post-COVID-19 patients: The need for a multifactorial protocol for a multifactorial pathophysiology. J. Clin. Med. 2022, 11, 2228. [Google Scholar] [CrossRef] [PubMed]
- Tampin, B.; Royle, J.; Bharat, C.; Trevenen, M.; Olsen, L.; Goucke, R. Psychological factors can cause false pain classification on PainDETECT. Scand. J. Pain 2019, 19, 501–512. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Kuner, R.; Jensen, T.S. Neuropathic pain: From Mechanisms to treatment. Physiol. Rev. 2021, 101, 259–301. [Google Scholar] [CrossRef] [PubMed]
- van Wilgen, C.P.; Vuijk, P.J.; Kregel, J.; Voogt, L.; Meeus, M.; Descheemaeker, F.; Keizer, D.; Nijs, J. Psychological distress and widespread pain contribute to the variance of the Central Sensitization Inventory: A cross-sectional study in patients with chronic pain. Pain Pract. 2018, 18, 239–246. [Google Scholar] [CrossRef]
- Kregel, J.; Schumacher, C.; Dolphens, M.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M.; Coppieters, I. Convergent validity of the Dutch Central Sensitization Inventory: Associations with psychophysical pain measures, quality of life, disability, and pain cognitions in patients with chronic spinal pain. Pain Pract. 2018, 18, 777–787. [Google Scholar] [CrossRef]
- Adams, G.R.; Gandhi, W.; Harrison, R.; van Reekum, C.M.; Gilron, I.; Salomons, T.V. Do “central sensitization” questionnaires reflect measures of nociceptive sensitization or psychological constructs? Protocol for a systematic review. Pain Rep. 2021, 6, e962. [Google Scholar] [CrossRef]
- Bouhassira, D.; Branders, S.; Attal, N.; Fernandes, A.M.; Demolle, D.; Barbour, J.; Ciampi de Andrade, D.; Pereira, A. Stratification of patients based on the Neuropathic Pain Symptom Inventory: Development and validation of a new algorithm. Pain 2021, 162, 1038–1046. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Variable | Sample (n = 146) | Males (n = 67) | Females (n = 78) |
|---|---|---|---|
| Demographic Characteristics | |||
| Age (years) | 57.5 ± 11.8 | 60.0 ± 10.3 | 55.2 ± 12.5 |
| Height (m) | 1.67 ± 0.09 | 1.73 ± 0.08 | 1.61 ± 0.06 |
| Weight (kg) | 81.8 ± 17.1 | 86.5 ± 15.6 | 77.8 ± 17.4 |
| Clinical Characteristics | |||
| Pain intensity (NPRS, 0–10) | 5.6 ± 1.7 | 5.2 ± 1.85 | 5.9 ± 1.55 |
| Post-COVID symptoms (months) | 18.8 ± 1.8 | 18.7 ± 2.0 | 18.9 ± 1.7 |
| Sensory-Related Features | |||
| PainDETECT (0–38) | 6.8 ± 6.1 | 5.5 ± 5.5 | 7.9 ± 6.45 |
| S-LANSS (0–24) | 6.9 ± 6.1 | 6.45 ± 5.9 | 7.2 ± 6.25 |
| Central Sensitization Inventory (0–100) | 33.9 ± 17.25 | 25.9 ± 14.3 | 41.05 ± 16.45 |
| Quality of Life | |||
| EuroQol 5-D Questionnaire (0–1) | 0.75 ± 0.2 | 0.8 ± 0.2 | 0.75 ± 0.2 |
| Psychological Characteristics | |||
| HADS-A (0–21) | 5.3 ± 4.2 | 4.45 ± 4.05 | 6.1 ± 4.2 |
| HADS-D (0–21) | 5.1 ± 4.3 | 4.4 ± 4.3 | 5.6 ± 4.3 |
| Pittsburgh Sleeping Quality Index (0–21) | 8.1 ± 4.3 | 6.85 ± 4.4 | 9.1 ± 3.9 |
| Pain Catastrophizing Scale (0–52) | 12.15 ± 11.95 | 10.3 ± 11.3 | 13.8 ± 12.4 |
| Tampa Scale for Kinesiophobia (0–44) | 24.1 ± 8.55 | 22.5 ± 8.75 | 25.5 ± 8.25 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | ||||||||||||||
| 2. Gender | −0.206 * | |||||||||||||
| 3. Height | n.s. | −0.595 ** | ||||||||||||
| 4. Weight | n.s. | −0.256 ** | 0.509 ** | |||||||||||
| 5. Post-COVID Symptoms | n.s. | n.s. | n.s. | n.s. | ||||||||||
| 6. Pain intensity | n.s. | 0.200 * | −0.191 * | n.s. | n.s. | |||||||||
| 7. HADS-A | n.s. | 0.194 * | n.s. | n.s. | −0.271 ** | 0.175 * | ||||||||
| 8. HADS-D | n.s. | n.s. | n.s. | n.s. | n.s. | 0.225 ** | 0.750 ** | |||||||
| 9. PSQI | n.s. | 0.262 ** | −0.213 ** | n.s. | −0.189 * | n.s. | 0.316 ** | 0.354 ** | ||||||
| 10. PAINDetect | n.s. | 0.193 * | −0.254 ** | n.s. | n.s. | 0.198 * | 0.169 * | n.s. | n.s. | |||||
| 11. S-LANSS | n.s. | n.s. | n.s. | 0.193 * | n.s. | 0.212 * | 0.213 ** | 0.169 * | n.s. | 0.671 ** | ||||
| 12. CSI | n.s. | 0.440 ** | −0.285 ** | n.s. | n.s. | 0.190 * | 0.551 ** | 0.446 ** | 0.390 ** | 0.413 ** | 0.274 ** | |||
| 13. PCS | n.s. | n.s. | n.s. | n.s. | −0.343 ** | n.s. | 0.492 ** | 0.483 ** | 0.282 ** | 0.220 ** | 0.263 ** | 0.402 ** | ||
| 14. TSK-11 | n.s. | 0.168 * | n.s. | n.s. | n.s. | n.s. | 0.356 ** | 0.306 ** | 0.288 ** | 0.283 * | 0.303 ** | 0.450 ** | 0.578 ** | |
| 15. EuroQol 5-D | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. | n.s. | −0.174 * | −0.301 ** | n.s. | n.s. | −0.199 * | −0.210 * | n.s. |
| Predictor Outcome | Β | SE B | 95% CI | B | t | p | |
|---|---|---|---|---|---|---|---|
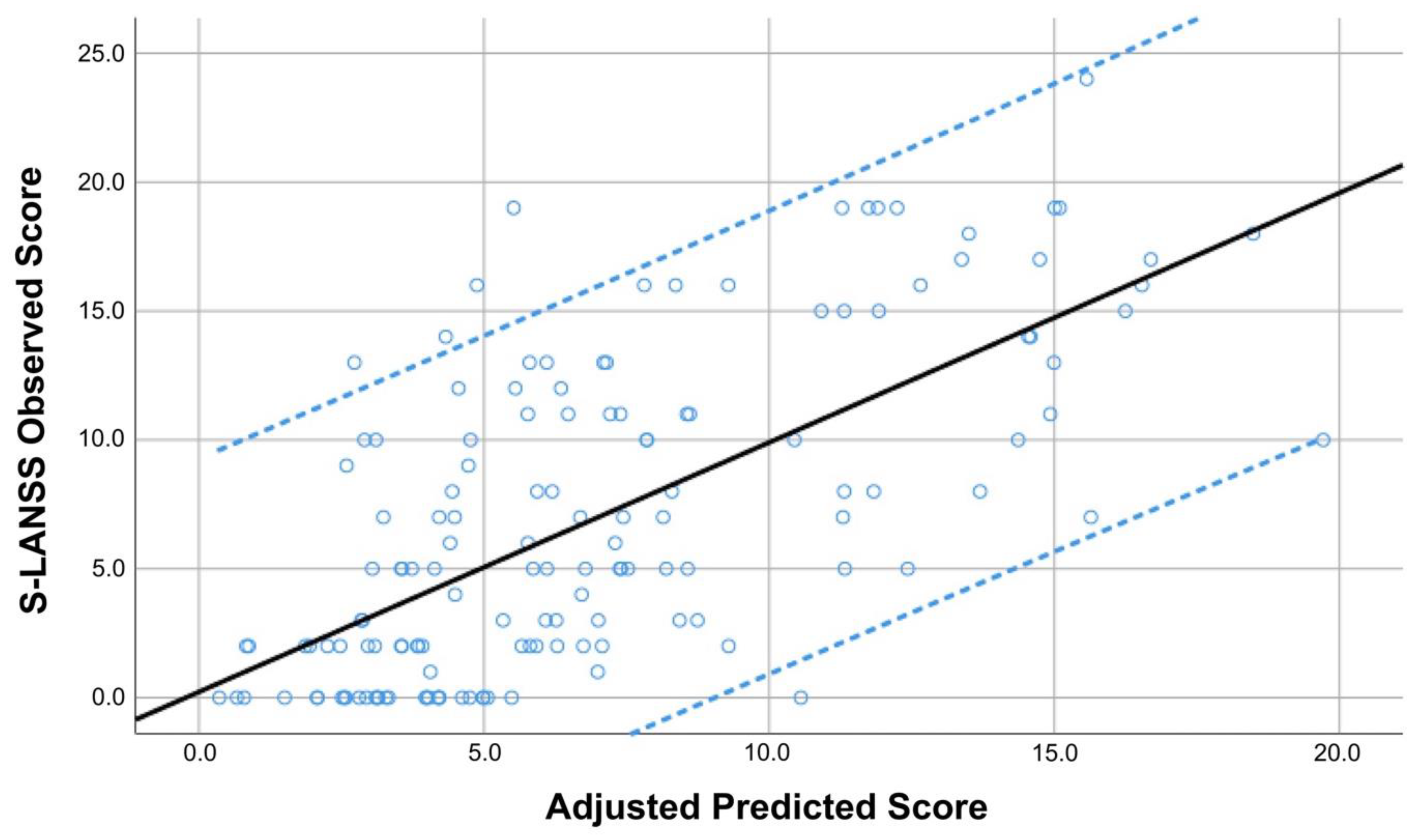
| S-LANSS | Step 1 PainDETECT | 0.670 | 0.062 | 0.548; 0.792 | 0.671 | 10.860 | <0.001 |
| Step 2 PainDETECT Post-COVID Duration | 0.666 −0.467 | 0.061 0.203 | 0.545; 0.786 −0.867; −0.066 | 0.667 −0.140 | 10.950 −2.305 | <0.001 0.023 | |
| Step 3 PainDETECT Post-COVID Duration Weight | 0.667 −0.518 0.044 | 0.060 0.202 0.022 | 0.548; 0.786 −0.918; −0.119 0.001; 0.087 | 0.669 −0.156 0.122 | 11.092 −2.564 2.006 | <0.001 0.011 0.047 |
| Predictor Outcome | Β | SE B | 95% CI | B | t | p | |
|---|---|---|---|---|---|---|---|
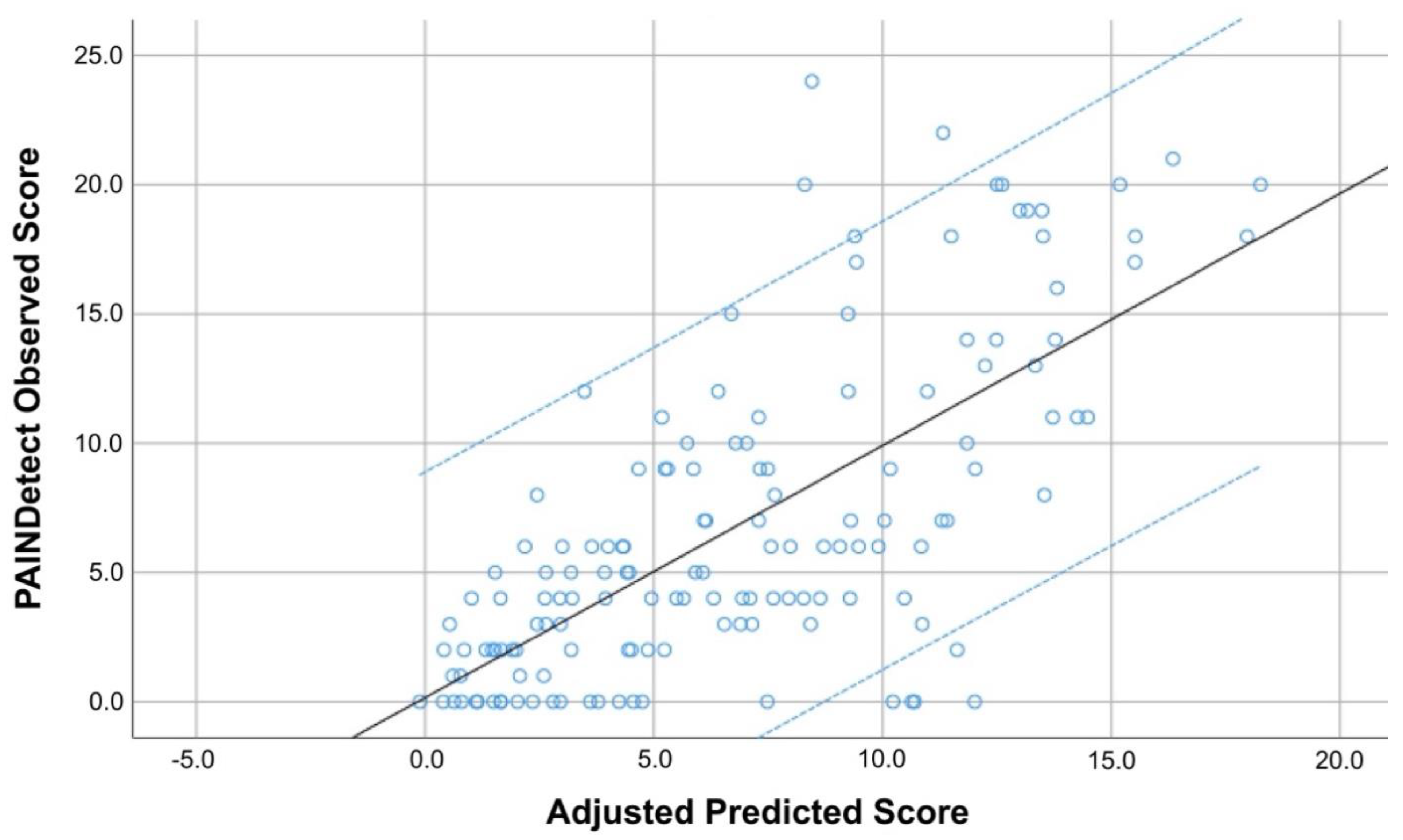
| PainDETECT | Step 1 S-LANSS | 0.672 | 0.062 | 0.550; 0.795 | 0.671 | 10.860 | <0.001 |
| Step 2 S-LANSS CSI | 0.604 0.088 | 0.061 0.022 | 0.483; 0.725 0.045; 0.130 | 0.603 0.247 | 9.876 4.042 | <0.001 <0.001 | |
| Step 3 S-LANSS CSI HADS-A | 0.614 0.116 –0.215 | 0.061 0.025 0.101 | 0.494; 0.734 0.066; 0.165 −0.415; −0.015 | 0.613 0.326 −0.148 | 10.129 4.596 −2.120 | <0.001 <0.001 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-de-las-Peñas, C.; Valera-Calero, J.A.; Herrero-Montes, M.; del-Valle-Loarte, P.; Rodríguez-Rosado, R.; Ferrer-Pargada, D.; Arendt-Nielsen, L.; Parás-Bravo, P. The Self-Reported Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) and PainDETECT Questionnaires in COVID-19 Survivors with Post-COVID Pain. Viruses 2022, 14, 1486. https://0-doi-org.brum.beds.ac.uk/10.3390/v14071486
Fernández-de-las-Peñas C, Valera-Calero JA, Herrero-Montes M, del-Valle-Loarte P, Rodríguez-Rosado R, Ferrer-Pargada D, Arendt-Nielsen L, Parás-Bravo P. The Self-Reported Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) and PainDETECT Questionnaires in COVID-19 Survivors with Post-COVID Pain. Viruses. 2022; 14(7):1486. https://0-doi-org.brum.beds.ac.uk/10.3390/v14071486
Chicago/Turabian StyleFernández-de-las-Peñas, César, Juan Antonio Valera-Calero, Manuel Herrero-Montes, Pablo del-Valle-Loarte, Rafael Rodríguez-Rosado, Diego Ferrer-Pargada, Lars Arendt-Nielsen, and Paula Parás-Bravo. 2022. "The Self-Reported Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) and PainDETECT Questionnaires in COVID-19 Survivors with Post-COVID Pain" Viruses 14, no. 7: 1486. https://0-doi-org.brum.beds.ac.uk/10.3390/v14071486