Impact of Weight Loss on the Total Antioxidant/Oxidant Potential in Patients with Morbid Obesity—A Longitudinal Study



Abstract
:1. Introduction
2. Materials and Methods
3. Blood Collection
4. Laboratory Measurements
5. Redox Assays
5.1. Total Antioxidant Capacity (TAC)
5.2. Total Oxidant Status (TOS)
5.3. Oxidative Stress Index (OSI)
5.4. Radical-Scavenging Activity Assay (DPPH)
5.5. Ferric-Reducing Antioxidant Power (FRAP)
6. Statistical Analysis
7. Results
7.1. Clinical and Laboratory Parameters
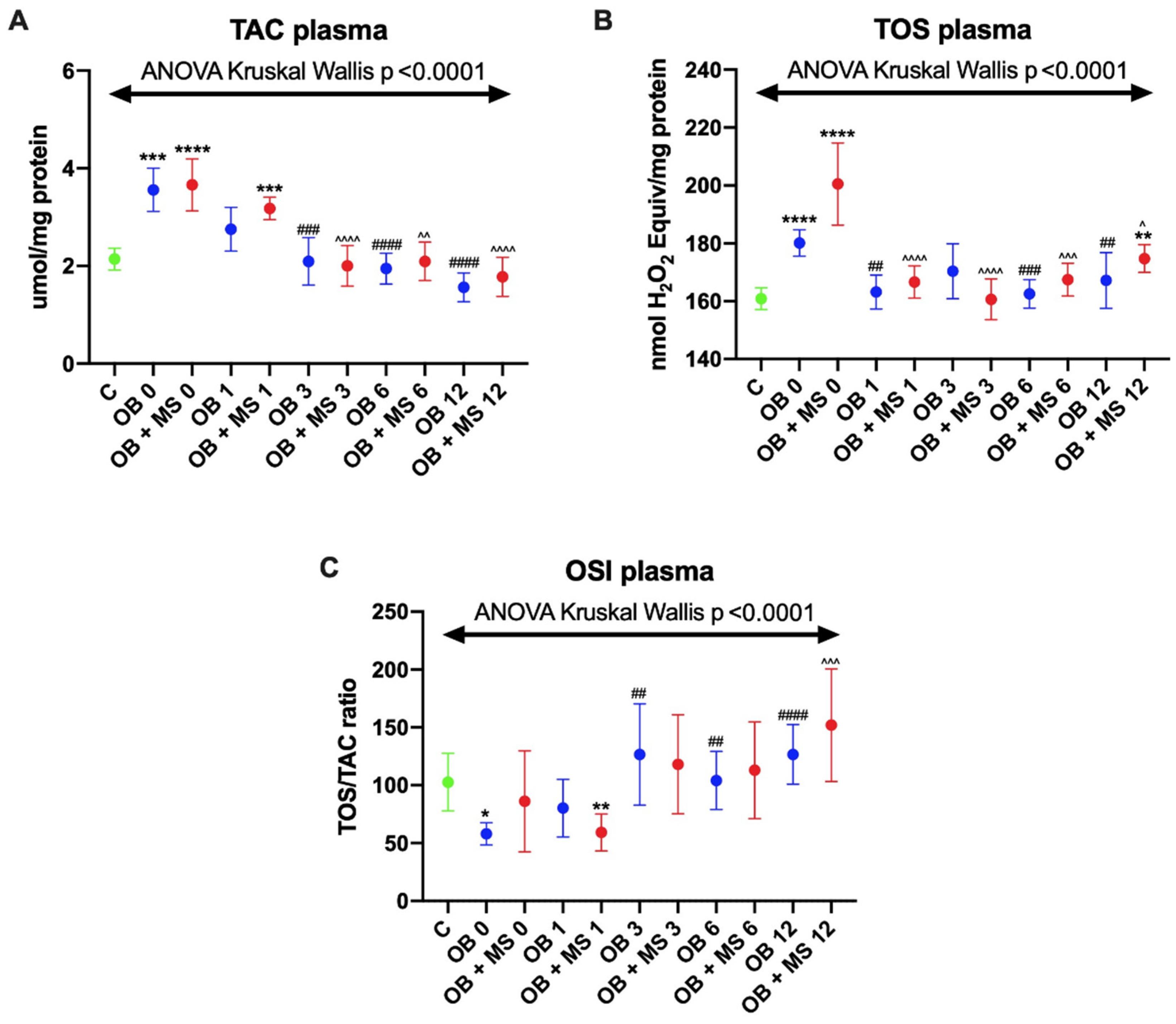
7.2. Total Antioxidant Capacity (TAC)
7.3. Total Oxidant Status (TOS)
7.4. Oxidative Stress Index (OSI)
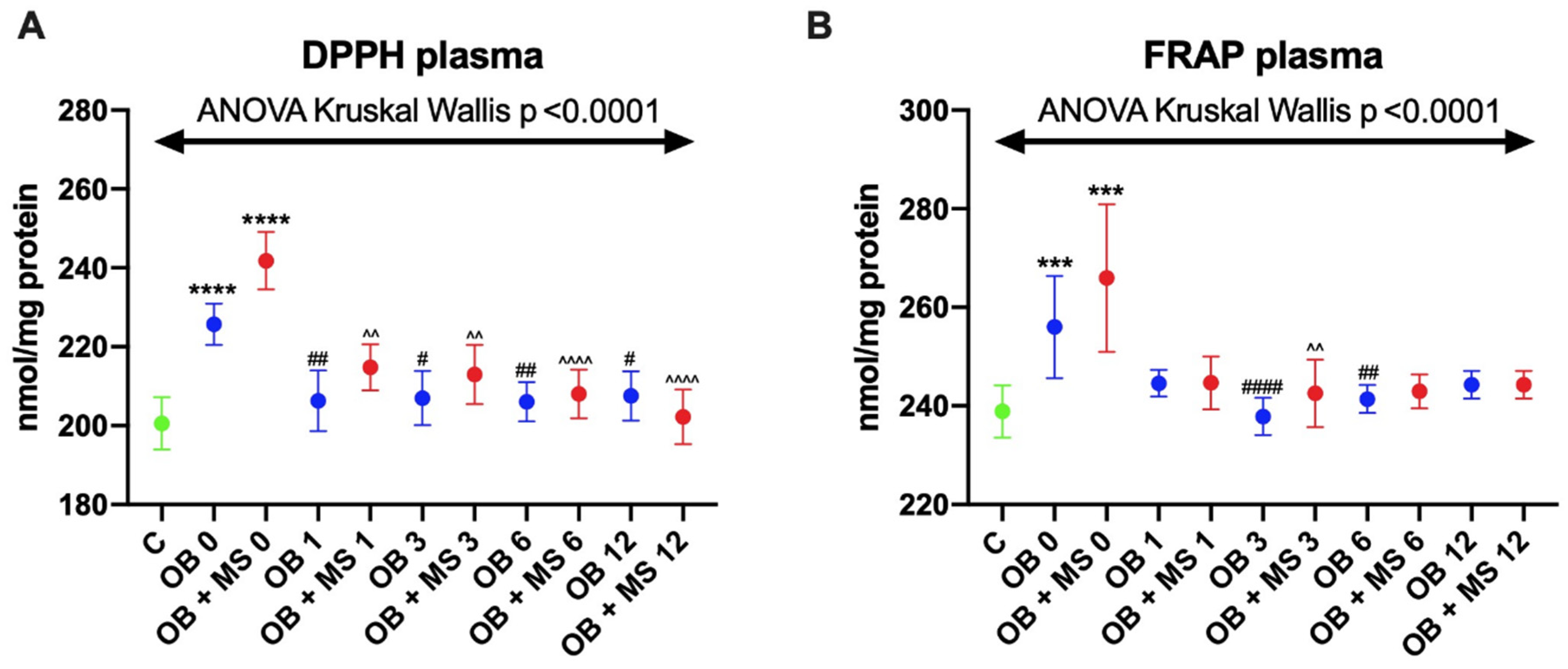
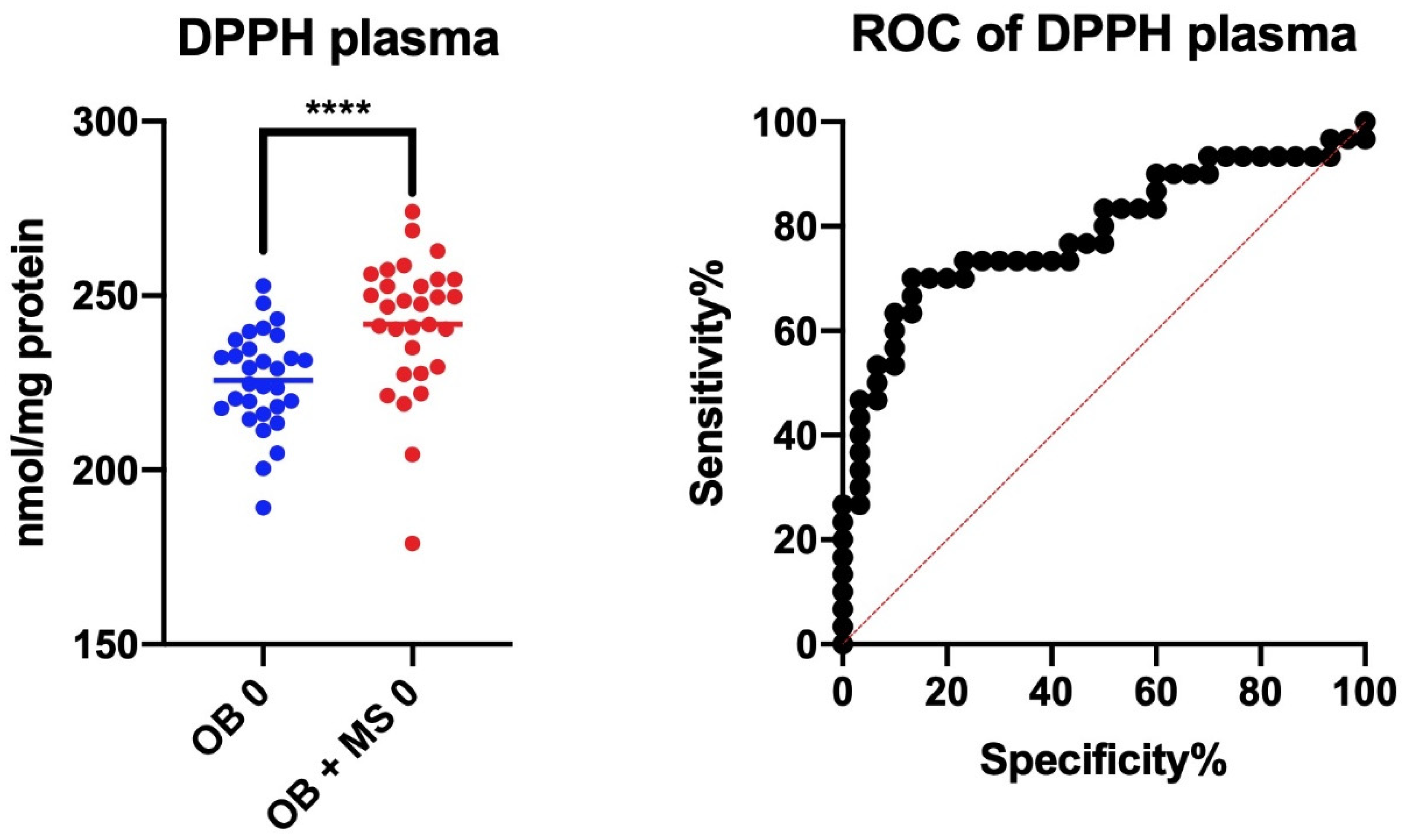
7.5. 2,2′-Diphenyl-1-Picrylhydrazyl Radical (DPPH) Assay
7.6. Ferric-Reducing Antioxidant Power (FRAP)
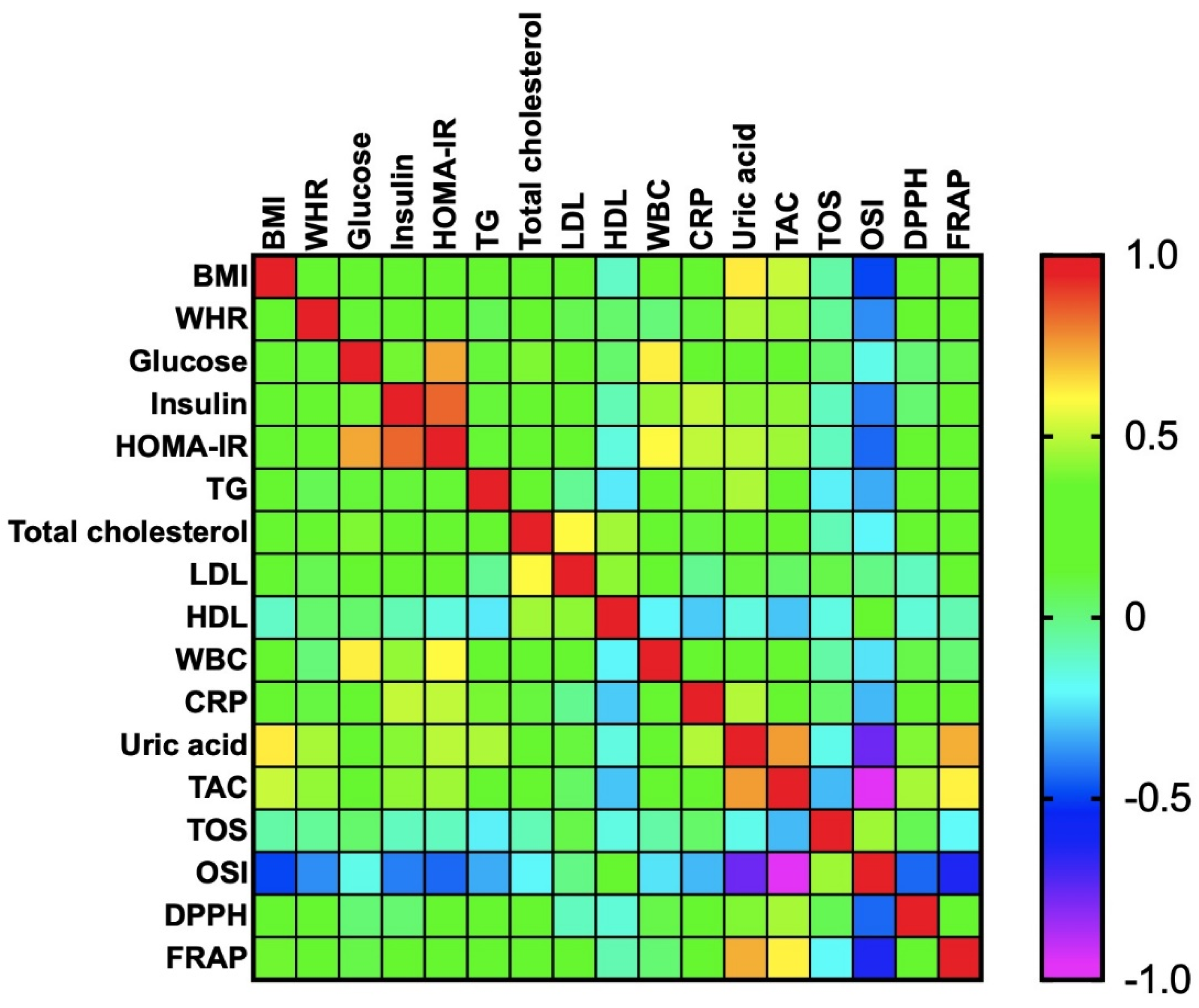
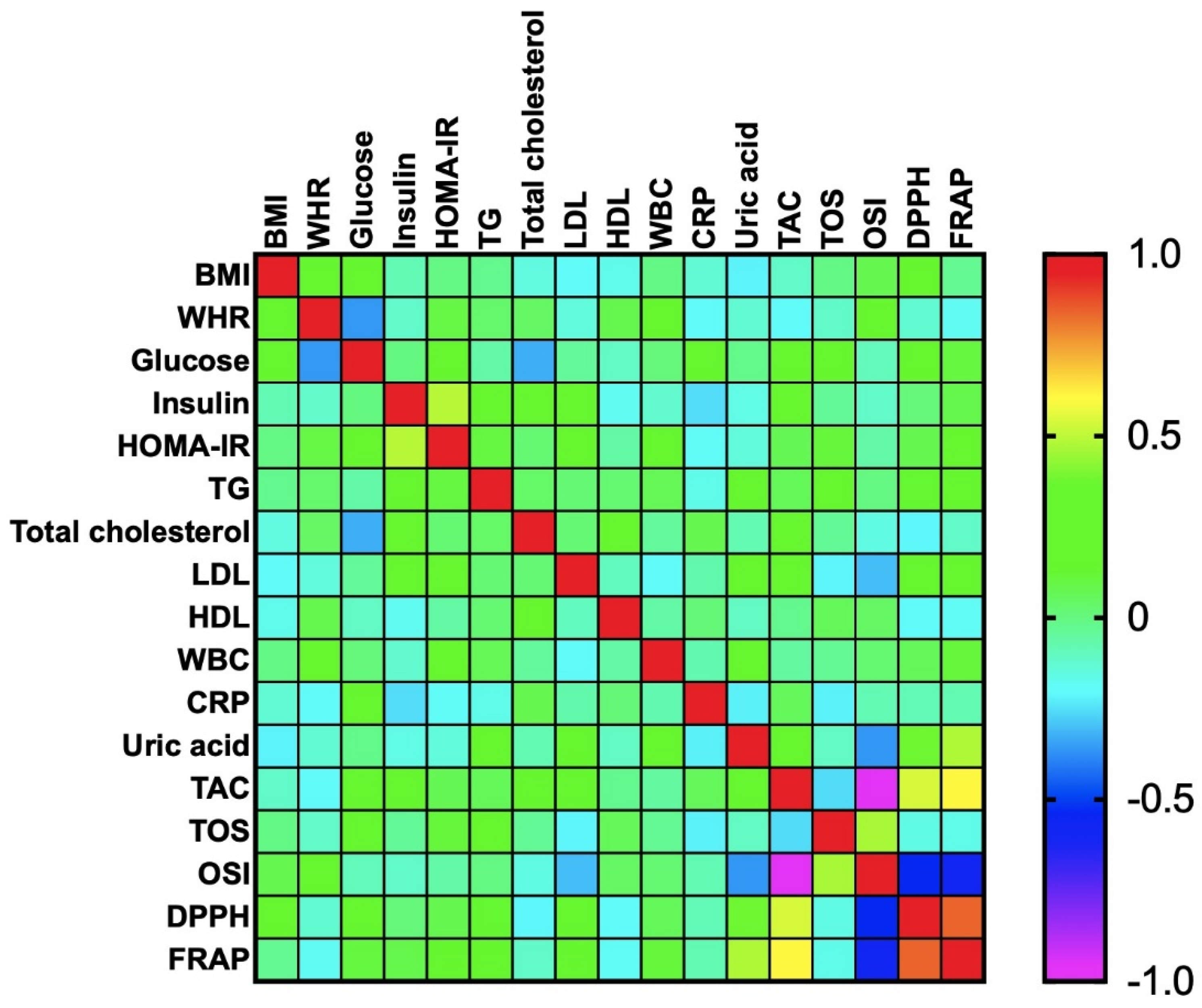
7.7. Correlations
7.8. ROC Analysis
8. Discussion
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Andò, S.; Gelsomino, L.; Panza, S.; Giordano, C.; Bonofiglio, D.; Barone, I.; Catalano, S. Obesity, leptin and breast cancer: Epidemiological evidence and proposed mechanisms. Cancers (Basel) 2019, 11, 62. [Google Scholar] [CrossRef] [Green Version]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Formisano, G.; Buchwald, H.; Scopinaro, N. Bariatric Surgery Worldwide 2013. Obes. Surg. 2015, 25, 1822–1832. [Google Scholar] [CrossRef]
- Murri, M.; García-Fuentes, E.; García-Almeida, J.M.; Garrido-Sánchez, L.; Mayas, M.D.; Bernal, R.; Tinahones, F.J. Changes in oxidative stress and insulin resistance in morbidly obese patients after bariatric surgery. Obes. Surg. 2010, 20, 363–368. [Google Scholar] [CrossRef]
- Li, S.; Tan, H.Y.; Wang, N.; Zhang, Z.J.; Lao, L.; Wong, C.W.; Feng, Y. The role of oxidative stress and antioxidants in liver diseases. Int. J. Mol. Sci. 2015, 16, 26087–26124. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, M.R.; Fasano, R.; Paolisso, G. Adiponectin and Cognitive Decline. Int. J. Mol. Sci. 2020, 21, 2010. [Google Scholar] [CrossRef] [Green Version]
- Sharma, R.S.; Harrison, D.J.; Kisielewski, D.; Cassidy, D.M.; McNeilly, A.D.; Gallagher, J.R.; Walsh, S.V.; Honda, T.; McCrimmon, R.J.; Dinkova-Kostova, A.T.; et al. Experimental Nonalcoholic Steatohepatitis and Liver Fibrosis Are Ameliorated by Pharmacologic Activation of Nrf2 (NF-E2 p45-Related Factor 2). CMGH 2018, 5, 367–398. [Google Scholar] [CrossRef] [Green Version]
- Wing, R.R.; Bolin, P.; Brancati, F.L.; Bray, G.A.; Clark, J.M.; Coday, M.; Crow, R.S.; Curtis, J.M.; Egan, C.M.; Espeland, M.A.; et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N. Engl. J. Med. 2013, 369, 145–154. [Google Scholar]
- Cornejo-Pareja, I.; Clemente-Postigo, M.; Tinahones, F.J. Metabolic and Endocrine Consequences of Bariatric Surgery. Front. Endocrinol. (Lausanne) 2019, 10, 626. [Google Scholar] [CrossRef] [Green Version]
- Sudlow, A.; le Roux, C.; Pournaras, D. The metabolic benefits of different bariatric operations: What procedure to choose? Endocr. Connect. 2020, 9, R28–R35. [Google Scholar] [CrossRef] [Green Version]
- Daigle, C.R.; Brethauer, S.A.; Tu, C.; Petrick, A.T.; Morton, J.M.; Schauer, P.R.; Aminian, A. Which postoperative complications matter most after bariatric surgery? Prioritizing quality improvement efforts to improve national outcomes. Surg. Obes. Relat. Dis. 2018, 14, 652–657. [Google Scholar] [CrossRef]
- Adil, M.T.; Jain, V.; Rashid, F.; Al-taan, O.; Whitelaw, D.; Jambulingam, P. Meta-analysis of the effect of bariatric surgery on physical function. Br. J. Surg. 2018, 105, 1107–1118. [Google Scholar] [CrossRef]
- Salminen, P.; Helmio, M.; Ovaska, J.; Juuti, A.; Leivonen, M.; Peromaa-Haavisto, P.; Hurme, S.; Soinio, M.; Nuutila, P.; Victorzon, M. Effect of laparoscopic sleeve gastrectomy vs laparoscopic roux-en-y gastric bypass onweight loss at 5 years among patients with morbid obesity the SLEEVEPASS randomized clinical trial. JAMA J. Am. Med. Assoc. 2018, 319, 241–254. [Google Scholar] [CrossRef]
- Peterli, R.; Wolnerhanssen, B.K.; Peters, T.; Vetter, D.; Kroll, D.; Borbely, Y.; Schultes, B.; Beglinger, C.; Drewe, J.; Schiesser, M.; et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic roux-en-y gastric bypass onweight loss in patients with morbid obesity the sm-boss randomized clinical trial. JAMA J. Am. Med. Assoc. 2018, 319, 255–265. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Zalewska, A.; Gerreth, K. Salivary Redox Biomarkers in Selected Neurodegenerative Diseases. J. Clin. Med. 2020, 9, 497. [Google Scholar] [CrossRef] [Green Version]
- Klimiuk, A.; Zalewska, A.; Sawicki, R.; Knapp, M.; Maciejczyk, M. Salivary Oxidative Stress Increases With the Progression of Chronic Heart Failure. J. Clin. Med. 2020, 9, 769. [Google Scholar] [CrossRef] [Green Version]
- Świderska, M.; Maciejczyk, M.; Zalewska, A.; Pogorzelska, J.; Flisiak, R.; Chabowski, A. Oxidative stress biomarkers in the serum and plasma of patients with non-alcoholic fatty liver disease (NAFLD). Can plasma AGE be a marker of NAFLD? Free Radic. Res. 2019, 53, 841–850. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Taranta-Janusz, K.; Wasilewska, A.; Kossakowska, A.; Zalewska, A. A Case-Control Study of Salivary Redox Homeostasis in Hypertensive Children. Can Salivary Uric Acid be a Marker of Hypertension? J. Clin. Med. 2020, 9, 837. [Google Scholar] [CrossRef] [Green Version]
- Zińczuk, J.; Maciejczyk, M.; Zaręba, K.; Romaniuk, W.; Markowski, A.; Kędra, B.; Zalewska, A.; Pryczynicz, A.; Matowicka-Karna, J.; Guzińska-Ustymowicz, K. Antioxidant Barrier, Redox Status, and Oxidative Damage to Biomolecules in Patients with Colorectal Cancer. Can Malondialdehyde and Catalase Be Markers of Colorectal Cancer Advancement? Biomolecules 2019, 9, 637. [Google Scholar] [CrossRef] [Green Version]
- Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Dadan, J.; Myśliwiec, H.; Choromańska, K.; Zalewska, A.; Maciejczyk, M. A Longitudinal Study of the Antioxidant Barrier and Oxidative Stress in Morbidly Obese Patients after Bariatric Surgery. Does the Metabolic Syndrome Affect the Redox Homeostasis of Obese People? J. Clin. Med. 2020, 9, 976. [Google Scholar] [CrossRef] [Green Version]
- Knaś, M.; Maciejczyk, M.; Sawicka, K.; Hady, H.R.; Niczyporuk, M.; Ładny, J.R.; Matczuk, J.; Waszkiel, D.; Żendzian-Piotrowska, M.; Zalewska, A. Impact of morbid obesity and bariatric surgery on antioxidant/oxidant balance of the unstimulated and stimulated human saliva. J. Oral Pathol. Med. 2016, 45, 455–464. [Google Scholar] [CrossRef]
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. IDF Commun. 2006, 1–23. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Heropolitanska-Pliszka, E.; Pietrucha, B.; Sawicka-Powierza, J.; Bernatowska, E.; Wolska-Kusnierz, B.; Pac, M.; Car, H.; Zalewska, A.; Mikoluc, B. Antioxidant Defense, Redox Homeostasis, and Oxidative Damage in Children With Ataxia Telangiectasia and Nijmegen Breakage Syndrome. Front. Immunol. 2019, 10, 2322. [Google Scholar] [CrossRef]
- Janaszewska, A.; Bartosz, G. Assay of total antioxidant capacity: Comparison of four methods as applied to human blood plasma. Scand. J. Clin. Lab. Invest. 2002, 62, 231–236. [Google Scholar] [CrossRef]
- Benzie, I.F.F.; Strain, J.J. The Ferric Reducing Ability of Plasma (FRAP) as a Measure of “Antioxidant Power”: The FRAP Assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef] [Green Version]
- Choromańska, B.; Myśliwiec, P.; Razak Hady, H.; Dadan, J.; Myśliwiec, H.; Chabowski, A.; Mikłosz, A. Metabolic Syndrome is Associated with Ceramide Accumulation in Visceral Adipose Tissue of Women with Morbid Obesity. Obesity 2019, 27, 444–453. [Google Scholar] [CrossRef] [Green Version]
- Grzegorczyk, E.A.; Harasim-Symbor, E.; Lukaszuk, B.; Harasiuk, D.; Choromanska, B.; Mysliwiec, P.; Zendzian-Piotrowska, M.; Chabowski, A. Lack of pronounced changes in the expression of fatty acid handling proteins in adipose tissue and plasma of morbidly obese humans. Nutr. Diabetes 2018, 8, 3. [Google Scholar] [CrossRef]
- Yazıcı, D.; Sezer, H. Insulin resistance, obesity and lipotoxicity. In Advances in Experimental Medicine and Biology; Springer: Berlin, Germany, 2017; Volume 960, pp. 277–304. [Google Scholar]
- Molnár, D.; Decsi, T.; Koletzko, B. Reduced antioxidant status in obese children with multimetabolic syndrome. Int. J. Obes. 2004, 28, 1197–1202. [Google Scholar] [CrossRef] [Green Version]
- Zalewska, A.; Kossakowska, A.; Taranta-Janusz, K.; Zięba, S.; Fejfer, K.; Salamonowicz, M.; Kostecka-Sochoń, P.; Wasilewska, A.; Maciejczyk, M. Dysfunction of Salivary Glands, Disturbances in Salivary Antioxidants and Increased Oxidative Damage in Saliva of Overweight and Obese Adolescents. J. Clin. Med. 2020, 9, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Schaft, N.; Schoufour, J.D.; Nano, J.; Kiefte-de Jong, J.C.; Muka, T.; Sijbrands, E.J.G.; Ikram, M.A.; Franco, O.H.; Voortman, T. Dietary antioxidant capacity and risk of type 2 diabetes mellitus, prediabetes and insulin resistance: The Rotterdam Study. Eur. J. Epidemiol. 2019, 34, 853–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Moreno, C. Methods Used to Evaluate the Free Radical Scavenging Activity in Foods and Biological Systems. Food Sci. Technol. Int. 2002, 8, 121–137. [Google Scholar] [CrossRef]
- Arnao, M.B. Some methodological problems in the determination of antioxidant activity using chromogen radicals: A practical case. Trends Food Sci. Technol. 2000, 11, 419–421. [Google Scholar] [CrossRef]
- Lushchak, V.I. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Biol. Interact. 2014, 224, 164–175. [Google Scholar] [CrossRef]
- Fejfer, K.; Buczko, P.; Niczyporuk, M.; Ładny, J.R.; Hady, H.R.; Knaś, M.; Waszkiel, D.; Klimiuk, A.; Zalewska, A.; Maciejczyk, M. Oxidative Modification of Biomolecules in the Nonstimulated and Stimulated Saliva of Patients with Morbid Obesity Treated with Bariatric Surgery. BioMed Res. Int. 2017, 2017, 4923769. [Google Scholar] [CrossRef] [Green Version]
- Bitencourt, M.R.; Patias, L.D.; Beck, M.; Alvarez, G.D.C.; Diehl, L.N.; Duarte, M.F.; Schetinger, M.R.; Morsch, V.M. Evaluation of the biochemical, inflammatory and oxidative profile of obese patients given clinical treatment and bariatric surgery. Clin. Chim. Acta 2017, 465, 72–79. [Google Scholar]
- Vlassara, H.; Cai, W.; Tripp, E.; Pyzik, R.; Yee, K.; Goldberg, L.; Tansman, L.; Chen, X.; Mani, V.; Fayad, Z.A.; et al. Oral AGE restriction ameliorates insulin resistance in obese individuals with the metabolic syndrome: A randomised controlled trial. Diabetologia 2016, 59, 2182–2192. [Google Scholar] [CrossRef]
- Sautin, Y.Y.; Johnson, R.J. Uric Acid: The Oxidant-Antioxidant Paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Wang, L.; Xie, R.; Dai, W.; Gao, C.; Shen, P.; Huang, X.; Zhang, F.; Yang, X.; Ji, G. Association of serum uric acid with body mass index: A cross-sectional study from Jiangsu province, China. Iran. J. Public Health 2014, 43, 1503–1509. [Google Scholar]
- Chaudhary, K.; Malhotra, K.; Sowers, J.; Aroor, A. Uric acid-key ingredient in the recipe for cardiorenal metabolic syndrome. CardioRenal Med. 2013, 3, 208–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfar, S.; Boussoffara, R.; Sfar, M.T.; Kerkeni, A. Antioxidant enzymes activities in obese Tunisian children. Nutr. J. 2013, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Skalicky, J.; Muzakova, V.; Kandar, R.; Meloun, M.; Rousar, T.; Palicka, V. Evaluation of oxidative stress and inflammation in obese adults with metabolic syndrome. Clin. Chem. Lab. Med. 2008, 46, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Goutzourelas, N.; Orfanou, M.; Charizanis, I.; Leon, G.; Spandidos, D.A.; Kouretas, D. Gsh levels affect weight loss in individuals with metabolic syndrome and obesity following dietary therapy. Exp. Ther. Med. 2018, 16, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghamohammadi, V.; Sajjadi, S.F.; Jarrahi, F.; Abdollahi, A.; Mirzaei, K. The Association Between Total Antioxidant Capacity and Resting Metabolic Rate (RMR)/Respiratory Quotient (RQ) in Overweight and Obese Woman. Diabetes Metab. Syndr. 2019, 13, 2763–2767. [Google Scholar] [CrossRef]
- Peluso, I.; Raguzzini, A. Salivary and Urinary Total Antioxidant Capacity as Biomarkers of Oxidative Stress in Humans. Patholog. Res. Int. 2016, 2016, 5480267. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Szulimowska, J.; Taranta-Janusz, K.; Werbel, K.; Wasilewska, A.; Zalewska, A. Salivary FRAP as A Marker of Chronic Kidney Disease Progression in Children. Antioxidants 2019, 8, 490. [Google Scholar] [CrossRef] [Green Version]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Fejfer, K.; Krahel, J.; Flisiak, I.; Kołodziej, U.; Zalewska, A. Salivary Antioxidants and Oxidative Stress in Psoriatic Patients: Can Salivary Total Oxidant Status and Oxidative Status Index Be a Plaque Psoriasis Biomarker? Oxid. Med. Cell. Longev. 2020, 2020, 9086024. [Google Scholar] [CrossRef] [Green Version]
- Klimiuk, A.; Maciejczyk, M.; Choromańska, M.; Fejfer, K.; Waszkiewicz, N.; Zalewska, A. Salivary Redox Biomarkers in Different Stages of Dementia Severity. J. Clin. Med. 2019, 8, 840. [Google Scholar] [CrossRef] [Green Version]
- Kusano, C.; Ferrari, B. Total antioxidant capacity: A biomarker in biomedical and nutritional studies. J. Cell Mol. Biol. 2008, 7, 1–15. [Google Scholar]
- Maciejczyk, M.; Zalewska, A.; Ładny, J.R. Salivary Antioxidant Barrier, Redox Status, and Oxidative Damage to Proteins and Lipids in Healthy Children, Adults, and the Elderly. Oxid. Med. Cell. Longev. 2019, 2019, 4393460. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | C | OB 0 | OB+MS 0 | OB 1 | OB+MS 1 | OB 3 | OB+MS 3 | OB 6 | OB+MS 6 | OB 12 | OB+MS 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 45 (28–56) | 39 (31–52) | 48 (28–56) | ||||||||
| BMI (kg/m2) | 23 (17–25) | 45 * (40–55) | 47 * (41–61) | 41 * (30–49) | 42 * (33–57) | 37 * # (28–47) | 39 * (29–50) | 33 * # (25–42) | 34 * ^ (26–48) | 29 # (23–38) | 31 * ^ (23–40) |
| WHR | 0.71 (0.65–0.75) | 0.96 * (0.81–1) | 0.98 * (0.84–1.2) | 0.96 * (0.74–1) | 0.99 * (0.87–1.2) | 0.94 * (0.8–1) | 0.98 * (0.83–1.1) | 0.93 * (0.81–0.98) | 0.96 * (0.87–1.1) | 0.91 * (0.8–0.98) | 0.93 * ^ (0.85–0.99) |
| Glucose (mg/dL) | 78 (57–98) | 98 * (76–122) | 106 * (89–264) | 93 * (69–115) | 99 * (75–147) | 88 (60–142) | 98 * (79–116) | 85 (68–109) | 96 * (81–157) | 84 # (73–111) | 90 * ^ (77–99) |
| Insulin (μIU/mL) | 7.6 (6.4–9.7) | 18 * (12–39) | 22 * (9.3–41) | 11 * # (4–22) | 15 * (5.8–35) | 7.8 # (2.7–16) | 11 * ^ (3.6–22) | 8.7 # (4.1–12) | 8.8 ^ (4.5–17) | 7.8 # (3–15) | 8.5 ^ (4.5–9.9) |
| HOMA–IR | 1.4 (1.2–2.1) | 4.2 * (2.6–9.3) | 5.8 * (3.1–15) | 2.7 * # (0.73–5.6) | 3.8 * (1.3–8.6) | 1.9 # (0.46–3.1) | 2.5 * ^ (0.95–4.4) | 1.8 # (0.76–2.9) | 2 * ^ (1.1–3.8) | 1.7 # (0.59–3.5) | 1.9 ^ (1.1–2.2) |
| Cholesterol (mg/dL) | 175 (158–194) | 195 * (147–231) | 211 * (167–268) | 176 (124–210) | 192 * (126–235) | 176 (120–217) | 181 ^ (120–237) | 178 (114–245) | 188 * (148–264) | 176 (114–231) | 174 ^ (138–295) |
| LDL (mg/dL) | 118 (111–123) | 125 (102–159) | 144 * (122–181) | 109 (83–153) | 122 ^ (66–183) | 109 (69–159) | 116 ^ (50–189) | 109 (61–166) | 110 ^ (83–157) | 111 # (59–134) | 102 * ^ (64–164) |
| TG (mg/dL) | 135 (119–150) | 127 (62–197) | 150 (104–289) | 108 * (66–209) | 136 (75–367) | 102 * (46–182) | 137 (78–240) | 92 * (48–182) | 130 (89–214) | 90 * # (36–182) | 102 * ^ (59–146) |
| HDL (mg/dL) | 60 (45–70) | 48 * (33–62) | 46 * (31–72) | 44 * (30–106) | 45 * (31–68) | 47 * (27–141) | 49 * (35–69) | 50 * (35–72) | 53 (35–86) | 53 * (38–81) | 56 ^ (43–70) |
| ALT (IU/L) | 24 (8–35) | 25 (6–93) | 27 (12–54) | 25 (6–52) | 28 (14–56) | 20 (6–43) | 24 (13–59) | 17 (6–51) | 21 (12–31) | 18 (8–37) | 19 (8–43) |
| AST (IU/L) | 24 (16–36) | 19 (13–44) | 21 (14–50) | 22 (14–98) | 27 (14–85) | 19 (12–36) | 21 (13–43) | 17 (9–48) | 20 (12–43) | 18 (12–52) | 19 (12–37) |
| CRP (mg/L) | 5.6 (4.7–6.5) | 9.1 * (1.5–28) | 12 * (5.3–18) | 5.6 (0.5–26) | 8.4 * (1.5–14) | 6.1 (0.3–17) | 7.1 (0.6–17) | 5.1 (0.3–20) | 6.1 ^ (0.5–11) | 4.9 # (0.2–7.8) | 5.5 ^ (1.2–16) |
| Uric acid (mg/dL) | 4 (2.3–6.4) | 6 * (4.3–13) | 7.1 * (4.6–13) | 5.2 * (3.7–11) | 6.1 * (3.8–9.5) | 4.9 # (3–8.5) | 5.4 * (3.4–8.2) | 4.5 # (2.4–6.4) | 5 * ^ (3.9–7.1) | 4.2 # (2.3–5.7) | 4.5 ^ (3.3–6.3) |
| Urea (mg/dL) | 24 (17–41) | 28 (18–38) | 29 * (18–60) | 24 # (7–34) | 27 (20–47) | 22 # (7–45) | 26 (17–41) | 22 (9–43) | 26 (19–51) | 22 (11–47) | 25 (18–55) |
| WBC (103/μL) | 7.4 (4.4–9.7) | 8.3 * (6.1–12) | 9.5 * (5.9–13) | 6.6 (4.6–9.6) | 7.2 (5–13) | 5.8 (4.6–11) | 6.9 (3.9–12) | 6 (4.8–9.3) | 7.2 (4.4–11) | 5.9 (4.1–8.5) | 7 (4.2–10) |
| RBC (106/μL) | 4.7 (3.9–5.3) | 4.6 (3.5–5.8) | 4.6 (4–5.5) | 4.8 (4.1–6) | 4.8 (4.3–6) | 4.6 (4.1–5.1) | 4.8 (4.1–5.5) | 4.6 (4–5.7) | 4.8 (4–5.7) | 4.6 (4.2–5.4) | 4.5 (3.3–5.7) |
| HGB (g/dL) | 14 (12–16) | 13 (11–15) | 13 (12–16) | 13 (10–16) | 14 (11–17) | 13 (12–16) | 13 (11–16) | 13 (10–15) | 13 (11–16) | 14 (9–16) | 14 (9–16) |
| PLT (103/μL) | 289 (259–315) | 262 (141–417) | 258 (183–418) | 261 (121–412) | 229 * (128–405) | 266 (130–312) | 247 * (131–345) | 292 (188–425) | 252 (167–375) | 201 * (130–345) | 224 * (164–378) |
| Parameter | Area | 95% Confidence Interval | p-Value | Cut Off | Sensitivity (%) | 95% CI | Specificity (%) | 95% CI |
|---|---|---|---|---|---|---|---|---|
| TAC | 0.53 | 0.3851 to 0.6816 | 0.657 | >3.529 | 56.67 | 39.20% to 72.62% | 53.33 | 36.14% to 69.77% |
| TOS | 0.74 | 0.6158 to 0.8647 | 0.002 | >184.8 | 66.67 | 48.78% to 80.77% | 62.07 | 44.00% to 77.31% |
| OSI | 0.54 | 0.3871 to 0.6865 | 0.628 | >52.96 | 60 | 42.32% to 75.41% | 55.17 | 37.55% to 71.59% |
| DPPH | 0.79 | 0.6669 to 0.9064 | <0.0001 | >234.9 | 73.33 | 55.55% to 85.82% | 76.67 | 59.07% to 88.21% |
| FRAP | 0.53 | 0.3855 to 0.6834 | 0.647 | >251.6 | 56.67 | 39.20% to 72.62% | 53.33 | 36.14% to 69.77% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choromańska, B.; Myśliwiec, P.; Łuba, M.; Wojskowicz, P.; Myśliwiec, H.; Choromańska, K.; Żendzian-Piotrowska, M.; Dadan, J.; Zalewska, A.; Maciejczyk, M. Impact of Weight Loss on the Total Antioxidant/Oxidant Potential in Patients with Morbid Obesity—A Longitudinal Study. Antioxidants 2020, 9, 376. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9050376
Choromańska B, Myśliwiec P, Łuba M, Wojskowicz P, Myśliwiec H, Choromańska K, Żendzian-Piotrowska M, Dadan J, Zalewska A, Maciejczyk M. Impact of Weight Loss on the Total Antioxidant/Oxidant Potential in Patients with Morbid Obesity—A Longitudinal Study. Antioxidants. 2020; 9(5):376. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9050376
Chicago/Turabian StyleChoromańska, Barbara, Piotr Myśliwiec, Magdalena Łuba, Piotr Wojskowicz, Hanna Myśliwiec, Katarzyna Choromańska, Małgorzata Żendzian-Piotrowska, Jacek Dadan, Anna Zalewska, and Mateusz Maciejczyk. 2020. "Impact of Weight Loss on the Total Antioxidant/Oxidant Potential in Patients with Morbid Obesity—A Longitudinal Study" Antioxidants 9, no. 5: 376. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox9050376