A Case-Control Study of Salivary Redox Homeostasis in Hypertensive Children. Can Salivary Uric Acid be a Marker of Hypertension?

 ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Issues
2.2. Patients
2.3. Saliva Collection
2.4. Dental Examination
2.5. Blood Collection
2.6. Total Protein Assay
2.7. Redox Assays
2.8. Enzymatic and Non-Enzymatic Antioxidants
2.9. Redox Status
2.10. Oxidative Stress Products
2.11. Nitrosative Stress Products
2.12. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Salivary Gland Function and Dental Examination
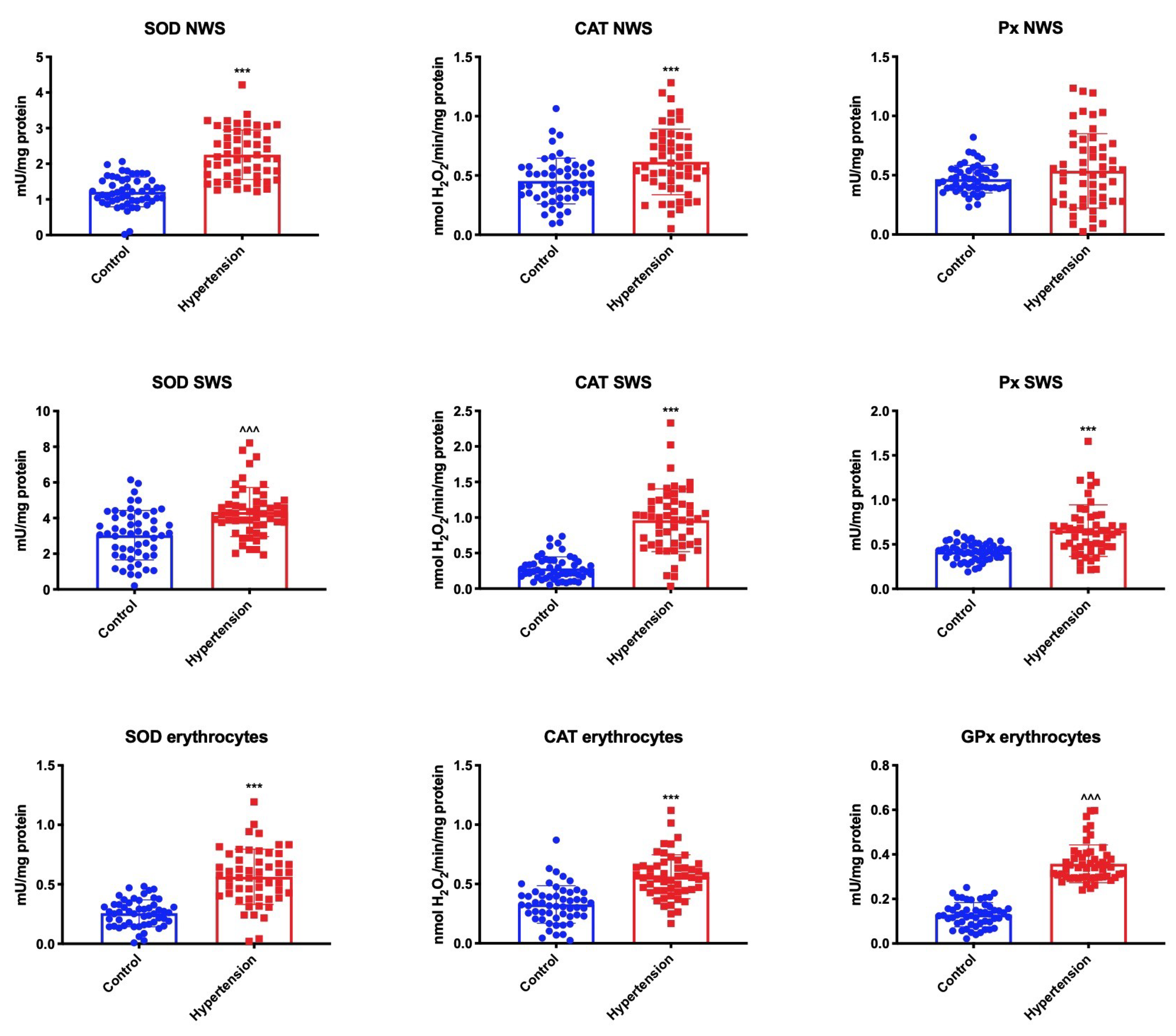
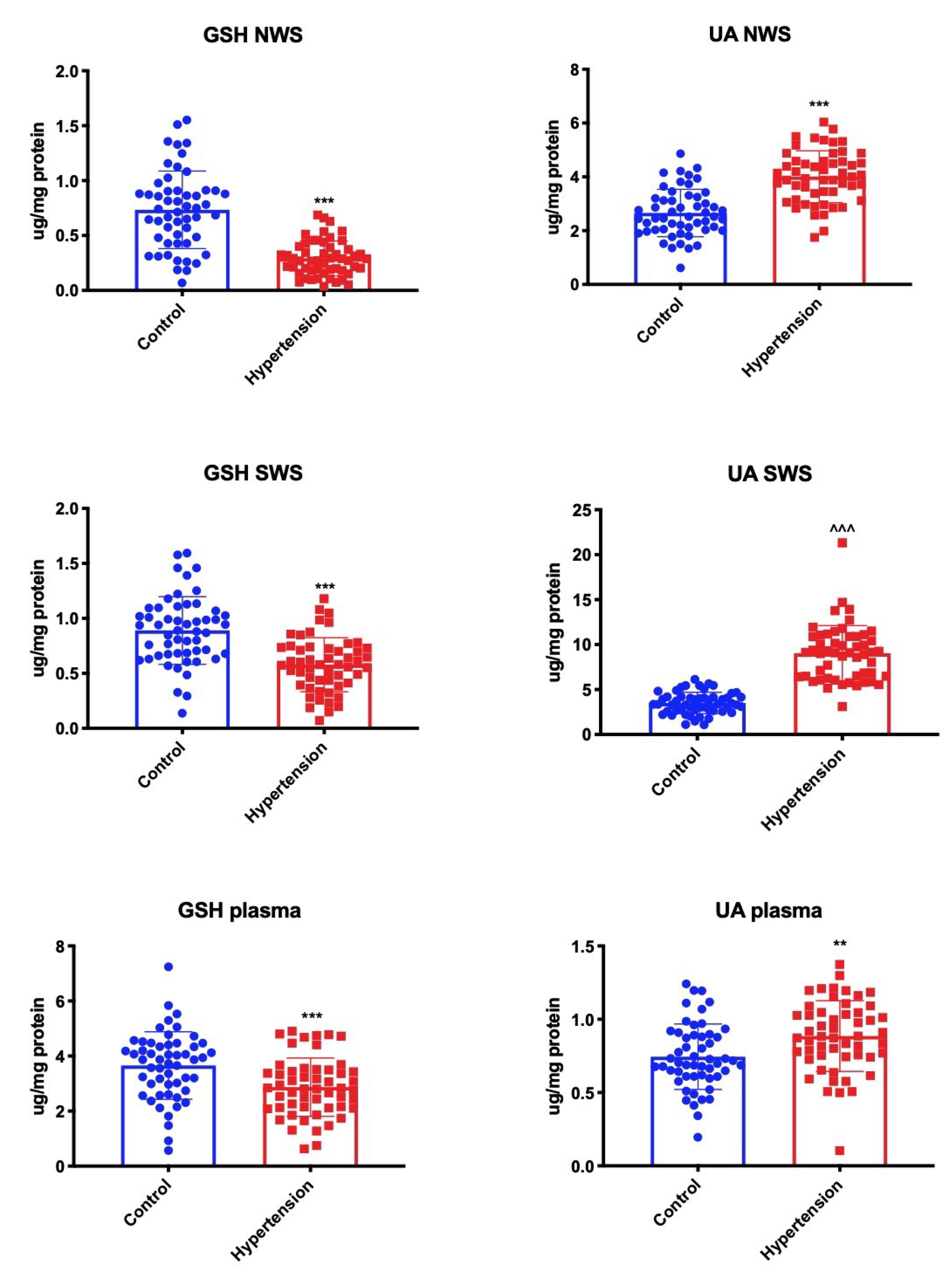
3.3. Enzymatic and Non-Enzymatic Antioxidants
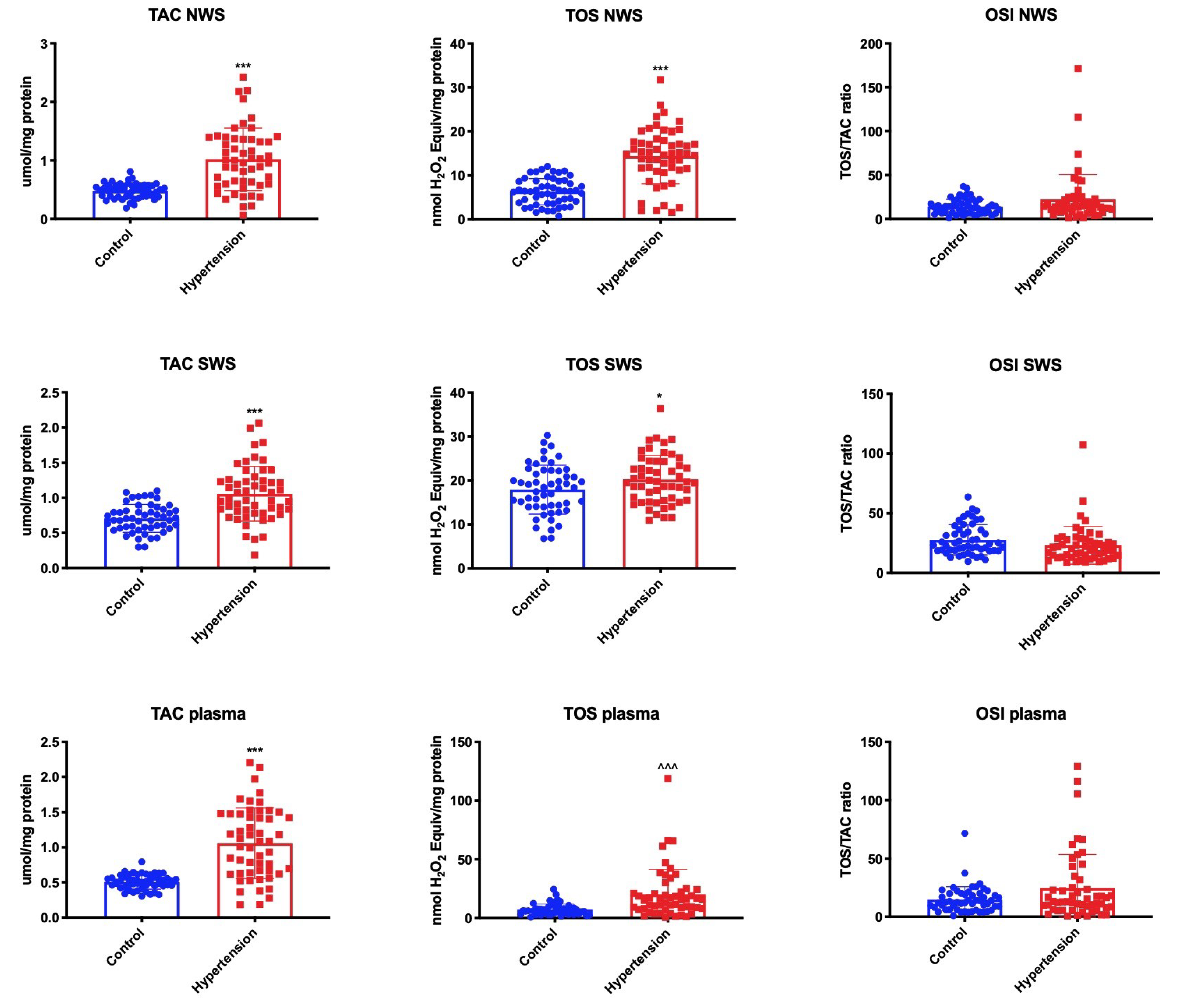
3.4. Redox Status
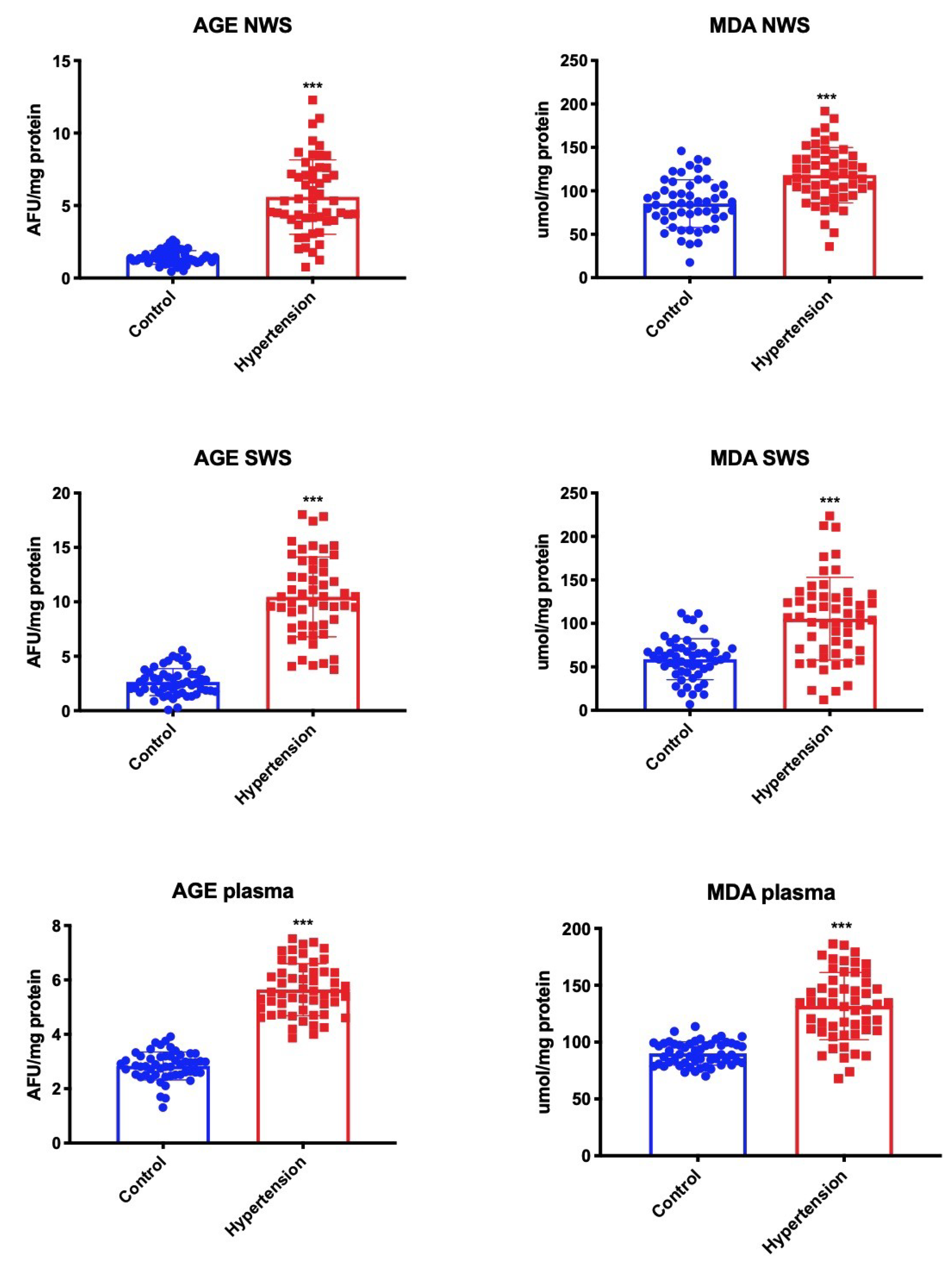
3.5. Oxidative Stress Products
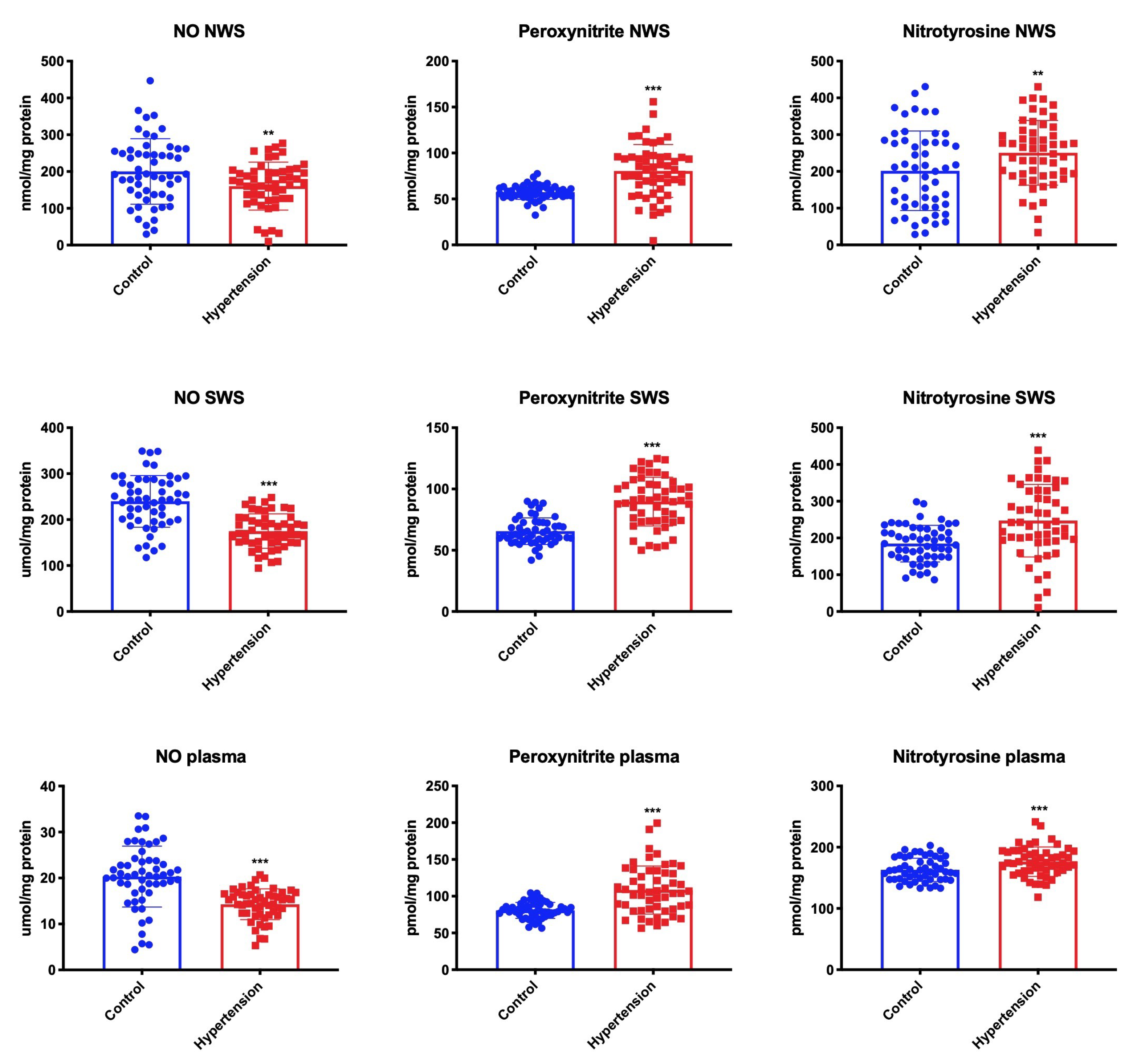
3.6. Nitrosative Stress
3.7. Correlations
3.8. ROC Analysis
4. Discussion
5. Conclusions
- Childhood hypertension is associated with disturbances in enzymatic and non-enzymatic antioxidant defense as well as enhanced oxidative and nitrosative damage both in the plasma/erythrocytes as well as salivary glands (NWS and SWS).
- In hypertension, the secretion of stimulated saliva decreases. Children with hypertension should receive additional dental care.
- Salivary UA may be a potential biomarker of hypertension in children. However, further studies are necessary to assess its diagnostic utility in a larger group of patients.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Poulter, N.R.; Prabhakaran, D.; Caulfield, M. Hypertension. Lancet 2015, 386, 801–812. [Google Scholar] [CrossRef]
- Falkner, B. Hypertension in children and adolescents: Epidemiology and natural history. Pediatr. Nephrol. 2010, 25, 1219–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matossian, D. Pediatric hypertension. Pediatr. Ann. 2018, 47, e499–e503. [Google Scholar] [CrossRef] [PubMed]
- Rao, G. Diagnosis, Epidemiology, and Management of Hypertension in Children. Pediatrics 2016, 138, e20153616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Q & As on Hypertension. Available online: https://www.who.int/features/qa/82/en (accessed on 20 February 2020).
- Dinh, Q.N.; Drummond, G.R.; Sobey, C.G.; Chrissobolis, S. Roles of Inflammation, Oxidative Stress, and Vascular Dysfunction in Hypertension. BioMed Res. Int. 2014, 2014, 406960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, E.; Gori, T.; Münzel, T. Oxidative stress and endothelial dysfunction in hypertension. Hypertens. Res. 2011, 34, 665–673. [Google Scholar] [CrossRef]
- Rodrigo, R.; González, J.; Paoletto, F. The role of oxidative stress in the pathophysiology of hypertension. Hypertens. Res. 2011, 34, 431–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsiropoulou, S.; Dulak-Lis, M.; Montezano, A.C.; Touyz, R.M. Biomarkers of Oxidative Stress in Human Hypertension. In Hypertension and Cardiovascular Disease; Andreadis, E.A., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 151–170. ISBN 978-3-319-39599-9. [Google Scholar]
- Lytvyn, Y.; Perkins, B.A.; Cherney, D.Z.I. Uric Acid as a Biomarker and A Therapeutic Target in Diabetes. Can. J. Diabetes 2015, 39, 239–246. [Google Scholar] [CrossRef]
- Fini, M.A.; Elias, A.; Johnson, R.J.; Wright, R.M. Contribution of uric acid to cancer risk, recurrence, and mortality. Clin. Transl. Med. 2012. [Google Scholar] [CrossRef] [Green Version]
- Tothova, L.; Kamodyova, N.; Cervenka, T.; Celec, P. Salivary markers of oxidative stress in oral diseases. Front. Cell. Infect. Microbiol. 2015, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T.W. Salivary biomarkers: Toward future clinical and diagnostic utilities. Clin. Microbiol. Rev. 2013, 26, 781–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kułak-Bejda, A.; Waszkiewicz, N.; Bejda, G.; Zalewska, A.; Maciejczyk, M. Diagnostic Value of Salivary Markers in Neuropsychiatric Disorders. Dis. Markers 2019, 2019, 4360612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Zalewska, A. Salivary Redox Biomarkers in Selected Neurodegenerative Diseases. J. Clin. Med. 2020, 9, 497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Szulimowska, J.; Taranta-Janusz, K.; Werbel, K.; Wasilewska, A.; Zalewska, A. Salivary FRAP as A Marker of Chronic Kidney Disease Progression in Children. Antioxidants 2019, 8, 409. [Google Scholar] [CrossRef] [Green Version]
- Gheena, S.; Chandrasekhar, T.; Ramani, P. Salivary characteristics of diabetic children. Braz. J. Oral Sci. 2011, 10, 93–97. [Google Scholar] [CrossRef]
- Salamonowicz, M.; Zalewska, A.; Maciejczyk, M. Oral consequences of obesity and metabolic syndrome in children and adolescents. Dent. Med. Probl. 2019, 56, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Zalewska, A.; Kossakowska, A.; Taranta-Janusz, K.; Zięba, S.; Fejfer, K.; Salamonowicz, M.; Kostecka-Sochoń, P.; Wasilewska, A.; Maciejczyk, M. Dysfunction of Salivary Glands, Disturbances in Salivary Antioxidants and Increased Oxidative Damage in Saliva of Overweight and Obese Adolescents. J. Clin. Med. 2020, 9, 548. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Szulimowska, J.; Skutnik, A.; Taranta-Janusz, K.; Wasilewska, A.; Wiśniewska, N.; Zalewska, A. Salivary Biomarkers of Oxidative Stress in Children with Chronic Kidney Disease. J. Clin. Med. 2018, 7, 209. [Google Scholar] [CrossRef] [Green Version]
- Zalewska, A.; Maciejczyk, M.; Szulimowska, J.; Imierska, M.; Błachnio-Zabielska, A. High-Fat Diet Affects Ceramide Content, Disturbs Mitochondrial Redox Balance, and Induces Apoptosis in the Submandibular Glands of Mice. Biomolecules 2019, 9, 877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Skutnik-Radziszewska, A.; Zieniewska, I.; Matczuk, J.; Domel, E.; Waszkiel, D.; Żendzian-Piotrowska, M.; Szarmach, I.; Zalewska, A. Antioxidant Defense, Oxidative Modification, and Salivary Gland Function in an Early Phase of Cerulein Pancreatitis. Oxid. Med. Cell. Longev. 2019, 2019, 8403578. [Google Scholar] [CrossRef] [PubMed]
- Maciejczyk, M.; Matczuk, J.; Żendzian-Piotrowska, M.; Niklińska, W.; Fejfer, K.; Szarmach, I.; Ładny, J.R.; Zieniewska, I.; Zalewska, A. Eight-Week Consumption of High-Sucrose Diet Has a Pro-Oxidant Effect and Alters the Function of the Salivary Glands of Rats. Nutrients 2018, 10, 1530. [Google Scholar] [CrossRef] [Green Version]
- Flynn, J.T.; Daniels, S.R.; Hayman, L.L.; Maahs, D.M.; McCrindle, B.W.; Mitsnefes, M.; Zachariah, J.P.; Urbina, E.M. Update: Ambulatory Blood Pressure Monitoring in Children and Adolescents. Hypertension 2014, 63, 1116–1135. [Google Scholar] [CrossRef]
- Kułaga, Z.; Litwin, M.; Grajda, A.; Kułaga, K.; Gurzkowska, B.; Góźdź, M.; Pan, H.; Rybi-Szumińska, A.; Szumiński, M.; Taranta-Janusz, K.; et al. Oscillometric blood pressure percentiles for Polish normal-weight school-aged children and adolescents. J. Hypertens. 2012, 30, 1942–1954. [Google Scholar] [CrossRef] [PubMed]
- Wühl, E.; Witte, K.; Soergel, M.; Mehls, O.; Schaefer, F. Distribution of 24-h ambulatory blood pressure in children: Normalized reference values and role of body dimensions. J. Hypertens 2002, 20, 1995–2007. [Google Scholar] [CrossRef] [PubMed]
- Urbina, E.; Alpert, B.; Flynn, J.; Hayman, L.; Harshfield, G.A.; Jacobson, M.; Mahoney, L.; McCrindle, B.; Mietus-Snyder, M.; Steinberger, J.; et al. Ambulatory Blood Pressure Monitoring in Children and Adolescents: Recommendations for Standard Assessment. Hypertension 2008, 52, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Falkner, B.; Daniels, S.R.; Flynn, J.T.; Gidding, S.; Green, L.A.; Ingelfinger, J.R.; Lauer, R.M.; Morgenstern, B.Z.; Portman, R.J.; Prineas, R.J.; et al. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar] [CrossRef] [Green Version]
- Saleh, J.; Figueiredo, M.A.Z.; Cherubini, K.; Salum, F.G. Salivary hypofunction: An update on aetiology, diagnosis and therapeutics. Arch. Oral Biol. 2015, 60, 242–255. [Google Scholar] [CrossRef]
- Yuan, A.; Woo, S.-B. Adverse drug events in the oral cavity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 35–47. [Google Scholar] [CrossRef] [Green Version]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The lms method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef]
- De Onis, M. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Int. J. Paediatr. 2006, 95, 76–85. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Zalewska, A.; Ładny, J.R. Salivary Antioxidant Barrier, Redox Status, and Oxidative Damage to Proteins and Lipids in Healthy Children, Adults, and the Elderly. Oxid. Med. Cell. Longev. 2019, 2019, 4393460. [Google Scholar] [CrossRef] [Green Version]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Flisiak, I.; Kołodziej, J.K.U.; Kotowska-Rodziewicz, A.; Klimiuk, A.; Zalewska, A. Enhanced Inflammation and Nitrosative Stress in the Saliva and Plasma of Patients with Plaque Psoriasis. J. Clin. Med. 2020, 9, 745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Kossakowska, A.; Szulimowska, J.; Klimiuk, A.; Knaś, M.; Car, H.; Niklińska, W.; Ładny, J.R.; Chabowski, A.; Zalewska, A. Lysosomal Exoglycosidase Profile and Secretory Function in the Salivary Glands of Rats with Streptozotocin-Induced Diabetes. J. Diabetes Res. 2017, 2017, 9850398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013; p. 1. [Google Scholar]
- Żukowski, P.; Maciejczyk, M.; Waszkiel, D. Sources of free radicals and oxidative stress in the oral cavity. Arch. Oral Biol. 2018, 92, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Lozano, P.; Henrikson, N.B.; Morrison, C.C.; Dunn, J.; Nguyen, M.; Blasi, P.R.; Whitlock, E.P. Lipid Screening in Childhood and Adolescence for Detection of Multifactorial Dyslipidemia. JAMA 2016, 316, 634. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Auinger, P.; Huang, T.T.K. Growth Curves for Cardio-Metabolic Risk Factors in Children and Adolescents. J. Pediatr. 2009, 155, S6–e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Screening for obesity in children and adolescents us preventive services task force recommendation statement. JAMA 2017, 317, 2417–2426. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Munoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New Equations to Estimate GFR in Children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar]
- Aebi, H. Catalase in Vitro. Methods Enzymol. 1984, 105, 121–126. [Google Scholar]
- Mansson-Rahemtulla, B.; Baldone, D.C.; Pruitt, K.M.; Rahemtulla, F. Specific assays for peroxidases in human saliva. Arch. Oral Biol. 1986, 31, 661–668. [Google Scholar] [CrossRef]
- Paglia, D.E.; Valentine, W.N. Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J. Lab. Clin. Med. 1967, 70, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Ellman, G.L. Tissue sulfhydryl groups. Arch. Biochem. Biophys. 1959, 82, 70–77. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Erel, O. A new automated colorimetric method for measuring total oxidant status. Clin. Biochem. 2005, 38, 1103–1111. [Google Scholar] [CrossRef]
- Żebrowska, E.; Maciejczyk, M.; Żendzian-Piotrowska, M.; Zalewska, A.; Chabowski, A. High Protein Diet Induces Oxidative Stress in Rat Cerebral Cortex and Hypothalamus. Int. J. Mol. Sci. 2019, 20, 1547. [Google Scholar] [CrossRef] [Green Version]
- Kalousová, M.; Skrha, J.; Zima, T. Advanced glycation end-products and advanced oxidation protein products in patients with diabetes mellitus. Physiol. Res. 2002, 51, 597–604. [Google Scholar]
- Maciejczyk, M.; Heropolitanska-Pliszka, E.; Pietrucha, B.; Sawicka-Powierza, J.; Bernatowska, E.; Wolska-Kusnierz, B.; Pac, M.; Car, H.; Zalewska, A.; Mikoluc, B. Antioxidant Defense, Redox Homeostasis, and Oxidative Damage in Children With Ataxia Telangiectasia and Nijmegen Breakage Syndrome. Front. Immunol. 2019, 10, 2322. [Google Scholar] [CrossRef]
- Buege, J.A.; Aust, S.D. Microsomal Lipid Peroxidation. Methods Enzymol. 1978, 52, 302–310. [Google Scholar]
- Grisham, M.B.; Johnson, G.G.; Lancaster, J.R. Quantitation of nitrate and nitrite in extracellular fluids. Methods Enzymol. 1996, 268, 237–246. [Google Scholar] [CrossRef]
- Borys, J.; Maciejczyk, M.; Antonowicz, B.; Sidun, J.; Świderska, M.; Zalewska, A. Free Radical Production, Inflammation and Apoptosis in Patients Treated With Titanium Mandibular Fixations—An Observational Study. Front. Immunol. 2019, 10, 2662. [Google Scholar] [CrossRef] [PubMed]
- Beckman, J.S.; Ischiropoulos, H.; Zhu, L.; van der Woerd, M.; Smith, C.; Chen, J.; Harrison, J.; Martin, J.C.; Tsai, M. Kinetics of superoxide dismutase- and iron-catalyzed nitration of phenolics by peroxynitrite. Arch. Biochem. Biophys. 1992, 298, 438–445. [Google Scholar] [CrossRef]
- Takimoto, E.; Kass, D.A. Role of Oxidative Stress in Cardiac Hypertrophy and Remodeling. Hypertension 2007, 49, 241–248. [Google Scholar] [CrossRef]
- Lushchak, V.I. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Biol. Interact. 2014, 224, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Gersch, C.; Palii, S.P.; Imaram, W.; Kim, K.M.; Karumanchi, S.A.; Angerhofer, A.; Johnson, R.J.; Henderson, G.N. Reactions of peroxynitrite with uric acid: Formation of reactive intermediates, alkylated products and triuret, and in vivo production of triuret under conditions of oxidative stress. Nucleosides Nucleotides Nucleic Acids 2009, 28, 118–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knaś, M.; Maciejczyk, M.; Waszkiel, D.; Zalewska, A. Oxidative stress and salivary antioxidants. Dent. Med. Probl. 2013, 50, 461–466. [Google Scholar]
- Sautin, Y.Y.; Johnson, R.J. Uric Acid: The Oxidant-Antioxidant Paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Higashi, Y.; Noma, K.; Yoshizumi, M.; Kihara, Y. Endothelial function and oxidative stress in cardiovascular diseases. Circ. J. 2009, 73, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Escobales, N.; Crespo, M. Oxidative-Nitrosative Stress In Hypertension. Curr. Vasc. Pharmacol. 2005. [Google Scholar] [CrossRef]
- Scirè, A.; Cianfruglia, L.; Minnelli, C.; Bartolini, D.; Torquato, P.; Principato, G.; Galli, F.; Armeni, T. Glutathione compartmentalization and its role in glutathionylation and other regulatory processes of cellular pathways. BioFactors 2019, 45, 152–168. [Google Scholar] [CrossRef]
- Alvarez, B.; Radi, R. Peroxynitrite reactivity with amino acids and proteins. Amino Acids 2003, 25, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Proctor, G.B.; Carpenter, G.H. Regulation of salivary gland function by autonomic nerves. Auton. Neurosci. 2007, 133, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Looms, D.; Tritsaris, K.; Pedersen, A.M.; Nauntofte, B.; Dissing, S. Nitric oxide signalling in salivary glands. J. Oral Pathol. Med. 2002, 31, 569–584. [Google Scholar] [CrossRef] [PubMed]
- Klimiuk, A.; Zalewska, A.; Sawicki, R.; Knapp, M.; Maciejczyk, M. Salivary Oxidative Stress Increases With the Progression of Chronic Heart Failure. J. Clin. Med. 2020, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawczuk, B.; Maciejczyk, M.; Sawczuk-Siemieniuk, M.; Posmyk, R.; Zalewska, A.; Car, H. Salivary Gland Function, Antioxidant Defence and Oxidative Damage in the Saliva of Patients with Breast Cancer: Does the BRCA1 Mutation Disturb the Salivary Redox Profile? Cancers 2019, 11, 1501. [Google Scholar] [CrossRef] [Green Version]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Fejfer, K.; Krahel, J.; Flisiak, I.; Kołodziej, U.; Zalewska, A. Salivary Antioxidants and Oxidative Stress in Psoriatic Patients: Can Salivary Total Oxidant Status and Oxidative Status Index Be a Plaque Psoriasis Biomarker? Oxid. Med. Cell. Longev. 2020, 2020, 9086024. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.; Nair, B. Comparative analysis of the oxidative stress and antioxidant status in type II diabetics and nondiabetics: A biochemical study. J. Oral Maxillofac. Pathol. 2017, 21, 394. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control n = 53 | Hypertension n = 53 | ||
|---|---|---|---|
| General Data | |||
| Age (years) | 13 ± 3.1 | 13 ± 3.5 | |
| Male n (%) | 28 (53%) | 28 (53%) | |
| BMI (kg/m2) | 22 ± 2.6 | 26 ± 5.9 * | |
| SDS BMI | 0.8 ± 0.2 | 2.4 ± 0.5 | |
| Obesity n (%) | 0 (0) | 20 (38%) | |
| Blood Pressure | |||
| SBP (mmHg) | 106 ± 10.5 | 124 ± 12 * | |
| DBP (mmHg) | 65 ± 8 | 76 ± 9.5 * | |
| Blood Tests | |||
| WBC (tys./μL) | 7.5 ± 0.9 | 6.8 ± 1.7 | |
| RBC (tys./μL) | 4.3 ± 0.5 | 4.3 ± 0.2 | |
| Hgb (g/dL) | 14 ± 0.9 | 14 ± 1.3 | |
| Hct (%) | 43 ± 2.6 | 42 ± 3.7 | |
| PLT (tys./μL) | 250 ± 65 | 274 ± 60 | |
| sCre (mg/dL) | 0.73 ± 0.5 | 0.73 ± 0.4 | |
| sUrea (mg/dL) | 15 ± 10 | 25 ± 11 | |
| HDL (mg/dL) | 52 ± 10 | 48 ± 12 | |
| LDL (mg/dL) | 70 ± 25 | 97 ± 24 * | |
| TC (mg/dL) | 167 ± 45 | 177 ± 74 | |
| TG (mg/dL) | 70 ± 38 | 122 ± 72 * | |
| Glucose (mg/dL) | 82 ± 5.5 | 89 ± 7.9 | |
| IL-6 (pg/mL) | 1.44 ± 0.57 | 2.49 ± 0.58 * | |
| eGFR (mL/min/1.73m2) | 140 ± 29 | 118 ± 38 | |
| Pharmacotherapy | |||
| Hypotensive drugs | 0 per day n (%) | 0 (0) | 22 (39) |
| 1 per day n (%) | 0 (0) | 24 (45) | |
| 2 per day n (%) | 0 (0) | 7 (13) | |
| Angiotensin-converting enzyme inhibitors n (%) | 0 (0) | 21 (40) | |
| Angiotensin receptor blockers n (%) | 0 (0) | 5 (9) | |
| Calcium channel blockers n (%) | 0 (0) | 4 (7) | |
| 24 h SBP (mmHg) | 127 ± 11 |
| 24 h DBP (mmHg) | 69 ± 7.5 |
| SBP daytime (mmHg) | 130 ± 11 |
| DBP daytime (mmHg) | 72 ± 7.6 |
| SBP nighttime (mmHg) | 117 ± 11 |
| DBP nighttime (mmHg) | 72 ± 16 |
| SBPL daytime (%) | 51 ± 3.7 |
| DBPL daytime (%) | 19 ± 3.0 |
| SBPL nighttime (%) | 47 ± 4.6 |
| DBPL nighttime (%) | 20 ± 2.8 |
| SBP 24 h Z-score | 0.21 ± 5.9 |
| DBP 24 h Z-score | 0.25 ± 2.2 |
| SBP day Z-score | 0.91 ± 2.5 |
| DBP day Z-score | 136 ± 675 |
| SBP night Z-score | -7 ± 20 |
| DBP night Z-score | -7.9 ± 29 |
| Control n = 53 | Hypertension n = 53 | |
|---|---|---|
| NWS flow (mL/min) | 0.47 ± 0.05 | 0.43 ± 0.05 |
| SWS flow (mL/min) | 1.8 ± 0.09 | 0.89 ± 0.09 * |
| TP NWS (μg/mL) | 1350 ± 185 | 1330 ± 264 |
| TP SWS (μg/mL) | 1019 ± 217 | 772 ± 228 * |
| α-amylase NWS (μmol/mg protein) | 0.2 ± 0.08 | 0.19 ± 0.08 |
| α-amylase SWS (μmol/mg protein) | 0.28 ± 0.05 | 0.21 ± 0.08 * |
| DMFT | 3.1 ± 0.1 | 3.1 ± 0.2 |
| dmft | 11 ± 0.1 | 11.1 ± 0.1 |
| PBI | 0 ± 0.1 | 0 ± 0.1 |
| GI | 0 ± 0.1 | 0 ± 0.1 |
| Pair of Variables | r | p |
|---|---|---|
| SWS | ||
| CAT and SOD | 0.32 | 0.028 |
| Saliva and blood | ||
| AGE NWS and AGE plasma | 0.83 | <0.001 |
| MDA NWS and MDA plasma | 0.83 | <0.001 |
| Pair of Variables | r | p |
|---|---|---|
| NWS | ||
| SOD and TOS | 0.83 | <0.001 |
| MDA and SBP | 0.64 | <0.001 |
| MDA and SBP | 0.49 | 0.001 |
| SWS | ||
| CAT and TOS | 0.75 | <0.001 |
| UA and TOS | 0.62 | <0.001 |
| UA and DBP | 0.8 | <0.001 |
| AGE and SBP | 0.64 | <0.001 |
| AGE and DBP | 0.5 | 0.001 |
| MDA and SBP | 0.6 | <0.001 |
| MDA and DBP | 0.31 | 0.025 |
| UA and DBP | 0.8 | <0.001 |
| UA and DBP 24 h Z-score | 0.35 | 0.016 |
| UA and SBP 24 h Z-score | 0.41 | 0.004 |
| GSH and Peroxynitrite | -0.61 | <0.001 |
| Peroxynitrite and MDA | 0.61 | <0.001 |
| Peroxynitrite and nitrotyrosine | 0.68 | <0.001 |
| SWS flow and MDA | −0.77 | <0.001 |
| SWS flow and NO | 0.56 | <0.001 |
| SWS flow and peroxynitrite | −0.42 | 0.002 |
| SWS flow and nitrotyrosine | −0.41 | 0.002 |
| Saliva and blood | ||
| AGE NWS and AGE plasma | 0.8 | <0.001 |
| MDA NWS and MDA plasma | 0.89 | <0.001 |
| UA SWS and IL-6 | 0.72 | <0.001 |
| AUC | Confidence Intervals | p Value | Cut-off | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|---|---|---|
| NWS | ||||||
| SOD (mU/mg protein) | 0.91 | 0.86–0.96 | <0.001 | >1.65 | 77 | 83 |
| CAT (nmol H2O2/min/mg protein) | 0.68 | 0.58–0.78 | 0.002 | >0.52 | 64 | 66 |
| Px (mU/mg protein) | 0.55 | 0.43–0.67 | 0.406 | >0.49 | 55 | 64 |
| GSH (µg/mg protein) | 0.87 | 0.80–0.94 | <0.001 | <0.43 | 79 | 79 |
| UA (µg/mg protein) | 0.85 | 0.77–0.92 | <0.001 | >3.35 | 72 | 79 |
| TAC (µmol/mg protein) | 0.83 | 0.74–0.92 | <0.001 | >0.59 | 77 | 82 |
| TOS (nmol H2O2 equiv/mg protein) | 0.87 | 0.79–0.95 | <0.001 | >10.30 | 81 | 87 |
| OSI (TOS/TAC ratio) | 0.58 | 0.47–0.68 | 0.186 | >13.45 | 57 | 55 |
| AGE (AFU/mg protein) | 0.96 | 0.92–1.00 | <0.001 | >2.08 | 92 | 92 |
| MDA (µmol/mg protein) | 0.79 | 0.70–0.87 | <0.001 | >101.3 | 75 | 74 |
| NO (nmol/mg protein) | 0.63 | 0.52–0.73 | 0.026 | <180.6 | 62 | 58 |
| Peroxynitrite (pmol/mg protein) | 0.79 | 0.69–0.89 | <0.001 | >63.47 | 75 | 77 |
| Nitrotyrosine (pmol/mg protein) | 0.63 | 0.53–0.74 | 0.018 | >221.3 | 64 | 60 |
| SWS | ||||||
| SOD (mU/mg protein) | 0.74 | 0.65–0.84 | <0.001 | >3.72 | 74 | 70 |
| CAT (nmol H2O2/min/mg protein) | 0.93 | 0.87–0.98 | <0.001 | >5.11 | 91 | 91 |
| Px (mU/mg protein) | 0.79 | 0.70–0.88 | <0.001 | >0.47 | 77 | 72 |
| GSH (µg/mg protein) | 0.79 | 0.70–0.88 | <0.001 | <0.70 | 70 | 70 |
| UA (µg/mg protein) | 0.98 | 0.96–1.00 | <0.001 | >5.50 | 94 | 96 |
| TAC (µmol/mg protein) | 0.80 | 0.71–0.88 | <0.001 | >0.82 | 74 | 75 |
| TOS (nmol H2O2 equiv/mg protein) | 0.61 | 0.50–0.72 | 0.055 | >19.37 | 55 | 58 |
| OSI (TOS/TAC ratio) | 0.64 | 0.53–0.74 | 0.015 | <22.30 | 58 | 55 |
| AGE (AFU/mg protein) | 0.99 | 0.97–1.00 | <0.001 | >4.64 | 92 | 92 |
| MDA (µmol/mg protein) | 0.80 | 0.72–0.89 | <0.001 | >68.72 | 77 | 74 |
| NO (nmol/mg protein) | 0.83 | 0.75–0.91 | <0.001 | <197.7 | 74 | 77 |
| Peroxynitrite (pmol/mg protein) | 0.84 | 0.76–0.92 | <0.001 | >72.86 | 83 | 79 |
| Nitrotyrosine (pmol/mg protein) | 0.72 | 0.62–0.82 | 0.001 | >204.5 | 66 | 66 |
| AUC | Confidence Intervals | p Value | Cut-off | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|---|---|---|
| Erythrocytes | ||||||
| SOD (mU/mg protein) | 0.89 | 0.83–0.96 | <0.001 | >0.37 | 83 | 83 |
| CAT (nmol H2O2/min/mg protein) | 0.85 | 0.77–0.92 | <0.001 | >0.43 | 79 | 79 |
| GPx (mU/mg protein) | 1.00 | 1.00–1.00 | <0.001 | >0.23 | 100 | 98 |
| Plasma | ||||||
| GSH (µg/mg protein) | 0.70 | 0.59–0.80 | 0.001 | <3.19 | 64 | 68 |
| UA (µg/mg protein) | 0.68 | 0.58–0.78 | 0.002 | >0.81 | 64 | 66 |
| TAC (µmol/mg protein) | 0.85 | 0.77–0.94 | <0.001 | >0.62 | 81 | 85 |
| TOS (nmol H2O2 equiv/mg protein) | 0.76 | 0.67–0.86 | <0.001 | >7.95 | 77 | 74 |
| OSI (TOS/TAS ratio) | 0.57 | 0.46–0.68 | 0.226 | >13.45 | 57 | 55 |
| AGE (AFU/mg protein) | 1.00 | 1.00–1.00 | <0.001 | >3.96 | 98 | 100 |
| MDA (µmol/mg protein) | 0.90 | 0.84–0.97 | <0.001 | >103.7 | 85 | 92 |
| NO (nmol/mg protein) | 0.82 | 0.73–0.91 | <0.001 | <16.66 | 77 | 79 |
| Peroxynitrite (pmol/mg protein) | 0.78 | 0.68–0.87 | <0.001 | >86.27 | 72 | 74 |
| Nitrotyrosine (pmol/mg protein) | 0.67 | 0.57–0.77 | 0.003 | >166.2 | 68 | 64 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maciejczyk, M.; Taranta-Janusz, K.; Wasilewska, A.; Kossakowska, A.; Zalewska, A. A Case-Control Study of Salivary Redox Homeostasis in Hypertensive Children. Can Salivary Uric Acid be a Marker of Hypertension? J. Clin. Med. 2020, 9, 837. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030837
Maciejczyk M, Taranta-Janusz K, Wasilewska A, Kossakowska A, Zalewska A. A Case-Control Study of Salivary Redox Homeostasis in Hypertensive Children. Can Salivary Uric Acid be a Marker of Hypertension? Journal of Clinical Medicine. 2020; 9(3):837. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030837
Chicago/Turabian StyleMaciejczyk, Mateusz, Katarzyna Taranta-Janusz, Anna Wasilewska, Agnieszka Kossakowska, and Anna Zalewska. 2020. "A Case-Control Study of Salivary Redox Homeostasis in Hypertensive Children. Can Salivary Uric Acid be a Marker of Hypertension?" Journal of Clinical Medicine 9, no. 3: 837. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030837