
The Role of the Adipokine Resistin in the Pathogenesis and Progression of Epithelial Ovarian Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. The Link between Obesity and EOC
3. Biological Functions of Resistin
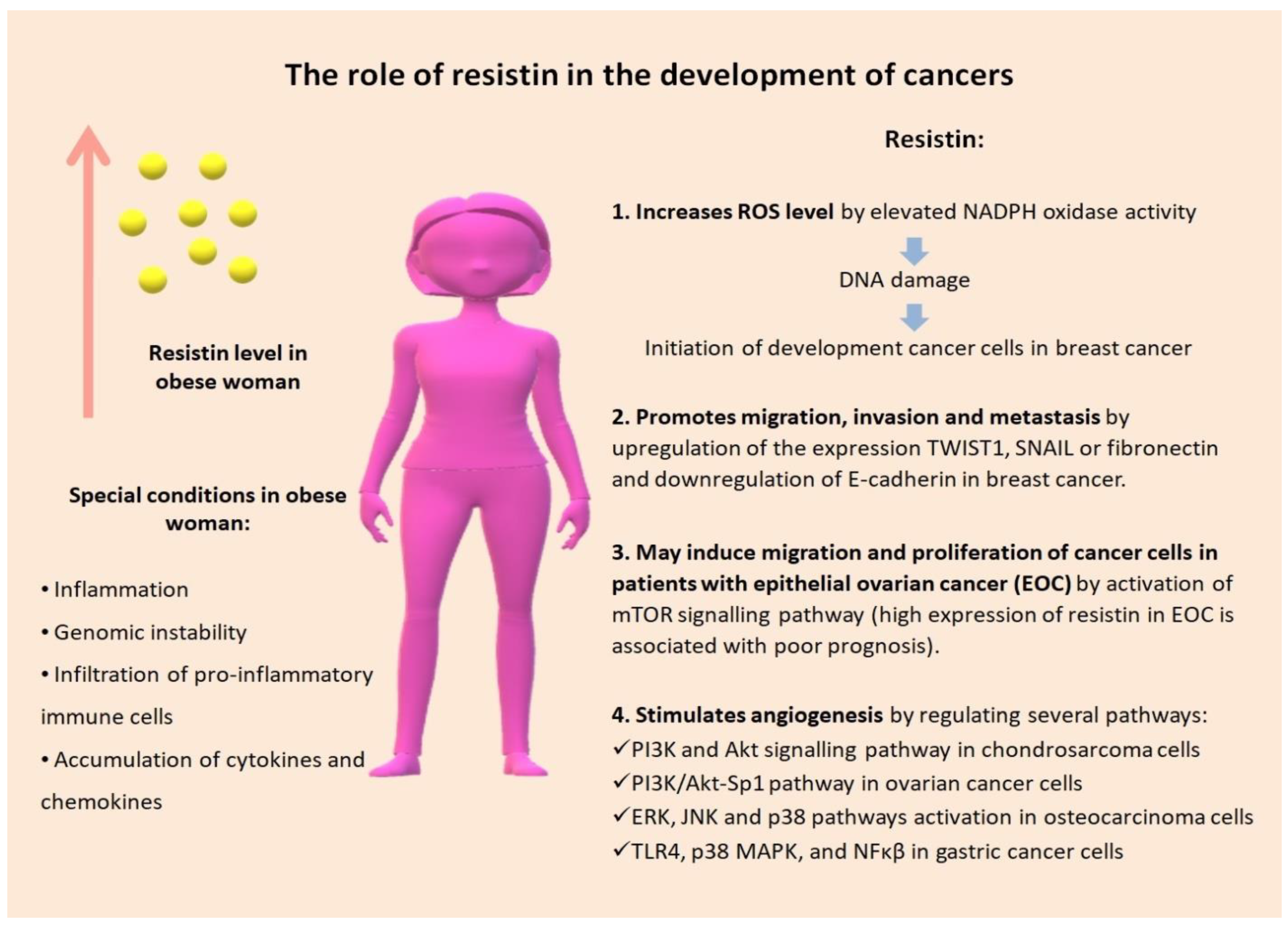
- the PI3K–Akt signaling pathway in chondrosarcoma cells, through downregulation of microRNA expression (miR)–16–5p [96];
- the PI3K–Akt–Sp1 pathway in ovarian cancer cells (HO-8910) through increasing the interaction with Specificity protein 1 (Sp1), triggering progressive phosphorylation of Sp1 on Thr453 and Thr739 [97];
- ERK, c-Jun N-terminal kinase (JNK), and p38 pathways activation in osteocarcinoma cells [98];
4. The Role and Significance of Resistin in the Biology and Progression of Epithelial Ovarian Cancer
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, F.; Jin, F.; Peng, S.; Li, C.; Wang, L.; Wang, S. Adipocyte-Derived CCDC3 Promotes Tumorigenesis in Epithelial Ovarian Cancer Through the Wnt/ß-Catenin Signalling Pathway. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Kossaï, M.; Leary, A.; Scoazec, J.-Y.; Genestie, C. Ovarian Cancer: A Heterogeneous Disease. Pathobiology 2018, 85, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.L.; Laios, A.; Jackson, D.; Nugent, D.; Orsi, N.M.; Theophilou, G.; Thangavelu, A.; de Jong, D. The Uncertain Benefit of Adjuvant Chemotherapy in Advanced Low-Grade Serous Ovarian Cancer and the Pivotal Role of Surgical Cytoreduction. J. Clin. Med. 2021, 10, 5927. [Google Scholar] [CrossRef]
- De Leo, A.; Santini, D.; Ceccarelli, C.; Santandrea, G.; Palicelli, A.; Acquaviva, G.; Chiarucci, F.; Rosini, F.; Ravegnini, G.; Pession, A.; et al. What Is New on Ovarian Carcinoma: Integrated Morphologic and Molecular Analysis Following the New 2020 World Health Organization Classification of Female Genital Tumors. Diagnostics 2021, 11, 697. [Google Scholar] [CrossRef]
- Moch, H. Female Genital Tumours: WHO Classification of Tumours. In WHO Classification of Tumours, 5th ed.; World Health Organization: Geneva, Switzerland, 2020; Volume 4. [Google Scholar]
- Kurman, R.J.; Shih, I.-M. The Dualistic Model of Ovarian Carcinogenesis: Revisited, Revised, and Expanded. Am. J. Pathol. 2016, 186, 733–747. [Google Scholar] [CrossRef] [Green Version]
- Kujawa, K.A.; Lisowska, K.M. [Ovarian cancer—from biology to clinic]. Postepy Hig. Med. Dosw. 2015, 69, 1275–1290. [Google Scholar] [CrossRef]
- Kurman, R.J.; Shih, I.-M. The Origin and Pathogenesis of Epithelial Ovarian Cancer: A Proposed Unifying Theory. Am. J. Surg. Pathol. 2010, 34, 433–443. [Google Scholar] [CrossRef] [Green Version]
- Kurman, R.J.; Shih, I.-M. Pathogenesis of Ovarian Cancer: Lessons from Morphology and Molecular Biology and Their Clinical Implications. Int. J. Gynecol. Pathol. 2008, 27, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Darb-Esfahani, S.; Kolaschinski, I.; Trillsch, F.; Mahner, S.; Concin, N.; Vergote, I.; Van Nieuwenhuysen, E.; Achimas-Cadariu, P.; Glajzer, J.; Woopen, H.; et al. Morphology and Tumour-Infiltrating Lymphocytes in High-Stage, High-Grade Serous Ovarian Carcinoma Correlated with Long-Term Survival. Histopathology 2018, 73, 1002–1012. [Google Scholar] [CrossRef]
- Ducie, J.; Dao, F.; Considine, M.; Olvera, N.; Shaw, P.A.; Kurman, R.J.; Shih, I.-M.; Soslow, R.A.; Cope, L.; Levine, D.A. Molecular Analysis of High-Grade Serous Ovarian Carcinoma with and without Associated Serous Tubal Intra-Epithelial Carcinoma. Nat. Commun. 2017, 8, 990. [Google Scholar] [CrossRef] [PubMed]
- Rabban, J.T.; Garg, K.; Crawford, B.; Chen, L.; Zaloudek, C.J. Early Detection of High-Grade Tubal Serous Carcinoma in Women at Low Risk for Hereditary Breast and Ovarian Cancer Syndrome by Systematic Examination of Fallopian Tubes Incidentally Removed during Benign Surgery. Am. J. Surg. Pathol. 2014, 38, 729–742. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Benson, J.L.; Gan, C.; Anglesio, M.; Arora, R.; Faruqi, A.Z.; Hirschowitz, L.; Kommoss, F.; Scott, K.; Trevisan, G.; et al. Disease Distribution in Low-Stage Tubo-Ovarian High-Grade Serous Carcinoma (HGSC): Implications for Assigning Primary Site and FIGO Stage. Int. J. Gynecol. Pathol. 2018, 37, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Sherman-Baust, C.A.; Kuhn, E.; Valle, B.L.; Shih, I.-M.; Kurman, R.J.; Wang, T.-L.; Amano, T.; Ko, M.S.H.; Miyoshi, I.; Araki, Y.; et al. A Genetically Engineered Ovarian Cancer Mouse Model Based on Fallopian Tube Transformation Mimics Human High-Grade Serous Carcinoma Development. J. Pathol. 2014, 233, 228–237. [Google Scholar] [CrossRef]
- Zhu, X.; Lang, J. Soluble PD-1 and PD-L1: Predictive and Prognostic Significance in Cancer. Oncotarget 2017, 8, 97671–97682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basta, A.; Bidziński, M.; Bieńkiewicz, A.; Blecharz, P.; Bodnar, L.; Jach, R.; Knapp, P.; Kojs, Z.; Kotarski, J.; Markowska, J.; et al. Recommendations of the Polish Gynecological Oncology Society for the diagnosis and treatment of ovarian cancer. Curr. Gynecol. Oncol. 2017, 15, 5–23. [Google Scholar] [CrossRef]
- Webb, P.M.; Jordan, S.J. Epidemiology of Epithelial Ovarian Cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 41, 3–14. [Google Scholar] [CrossRef] [Green Version]
- La Vecchia, C. Ovarian Cancer: Epidemiology and Risk Factors. Eur. J. Cancer Prev. 2017, 26, 55–62. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and Cancer Risk: Emerging Biological Mechanisms and Perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef]
- Kolb, R.; Sutterwala, F.S.; Zhang, W. Obesity and Cancer: Inflammation Bridges the Two. Curr. Opin. Pharmacol. 2016, 29, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. International Agency for Research on Cancer Handbook Working Group Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Metzinger, M.N.; Lewellen, K.A.; Cripps, S.N.; Carey, K.D.; Harper, E.I.; Shi, Z.; Tarwater, L.; Grisoli, A.; Lee, E.; et al. Obesity Contributes to Ovarian Cancer Metastatic Success through Increased Lipogenesis, Enhanced Vascularity, and Decreased Infiltration of M1 Macrophages. Cancer Res. 2015, 75, 5046–5057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caballero, B. Humans against Obesity: Who Will Win? Adv. Nutr. 2019, 10, S4–S9. [Google Scholar] [CrossRef] [PubMed]
- Polsky, S.; Ellis, S.L. Obesity, Insulin Resistance, and Type 1 Diabetes Mellitus. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 277–282. [Google Scholar] [CrossRef]
- Alpert, M.A.; Karthikeyan, K.; Abdullah, O.; Ghadban, R. Obesity and Cardiac Remodeling in Adults: Mechanisms and Clinical Implications. Prog. Cardiovasc. Dis. 2018, 61, 114–123. [Google Scholar] [CrossRef]
- Naik, A.; Monjazeb, A.M.; Decock, J. The Obesity Paradox in Cancer, Tumor Immunology, and Immunotherapy: Potential Therapeutic Implications in Triple Negative Breast Cancer. Front. Immunol. 2019, 10, 1–12. [Google Scholar]
- Góralska, M.; Majewska-Szczepanik, M.; Szczepanik, M. Immunological mechanisms involved in obesity and their role in metabolic syndrome. Postepy. Hig. Med. Dosw. 2015, 69, 1384–1404. [Google Scholar]
- Gupta, M.; Babic, A.; Beck, A.H.; Terry, K. TNF-α Expression, Risk Factors, and Inflammatory Exposures in Ovarian Cancer: Evidence for an Inflammatory Pathway of Ovarian Carcinogenesis? Hum. Pathol. 2016, 54, 82–91. [Google Scholar] [CrossRef] [Green Version]
- Chechlinska, M.; Kowalewska, M.; Nowak, R. Systemic Inflammation as a Confounding Factor in Cancer Biomarker Discovery and Validation. Nat. Rev. Cancer 2010, 10, 2–3. [Google Scholar] [CrossRef]
- Pang, L.; Chang, X. Resistin Expression in Epithelial Ovarian Cancer Promotes the Proliferation and Migration of Ovarian Cancer Cells to Worsen Prognosis. J. Cancer 2021, 12, 6796–6804. [Google Scholar] [CrossRef]
- Rak, A.; Drwal, E.; Wróbel, A.; Gregoraszczuk, E.Ł. Resistin Is a Survival Factor for Porcine Ovarian Follicular Cells. Reproduction 2015, 150, 343–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, L.; Zhang, G.-F.; Yu, L.; Wang, H.-Y.; Jia, X.-J.; Wang, T.-J. Novel Oncogenic and Chemoresistance-Inducing Functions of Resistin in Ovarian Cancer Cells Require MiRNAs-Mediated Induction of Epithelial-to-Mesenchymal Transition. Sci. Rep. 2018, 8, 12522. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Salmeri, F.M.; Ban Frangež, H.; Ghezzi, F.; Vrtačnik-Bokal, E.; Granese, R. Evaluation of M1 and M2 Macrophages in Ovarian Endometriomas from Women Affected by Endometriosis at Different Stages of the Disease. Gynecol. Endocrinol. 2020, 36, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Vankerckhoven, A.; Wouters, R.; Mathivet, T.; Ceusters, J.; Baert, T.; Van Hoylandt, A.; Gerhardt, H.; Vergote, I.; Coosemans, A. Opposite Macrophage Polarization in Different Subsets of Ovarian Cancer: Observation from a Pilot Study. Cells 2020, 9, E305. [Google Scholar] [CrossRef] [Green Version]
- López-Janeiro, Á.; Padilla-Ansala, C.; de Andrea, C.E.; Hardisson, D.; Melero, I. Prognostic Value of Macrophage Polarization Markers in Epithelial Neoplasms and Melanoma. A Systematic Review and Meta-Analysis. Mod. Pathol. 2020, 33, 1458–1465. [Google Scholar] [CrossRef]
- Ye, J.; McGuinness, O.P. Inflammation during Obesity Is Not All Bad: Evidence from Animal and Human Studies. Am. J. Physiol. Endocrinol. Metab. 2013, 304, E466–477. [Google Scholar] [CrossRef] [Green Version]
- Dieli-Conwright, C.M.; Parmentier, J.-H.; Sami, N.; Lee, K.; Spicer, D.; Mack, W.J.; Sattler, F.; Mittelman, S.D. Adipose Tissue Inflammation in Breast Cancer Survivors: Effects of a 16-Week Combined Aerobic and Resistance Exercise Training Intervention. Breast Cancer Res. Treat. 2018, 168, 147–157. [Google Scholar] [CrossRef]
- Kessous, R.; Davidson, E.; Meirovitz, M.; Sergienko, R.; Sheiner, E. Prepregnancy Obesity: A Risk Factor for Future Development of Ovarian and Breast Cancer. Eur. J. Cancer Prev. 2017, 26, 151–155. [Google Scholar] [CrossRef]
- Huang, T.; Tworoger, S.S.; Willett, W.C.; Stampfer, M.J.; Rosner, B.A. Associations of Early Life and Adulthood Adiposity with Risk of Epithelial Ovarian Cancer. Ann. Oncol. 2019, 30, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Tworoger, S.S.; Huang, T. Obesity and Ovarian Cancer. In Obesity and Cancer; Pischon, T., Nimptsch, K., Eds.; Recent Results in Cancer Research; Springer International Publishing: Cham, Switzerland, 2016; Volume 208, pp. 155–176. ISBN 978-3-319-42540-5. [Google Scholar]
- Foong, K.W.; Bolton, H. Obesity and Ovarian Cancer Risk: A Systematic Review. Post. Reprod. Health 2017, 23, 183–198. [Google Scholar] [CrossRef]
- Zhang, Y.; Coletta, A.M.; Allen, P.K.; Parikh, A.M.; Cox-Mattin, M.; Meyer, L.A.; Sun, C.C.; Basen-Engquist, K.M.; Lu, K.H.; Klopp, A.H. Perirenal Adiposity Is Associated With Lower Progression-Free Survival From Ovarian Cancer. Int. J. Gynecol. Cancer 2018, 28, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Purcell, S.A.; Elliott, S.A.; Kroenke, C.H.; Sawyer, M.B.; Prado, C.M. Impact of Body Weight and Body Composition on Ovarian Cancer Prognosis. Curr. Oncol. Rep. 2016, 18, 8. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.M.; Green, A.C.; Whiteman, D.C.; Sadeghi, S.; Kolahdooz, F.; Webb, P.M. Obesity and the Risk of Epithelial Ovarian Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2007, 43, 690–709. [Google Scholar] [CrossRef] [PubMed]
- Bae, H.S.; Kim, H.J.; Hong, J.H.; Lee, J.K.; Lee, N.W.; Song, J.Y. Obesity and Epithelial Ovarian Cancer Survival: A Systematic Review and Meta-Analysis. J. Ovarian Res. 2014, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Tanha, K.; Mottaghi, A.; Nojomi, M.; Moradi, M.; Rajabzadeh, R.; Lotfi, S.; Janani, L. Investigation on Factors Associated with Ovarian Cancer: An Umbrella Review of Systematic Review and Meta-Analyses. J. Ovarian Res. 2021, 14, 153. [Google Scholar] [CrossRef]
- Nagle, C.M.; Dixon, S.C.; Jensen, A.; Kjaer, S.K.; Modugno, F.; deFazio, A.; Fereday, S.; Hung, J.; Johnatty, S.E.; Australian Ovarian Cancer Study Group; et al. Obesity and Survival among Women with Ovarian Cancer: Results from the Ovarian Cancer Association Consortium. Br. J. Cancer 2015, 113, 817–826. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Woo, Y.C.; Wang, Y.; Yeung, C.Y.; Xu, A.; Lam, K.S.L. Obesity, Adipokines and Cancer: An Update. Clin. Endocrinol. 2015, 83, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Surmi, B.K.; Hasty, A.H. Macrophage Infiltration into Adipose Tissue. Future Lipidol. 2008, 3, 545–556. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.; Apovian, C.M. Macrophage Functions in Lean and Obese Adipose Tissue. Metabolism 2017, 72, 120–143. [Google Scholar] [CrossRef]
- Cozzo, A.J.; Fuller, A.M.; Makowski, L. Contribution of Adipose Tissue to Development of Cancer. Compr. Physiol. 2017, 8, 237–282. [Google Scholar] [CrossRef]
- Lee, Y.S.; Olefsky, J. Chronic Tissue Inflammation and Metabolic Disease. Genes. Dev. 2021, 35, 307–328. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.R.; Milner, J.J.; Makowski, L. The Inflammation Highway: Metabolism Accelerates Inflammatory Traffic in Obesity. Immunol. Rev. 2012, 249, 218–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLean, P.S.; Higgins, J.A.; Giles, E.D.; Sherk, V.D.; Jackman, M.R. The Role for Adipose Tissue in Weight Regain after Weight Loss. Obes. Rev. 2015, 16, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Taylor, E.B. The Complex Role of Adipokines in Obesity, Inflammation, and Autoimmunity. Clin. Sci. 2021, 135, 731–752. [Google Scholar] [CrossRef]
- Deng, T.; Lyon, C.J.; Bergin, S.; Caligiuri, M.A.; Hsueh, W.A. Obesity, Inflammation, and Cancer. Annu. Rev. Pathol. 2016, 11, 421–449. [Google Scholar] [CrossRef] [Green Version]
- Zorena, K.; Jachimowicz-Duda, O.; Ślęzak, D.; Robakowska, M.; Mrugacz, M. Adipokines and Obesity. Potential Link to Metabolic Disorders and Chronic Complications. Int. J. Mol. Sci. 2020, 21, 3570. [Google Scholar] [CrossRef]
- Rajesh, Y.; Sarkar, D. Association of Adipose Tissue and Adipokines with Development of Obesity-Induced Liver Cancer. Int. J. Mol. Sci. 2021, 22, 2163. [Google Scholar] [CrossRef]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity with Survival Outcomes in Patients with Cancer: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef]
- Wang, Y.-Y.; Hung, A.C.; Lo, S.; Yuan, S.-S.F. Adipocytokines Visfatin and Resistin in Breast Cancer: Clinical Relevance, Biological Mechanisms, and Therapeutic Potential. Cancer Lett. 2021, 498, 229–239. [Google Scholar] [CrossRef]
- Ho, G.Y.F.; Wang, T.; Gunter, M.J.; Strickler, H.D.; Cushman, M.; Kaplan, R.C.; Wassertheil-Smoller, S.; Xue, X.; Rajpathak, S.N.; Chlebowski, R.T.; et al. Adipokines Linking Obesity with Colorectal Cancer Risk in Postmenopausal Women. Cancer Res. 2012, 72, 3029–3037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieman, K.M.; Romero, I.L.; Van Houten, B.; Lengyel, E. Adipose Tissue and Adipocytes Support Tumorigenesis and Metastasis. Biochim. Biophys. Acta 2013, 1831, 1533–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.K.; Ahima, R.S. Resistin in Rodents and Humans. Diabetes Metab. J. 2013, 37, 404–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jasińska, A.; Pietruczuk, M. Adipocytokines – proteins of multidirectional function. Diagn. Lab. 2010, 46, 331–338. [Google Scholar]
- Wertel, I.; Suszczyk, D.; Pawłowska, A.; Bilska, M.; Chudzik, A.; Skiba, W.; Paduch, R.; Kotarski, J. Prognostic and Clinical Value of Interleukin 6 and CD45+CD14+ Inflammatory Cells with PD-L1+/PD-L2+ Expression in Patients with Different Manifestation of Ovarian Cancer. J. Immunol. Res. 2020, 2020, 1715064. [Google Scholar] [CrossRef]
- Piao, J.; Lee, E.J.; Lee, M. Association between Pelvic Inflammatory Disease and Risk of Ovarian Cancer: An Updated Meta-Analysis. Gynecol. Oncol. 2020, 157, 542–548. [Google Scholar] [CrossRef]
- Okła, K.; Czerwonka, A.; Wawruszak, A.; Bobiński, M.; Bilska, M.; Tarkowski, R.; Bednarek, W.; Wertel, I.; Kotarski, J. Clinical Relevance and Immunosuppressive Pattern of Circulating and Infiltrating Subsets of Myeloid-Derived Suppressor Cells (MDSCs) in Epithelial Ovarian Cancer. Front. Immunol. 2019, 10, 691. [Google Scholar] [CrossRef] [Green Version]
- Wertel, I.; Okła, K.; Surówka, J.; Bilska, M.; Polak, G.; Bednarek, W.; Kotarski, J. Why ovarian cancer cells escape from immune surveillance? Wiad. Lek. 2017, 70, 74–80. [Google Scholar]
- Jung, H.S.; Park, K.-H.; Cho, Y.M.; Chung, S.S.; Cho, H.J.; Cho, S.Y.; Kim, S.J.; Kim, S.Y.; Lee, H.K.; Park, K.S. Resistin Is Secreted from Macrophages in Atheromas and Promotes Atherosclerosis. Cardiovasc. Res. 2006, 69, 76–85. [Google Scholar] [CrossRef]
- Acquarone, E.; Monacelli, F.; Borghi, R.; Nencioni, A.; Odetti, P. Resistin: A Reappraisal. Mech. Ageing Dev. 2019, 178, 46–63. [Google Scholar] [CrossRef]
- Amato, M.C.; Pizzolanti, G.; Torregrossa, V.; Misiano, G.; Milano, S.; Giordano, C. Visceral Adiposity Index (VAI) Is Predictive of an Altered Adipokine Profile in Patients with Type 2 Diabetes. PLoS ONE 2014, 9, e91969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsuk, E.; Kubiak, J.Z. In Vitro Culture of Mouse Oocytes for Meiotic Maturation. Methods Mol. Biol. 2018, 1818, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Kwak, M.K.; Kim, H.J.; Ahima, R.S. Linking Resistin, Inflammation, and Cardiometabolic Diseases. Korean J. Intern. Med. 2017, 32, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.R.; Lazar, M.A. Human Resistin: Found in Translation from Mouse to Man. Trends Endocrinol. Metab. 2011, 22, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Lee, H.-C.; Kwon, Y.-W.; Lee, S.E.; Cho, Y.; Kim, J.; Lee, S.; Kim, J.-Y.; Lee, J.; Yang, H.-M.; et al. Adenylyl Cyclase-Associated Protein 1 Is a Receptor for Human Resistin and Mediates Inflammatory Actions of Human Monocytes. Cell. Metab. 2014, 19, 484–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, Y.-Y.; Shen, C.-H.; Huang, W.-S.; Chin, C.-C.; Kuo, Y.-H.; Hsieh, M.C.; Yu, H.-R.; Chang, T.-S.; Lin, T.-H.; Chiu, Y.-W.; et al. Resistin-Induced Stromal Cell-Derived Factor-1 Expression through Toll-like Receptor 4 and Activation of P38 MAPK/ NFκB Signaling Pathway in Gastric Cancer Cells. J. Biomed. Sci. 2014, 21, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudan, S.K.; Deshmukh, S.K.; Poosarla, T.; Holliday, N.P.; Dyess, D.L.; Singh, A.P.; Singh, S. Resistin: An Inflammatory Cytokine with Multi-Faceted Roles in Cancer. Biochim. Biophys. Acta Rev. Cancer 2020, 1874, 188419. [Google Scholar] [CrossRef]
- Gherman, C.; Braicu, O.L.; Zanoaga, O.; Jurj, A.; Pileczki, V.; Maralani, M.; Drigla, F.; Braicu, C.; Budisan, L.; Achimas-Cadariu, P.; et al. Caffeic Acid Phenethyl Ester Activates Pro-Apoptotic and Epithelial-Mesenchymal Transition-Related Genes in Ovarian Cancer Cells A2780 and A2780cis. Mol. Cell Biochem. 2016, 413, 189–198. [Google Scholar] [CrossRef]
- Al Hannan, F.; Culligan, K.G. Human Resistin and the RELM of Inflammation in Diabesity. Diabetol. Metab. Syndr. 2015, 7, 54. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Yang, Q.; Cai, D.; Guo, H.; Fang, J.; Cui, H.; Gou, L.; Deng, J.; Wang, Z.; Zuo, Z. Resistin, a Novel Host Defense Peptide of Innate Immunity. Front. Immunol. 2021, 12, 1–14. [Google Scholar]
- Son, Y.M.; Ahn, S.M.; Kim, G.R.; Moon, Y.S.; Kim, S.H.; Park, Y.-M.; Lee, W.K.; Min, T.S.; Han, S.H.; Yun, C.-H. Resistin Enhances the Expansion of Regulatory T Cells through Modulation of Dendritic Cells. BMC Immunol. 2010, 11, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, L.; Yu, Y.; Wang, L.; Zhu, Z.; Lu, R.; Yao, Z. Hypoxia-Induced CCL28 Promotes Recruitment of Regulatory T Cells and Tumor Growth in Liver Cancer. Oncotarget 2016, 7, 75763–75773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Nola, R.; Menga, A.; Castegna, A.; Loizzi, V.; Ranieri, G.; Cicinelli, E.; Cormio, G. The Crowded Crosstalk between Cancer Cells and Stromal Microenvironment in Gynecological Malignancies: Biological Pathways and Therapeutic Implication. Int. J. Mol. Sci. 2019, 20, E2401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wertel, I.; Surówka, J.; Polak, G.; Barczyński, B.; Bednarek, W.; Jakubowicz-Gil, J.; Bojarska-Junak, A.; Kotarski, J. Macrophage-Derived Chemokine CCL22 and Regulatory T Cells in Ovarian Cancer Patients. Tumour Biol. 2015, 36, 4811–4817. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, D.; Kant, S.; Pandey, S.; Ehtesham, N.Z. Resistin in Metabolism, Inflammation, and Disease. FEBS J. 2020, 287, 3141–3149. [Google Scholar] [CrossRef]
- Rubio-Guerra, A.F.; Cabrera-Miranda, L.J.; Vargas-Robles, H.; Maceda-Serrano, A.; Lozano-Nuevo, J.J.; Escalante-Acosta, B.A. Correlation between Levels of Circulating Adipokines and Adiponectin/Resistin Index with Carotid Intima-Media Thickness in Hypertensive Type 2 Diabetic Patients. Cardiology 2013, 125, 150–153. [Google Scholar] [CrossRef]
- Singh, S.; Chouhan, S.; Mohammad, N.; Bhat, M.K. Resistin Causes G1 Arrest in Colon Cancer Cells through Upregulation of SOCS3. FEBS Lett. 2017, 591, 1371–1382. [Google Scholar] [CrossRef] [Green Version]
- Deb, A.; Deshmukh, B.; Ramteke, P.; Bhati, F.K.; Bhat, M.K. Resistin: A Journey from Metabolism to Cancer. Transl. Oncol. 2021, 14, 101178. [Google Scholar] [CrossRef]
- Assiri, A.M.A.; Kamel, H.F.M.; Hassanien, M.F.R. Resistin, Visfatin, Adiponectin, and Leptin: Risk of Breast Cancer in Pre- and Postmenopausal Saudi Females and Their Possible Diagnostic and Predictive Implications as Novel Biomarkers. Dis. Markers 2015, 2015, 1–9. [Google Scholar] [CrossRef]
- Zhao, C.-C.; Chen, J.; Niu, R.-F.; Liu, Y.; Zhang, C.-G. Increased Resistin Suggests Poor Prognosis and Promotes Development of Lung Adenocarcinoma. Oncol. Rep. 2018, 40, 3392–3404. [Google Scholar] [CrossRef]
- Bonaventura, A.; Grossi, F.; Carbone, F.; Vecchié, A.; Minetti, S.; Bardi, N.; Elia, E.; Ansaldo, A.M.; Ferrara, D.; Rijavec, E.; et al. Resistin Is Associated with Overall Survival in Non-Small Cell Lung Cancer Patients during Nivolumab Treatment. Clin. Transl. Oncol. 2020, 22, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-H.; Wang, P.-J.; Hsieh, Y.-C.; Lo, S.; Lee, Y.-C.; Chen, Y.-C.; Tsai, C.-H.; Chiu, W.-C.; Chu-Sung Hu, S.; Lu, C.-W.; et al. Resistin Facilitates Breast Cancer Progression via TLR4-Mediated Induction of Mesenchymal Phenotypes and Stemness Properties. Oncogene 2018, 37, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Hlavna, M.; Kohut, L.; Lipkova, J.; Bienertova-Vasku, J.; Dostalova, Z.; Chovanec, J.; Vasku, A. Relationship of Resistin Levels with Endometrial Cancer Risk. Neoplasma 2011, 58, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-S.; Tang, C.-H.; Chie, M.-J.; Tsai, C.-H.; Fong, Y.-C.; Lu, Y.-C.; Chen, W.-C.; Lai, C.-T.; Wei, C.-Y.; Tai, H.-C.; et al. Resistin Facilitates VEGF-A-Dependent Angiogenesis by Inhibiting MiR-16-5p in Human Chondrosarcoma Cells. Cell Death Dis. 2019, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Pang, L.; Zhang, Y.; Yu, Y.; Zhang, S. Resistin Promotes the Expression of Vascular Endothelial Growth Factor in Ovary Carcinoma Cells. Int. J. Mol. Sci. 2013, 14, 9751–9766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.-C.; Cheng, S.-P.; Han, C.-K.; Huang, Y.-L.; Wang, S.-W.; Lee, J.-J.; Lai, C.-T.; Fong, Y.-C.; Tang, C.-H. Resistin Enhances Angiogenesis in Osteosarcoma via the MAPK Signaling Pathway. Aging 2019, 11, 9767–9777. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Fu, G.; Dai, T.; Huang, H. Migration of Endothelial Progenitor Cells Mediated by Stromal Cell-Derived Factor-1alpha/CXCR4 via PI3K/Akt/ENOS Signal Transduction Pathway. J. Cardiovasc. Pharmacol. 2007, 50, 274–280. [Google Scholar] [CrossRef]
- Holm, J.B.; Rosendahl, A.H.; Borgquist, S. Local Biomarkers Involved in the Interplay between Obesity and Breast Cancer. Cancers 2021, 13, 6286. [Google Scholar] [CrossRef]
- Kulbe, H.; Iorio, F.; Chakravarty, P.; Milagre, C.S.; Moore, R.; Thompson, R.G.; Everitt, G.; Canosa, M.; Montoya, A.; Drygin, D.; et al. Integrated Transcriptomic and Proteomic Analysis Identifies Protein Kinase CK2 as a Key Signaling Node in an Inflammatory Cytokine Network in Ovarian Cancer Cells. Oncotarget 2016, 7, 15648–15661. [Google Scholar] [CrossRef]
- Nomelini, R.S.; Borges Júnior, L.E.; de Lima, C.A.; Chiovato, A.F.C.; Micheli, D.C.; Tavares-Murta, B.M.; Murta, E.F.C. TNF-R2 in Tumor Microenvironment as Prognostic Factor in Epithelial Ovarian Cancer. Clin. Exp. Med. 2018, 18, 547–554. [Google Scholar] [CrossRef]
- Xie, Q.; Cheng, Z.; Chen, X.; Lobe, C.G.; Liu, J. The Role of Notch Signalling in Ovarian Angiogenesis. J. Ovarian Res. 2017, 10, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.-J.; Pena, G.N.A.; Pradeep, S.; Cho, M.S.; Coleman, R.L.; Sood, A.K. Anti-Vascular Therapies in Ovarian Cancer: Moving beyond Anti-VEGF Approaches. Cancer Metastasis Rev. 2015, 34, 19–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santilli, F.; Liani, R.; Di Fulvio, P.; Formoso, G.; Simeone, P.; Tripaldi, R.; Ueland, T.; Aukrust, P.; Davì, G. Increased Circulating Resistin Is Associated with Insulin Resistance, Oxidative Stress and Platelet Activation in Type 2 Diabetes Mellitus. Thromb. Haemost. 2016, 116, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Miyoshi, K.; Claudio, E.; Siebenlist, U.K.; Gonzalez, F.J.; Flaws, J.; Wagner, K.-U.; Hennighausen, L. Loss of the Peroxisome Proliferation-Activated Receptor Gamma (PPARgamma) Does Not Affect Mammary Development and Propensity for Tumor Formation but Leads to Reduced Fertility. J. Biol. Chem. 2002, 277, 17830–17835. [Google Scholar] [CrossRef] [Green Version]
- Dupont, J.; Reverchon, M.; Cloix, L.; Froment, P.; Ramé, C. Involvement of Adipokines, AMPK, PI3K and the PPAR Signaling Pathways in Ovarian Follicle Development and Cancer. Int. J. Dev. Biol. 2012, 56, 959–967. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | Odds Ratio (95 % CI) |
|---|---|
| P16INK4a | 2.657 (1.173–6.014) |
| Polycystic ovarian syndrome | 1.580 (1.081–2.310) |
| Endometriosis | 1.433 (1.294–1.586) |
| Obesity | 1.274 (1.194–1.36) |
| Hormone therapy (estrogen-progestin) | 1.190 (1.043–1.357) |
| Overweight | 1.079 (1.041–1.119) |
| BRCA2 N372H rs144848 | 1.079 (1.018–1.143) |
| MTHFR C677T | 1.077 (1.032–1.124) |
| Recreational physical activity | 0.830 (0.745–0.925) |
| Oral contraceptive | 0.655 (0.515–0.833) |
| Breast feeding | 0.719 (0.679–0.762) |
| Differences in the Functioning of Adipose Tissue | Lean | Obese |
|---|---|---|
| Immune Cell Populations | ILC2s, Tregs, eosinophils, type II NKT and Th2 cells, and M2-like macrophages | Th1, NK, CD8+ T cells, adipocyte MHC II, M1-like macrophages |
| Cytokines | IL-4, IL-5, IL-10, IL-13, IL-25, IL-33 | IL-1β, IL-6, TNFα, IFN-γ |
| Adipokines | Adiponectin, Sfrp5 | Leptin |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parafiniuk, K.; Skiba, W.; Pawłowska, A.; Suszczyk, D.; Maciejczyk, A.; Wertel, I. The Role of the Adipokine Resistin in the Pathogenesis and Progression of Epithelial Ovarian Cancer. Biomedicines 2022, 10, 920. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040920
Parafiniuk K, Skiba W, Pawłowska A, Suszczyk D, Maciejczyk A, Wertel I. The Role of the Adipokine Resistin in the Pathogenesis and Progression of Epithelial Ovarian Cancer. Biomedicines. 2022; 10(4):920. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040920
Chicago/Turabian StyleParafiniuk, Klaudia, Wiktoria Skiba, Anna Pawłowska, Dorota Suszczyk, Aleksandra Maciejczyk, and Iwona Wertel. 2022. "The Role of the Adipokine Resistin in the Pathogenesis and Progression of Epithelial Ovarian Cancer" Biomedicines 10, no. 4: 920. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040920